Inflammatory pseudotumors (IPTs) are defined as mass-like lesions of unknown etiology with histological features of nonspecific inflammation and mesenchymal proliferation. Although originally detected and most commonly found in the lung, IPTs have been reported in various other sites as well, including the eye orbit, respiratory tract, digestive system, bladder, heart, soft tissues, lymph nodes, liver, mesothelial membranes, and spleen.1-3 IPT of the spleen represents an extremely rare lesion and are most frequently detected incidentally. A diagnosis in the majority of reported cases is made after splenectomy, since IPT of the spleen has often been misdiagnosed as a splenic neoplasm both clinically and radiologically.4 Here we report a case of a 19-year-old male who was diagnosed with a splenic malignancy before surgery.
Case Report
A 19-year-old male presented to the outpatient surgery department of the Hamdard Institute of Medical Sciences and Research and associated Hakeem Abdul Hameed Centenary Hospital, Hamdard University, New Delhi. He had a history of pain and heaviness in the left hypochondrium for the last six to eight months. There were no other associated symptoms (e.g., fever, chills, loss of appetite, or weight loss). Physical examination revealed a moderate degree of splenomegaly. A complete blood count showed mild anemia with 80% neutrophils on differential leukocyte count. All other parameters were within normal range. The biochemical tests were also within normal limits. The serological tests for malaria, Kala Azar, and hydatid disease also turned out to be negative, thus excluding an infectious etiology for the enlarged spleen.
Ultrasonography imaging revealed an enlarged spleen with a large, round, and heterogeneous mass at the lower pole of the spleen with central hyperechoic areas. The mass measured 9.6 × 8.8 cm. Contrast-enhanced computed tomography revealed an enlarged spleen with a poorly defined, round, hypodense lesion measuring 10.7 × 8 × 8.2 cm with extensive coarse calcification, completely occupying the lower pole of the spleen and producing a bulge in the splenic contour. Minimal enhancement on contrast was noted. This led to a clinical diagnosis of splenomegaly with a splenic mass lesion, suggestive of malignancy.
An open splenectomy was done, and the specimen was sent for histopathological examination. On gross examination, a resected specimen of the spleen with intact capsule was received, measuring 15 ×
10 × 7 cm. The weight of the spleen was 957 g. Serial sections revealed a well-circumscribed nodular growth measuring 9 × 8 × 5 cm in diameter on the lower pole of the spleen. The cut section of the growth showed tan white solid areas with foci of yellowish discoloration [Figure 1].
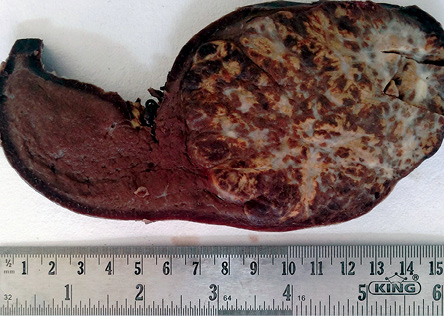
Figure 1: Gross examination: cut section of the splenic lesion showing well-circumscribed growth with tan white solid areas and foci of yellowish discoloration.
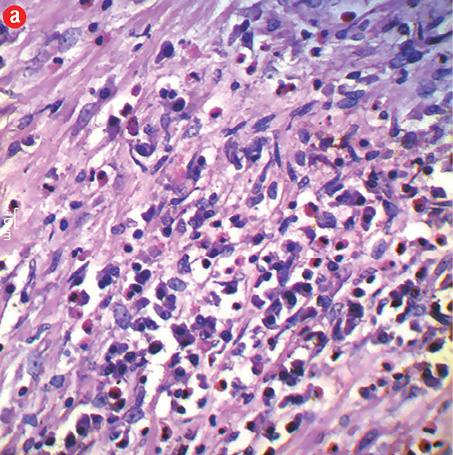
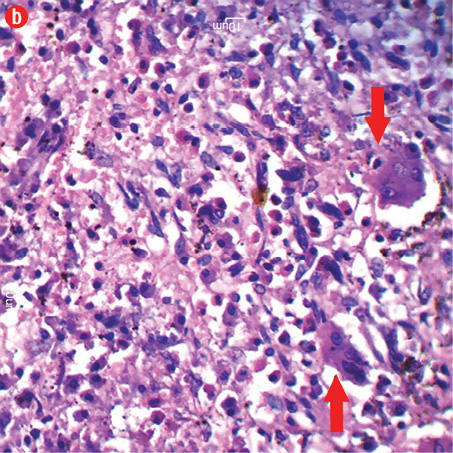
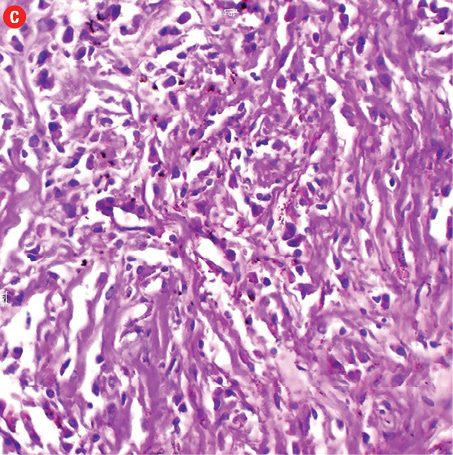
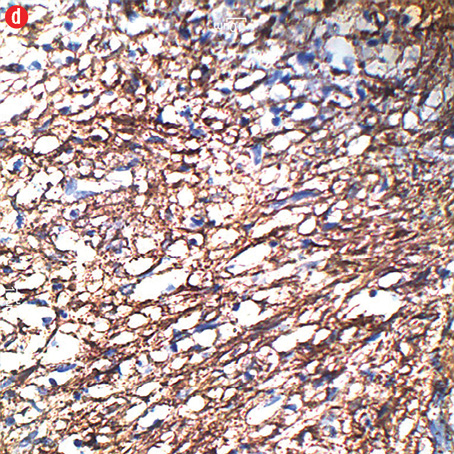
Microscopic examination of the nodular growth showed spindle cells in a hyalinized stroma with inflammatory infiltration of predominantly plasma cells and lymphocytes along with few neutrophils and eosinophils [Figure 2a and 2c]. Multinucleated foreign body giant cells, hemosiderin laden histiocytes, and areas of hemorrhage were also seen [Figure 2b]. The spindle cells were positive for smooth muscle actin [Figure 2d]. Adjacent splenic tissue was compressed. No atypia or mitotic activity was noted. Thus, a diagnosis of IPT of the spleen was made based on the histology findings.
|
|
|
|
|
|
|
|
|
