A seven-year-old girl with Down syndrome was incidentally found to have abnormal chest radiograph finding. She had no history of fever, dyspnea, hemoptysis, or features of upper airway obstruction. There was no significant family history or contact with tuberculosis. Oxygen saturation in room air was 97%. Normal vesicular breath sounds were heard bilaterally on examination of the chest.
Her chest radiograph [Figure 1] and computed tomography [Figure 2 and 3] of the chest are given below.
Question
What is the diagnosis?
Answer
Subpleural cysts of Down syndrome.
Discussion
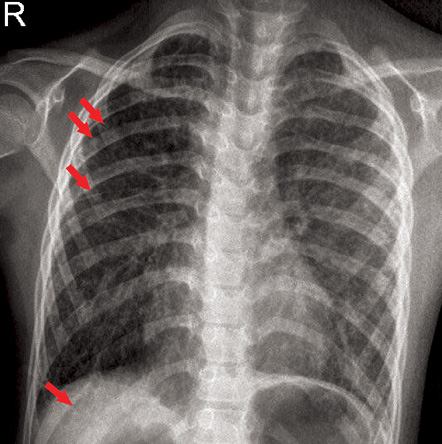
Figure 1: Chest radiograph of a seven-year-old girl, anteroposterior view.
Chest radiograph showed hyperinflated lungs with bilateral diffuse reticulonodular interstitial opacities and small cystic lucencies [Figure 1, arrows] in the lung bases. Computed tomography (CT) of the lungs showed multiple air filled cystic lucencies [Figure 2 and 3, arrows] in both lungs with a subpleural and basal predominant distribution. These findings were consistent with subpleural cysts of Down syndrome.
Subpleural cysts are small cystic dilatations along the subpleural surface of the lung. The first association of this finding with Down syndrome was reported in 1986 in two infants who were found to have cystic lung disease on autopsy.1 Gonzalez et al,2 reported a prevalence of 20% in an autopsy series of 98 patients with Down syndrome. Biko et al,3 found a prevalence of 36% in a review of the CT scans of 25 children with Down syndrome.
The etiology of these cysts is unknown, but they are thought to be related to pulmonary hypoplasia, which is a feature of Down syndrome. Children with Down syndrome have a diminished number of alveoli, a smaller alveolar surface area, and enlarged alveoli and alveolar ducts.4
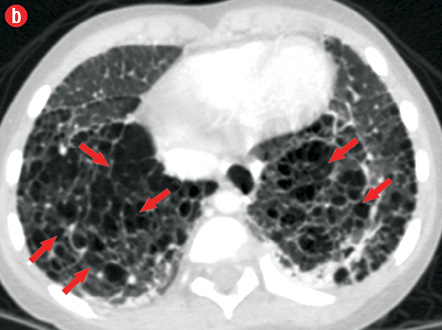
Figure 2: Axial computed tomography images of the chest at the level of (a) upper lobes and (b) lower lobes.
These cysts are not well appreciated on plain chest radiographs. Gyves-Ray et al,5 reported a child with Down syndrome in whom extensive cystic lung disease was discovered incidentally on CT when the chest radiograph had failed to demonstrate the finding. The same author then reviewed chest radiographs of 45 children with Down syndrome, and only one (1.8%) showed cystic lung disease. However, CT examination of these children was not performed.5
To the best of our knowledge, there are no published reports of extensive lung involvement obvious on plain radiograph. Biko et al,3 in his series of nine cases, reported that cysts were found in the anteromedial portion of the lung in the majority while two of these children had cysts extending along the bronchovascular bundles into deeper lung tissue. The finding of subpleural cysts in Down syndrome should be distinguished from Langerhans cell histiocytosis and pneumatoceles. In pulmonary Langerhans cell histiocytosis, lesions have variable appearance depending on the stage of disease, ranging from small peribronchiolar nodular opacities to multiple irregularly shaped cysts. These cysts have middle and upper zone predilection.6
Subpleural cysts in Down syndrome have only limited or no clinical significance. They are usually incidental finding on chest CT and can usually be managed with close observation.7
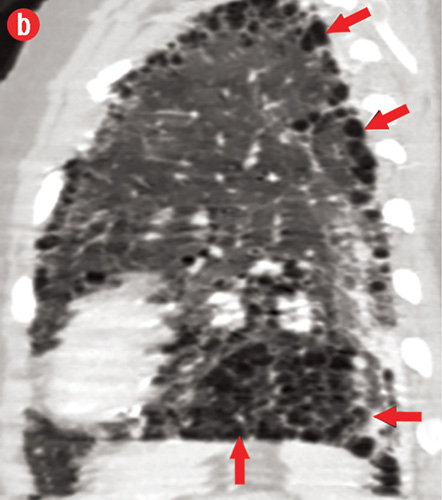
Figure 3: (a) Coronal and (b) sagittal computed tomography images of chest.
Conclusion
Subpleural cysts are common finding in Down syndrome, which may be incidentally noted on CT scan images, but rarely can be seen on chest radiograph. These cystic spaces are secondary to the hypoplasia of the lung in Down syndrome and further diagnostic work-up is not routinely needed.
Disclosure
The authors declared no conflicts of interest.
references
- Joshi VV, Kasznica J, Ali Khan MA, Amato JJ, Levine OR. Cystic lung disease in Down’s syndrome: a report of two cases. Pediatr Pathol 1986;5(1):79-86.
- Gonzalez OR, Gomez IG, Recalde AL, Landing BH. Postnatal development of the cystic lung lesion of Down syndrome: suggestion that the cause is reduced formation of peripheral air spaces. Pediatr Pathol 1991 Jul-Aug;11(4):623-633.
- Biko DM, Schwartz M, Anupindi SA, Altes TA. Subpleural lung cysts in Down syndrome: prevalence and association with coexisting diagnoses. Pediatr Radiol 2008 Mar;38(3):280-284.
- Cooney TP, Thurlbeck WM. Pulmonary hypoplasia in Down’s syndrome. N Engl J Med 1982 Nov;307(19):1170-1173.
- Gyves-Ray K, Kirchner S, Stein S, Heller R, Hernanz-Schulman M. Cystic lung disease in Down syndrome.Pediatr Radiol 1994;24(2):137-138.
- Abbott GF, Rosado-de-Christenson ML, Franks TJ, Frazier AA, Galvin JR. From the archives of the AFIP: pulmonary Langerhans cell histiocytosis. Radiographics 2004 May-Jun;24(3):821-841.
- McDowell KM, Craven DI. Pulmonary complications of Down syndrome during childhood. J Pediatr 2011 Feb;158(2):319-325.