Figure 2: Hematoxylin and eosin staining. (a) Proliferation of spindle cells along with admixture of inflammatory cells, including lymphocytes, plasma cells, and eosinophils. Magnification = 400 ×. (b) Polymorphous inflammatory cells, mainly plasma cells, lymphocytes, eosinophils and multinucleated foreign body giant cells (arrow). Magnification = 400 ×. (c) Proliferation of spindle cells in a hyalinized stroma was visible. Magnification = 100 ×. (d) Immunohistochemical staining showing spindle cells positive for smooth muscle actin. Magnification = 100 ×. |
The patient has been followed-up regularly and has remained asymptomatic for the last six months.
Discussion
The term inflammatory pseudotumor was coined by Umiker et al in 1954.5 The first case of IPT of the spleen was reported by Cotelingam and Jaffe in 1984.6 They categorized the lesion as a “spectrum of non-neoplastic, inflammatory, and reparative changes”. Only about 115 cases have been reported in the medical literature since that time.7
IPTs of the spleen are very rare lesions and in the majority of cases they are detected as an incidental finding. The rarity of this lesion is also suggested by the fact that overall incidence of primary benign splenic tumors is only 0.007%.8 The differential diagnosis of IPT of the spleen includes both benign as well as malignant splenic lesions. The benign lesions include splenic cyst, abscess, organizing hematoma, hamartoma, hemangioma, lymphangioma, lipoma, and fibroma. The malignant differentials include malignant lymphoma, hemangiosarcoma, malignant fibrous histiocytoma, fibrosarcoma, and metastatic cancers.7-9
Patients are typically asymptomatic in most cases. The symptomatic patient usually presents with left upper quadrant abdominal pain or discomfort with or without fever or enlarged spleen.7 Our patient presented with pain and heaviness in the left hypochondrium with splenomegaly. Fine needle aspiration cytology or needle biopsy can usually differentiate benign from malignant lesions. However, these modalities are usually not recommended for splenic lesions because of potential risk of bleeding, poor specificity, uncertainty of detecting the disease, and the risk of spillage of cells in malignant tumors.7,9 Histopathology of the resected specimen remains the gold standard for categorizing splenic masses.7
Although IPT has been reported to occur at diverse anatomic sites, virtually all IPTs share certain histological features. They are usually benign, solitary and well-circumscribed masses, composed microscopically in varying proportions of plump spindle cells along with polymorphous inflammatory cell infiltrate consisting mainly of lymphocytes, plasma cells, and histiocytes. Foreign body giant cells, hemosiderin laden macrophages, neutrophils, and eosinophils may also be seen.1,2 Immunohistochemically, the majority of the cases show positivity for smooth muscle actin and vimentin.1
Although the exact pathogenesis is still unknown, the various possibilities include infections (Mycobacterium, Ebstein-Barr virus, human immunodeficiency virus, etc.), vascular abnormalities, immunological derangements and neoplastic process.1,7 Matsubayashi et al,10 suggested the development of IPT of the spleen after rupture of splenic hemangioma while Gomez et al,11 suggested the role of human herpes virus-8 in the development of some pulmonary IPTs. Contrary to the claim made by different authors regarding benign or malignant nature of IPT of the spleen,12,13 the World Health Organization (WHO) has placed this entity between benign and malignant lesion and categorized its biological behavior in an intermediate category (rarely metastatizing, <5%).14 Various synonyms are also given for IPT of the spleen by the WHO, such as inflammatory myofibroblastic tumor, plasma cell granulomas, inflammatory myofibroblastic proliferation, plasma cell pseudotumor, and inflammatory fibrosarcoma.14
Splenectomy is both diagnostic as well as curative for this lesion, and to date no local recurrence, invasion or evidence of metastasis has been reported.
Conclusion
IPT of the spleen is a rare, benign tumor of unknown etiology with non-specific clinical features and is often detected as an incidental finding. Preoperative diagnosis of this entity is usually difficult. Splenectomy is curative and histopathological examination remains the gold standard for rendering the diagnosis.
Disclosure
The authors declared no conflicts of interest.
references
- 1. Lewis JT, Gaffney RL, Casey MB, Farrell MA, Morice WG, Macon WR. Inflammatory pseudotumor of the spleen associated with a clonal Epstein-Barr virus genome. Case report and review of the literature. Am J Clin Pathol 2003 Jul;120(1):56-61.
- 2. Oshiro H, Nomura M, Yamanaka S, Watanabe S, Inayama Y. Splenic inflammatory pseudotumor (inflammatory myofibroblastic tumor). J Clin Exp Hematop 2007 Nov;47(2):83-88.
- 3. Singh S, Chhabra S, Modi S, Marwah N, Rawal A, Arora B. Inflammatory psuedo-tumor of the spleen. Indian J Pathol Microbiol 2009 Oct-Dec;52(4):564-565.
- 4. Yan J, Peng C, Yang W, Wu C, Ding J, Shi T, et al. Inflammatory pseudotumour of the spleen: report of 2 cases and literature review. Can J Surg 2008 Feb;51(1):75-765
- Umiker WO, Iverson L. Postinflammatory tumors of the lung; report of four cases simulating xanthoma, fibroma, or plasma cell tumor. J Thorac Surg 1954 Jul;28(1):55-63.
- 6. Cotelingam JD, Jaffe ES. Inflammatory pseudotumor of the spleen. Am J Surg Pathol 1984 May;8(5):375-380.
- 7. Ma ZH, Tian XF, Ma J, Zhao YF. Inflammatory pseudotumor of the spleen: A case report and review of published cases. Oncol Lett 2013 Jun;5(6):1955-1957.
- 8. Tsugawa K, Hashizume M, Migou S, Kawanaka H, Sugimachi K, Irie H, et al. Laparoscopic splenectomy for an inflammatory pseudotumor of the spleen: operative technique and case report. Hepatogastroenterology 1998 Sep-Oct;45(23):1887-1891.
- 9. Chen WH, Liu TP, Liu CL, Tzen CY. Inflammatory pseudotumor of the spleen. J Chin Med Assoc 2004 Oct;67(10):533-536.
- 10. Matsubayashi H, Mizoue T, Mizuguchi Y, Shinohara Y, Magami Y, Horibe T, et al. A case of hemangioma accompanied by inflammatory pseudotumor of the spleen. J Clin Gastroenterol 2000 Oct;31(3):258-261.
- 11. Gomez-Roman JJ, Sanchez-Velasco P, Ocejo-Vinyals G. Hernandez –Nieto E, Levya-Cobian F, Val-Bernal JF. Human herpes virus-8 genes are expressed in pulmonary inflammatory myofibroblastic tumor (Inflammatory pseudotumor). Am J Surg Pathol 2001;25:624-629.
- 12. Coffin CM, Watterson J, Priest JR, Dehner LP. Extrapulmonary inflammatory myofibroblastic tumor (inflammatory pseudotumor). A clinicopathologic and immunohistochemical study of 84 cases. Am J Surg Pathol 1995 Aug;19(8):859-872.
- 13. Meis JM, Enzinger FM. Inflammatory fibrosarcoma of the mesentery and retroperitoneum. A tumor closely simulating inflammatory pseudotumor. Am J Surg Pathol 1991 Dec;15(12):1146-1156.
- 14. Fletcher CD, Unni KK, Merterns F, eds. Pathology and genetics of tumours of soft tissue and bone. World Health Organization classification of tumors. Lyon: IARC press; 2002.