|
|
Abstract
Pfeiffer syndrome is a rare genetic disorder with combination of bicoronal craniosynostosis, broad thumbs, broad great toes, ankylosis of elbow and partial variable syndactyly of the hands and feet. Since the disorder was reported by Pfeiffer in 1964, new associations have been added on. Authors report a newborn with features of Pfeiffer syndrome type 3 with hypothyroidism, tail like appendage and extremely anteriorly placed anus as new associations.
Keywords: Hypothyroidism; Neonate; Pfeiffer syndrome; Proptosis; Tail like appendage; New associations.
Introduction
Pfeiffer Syndrome is a genetic disorder, first described by a German geneticist, Rudolf Pfeiffer in 1964. The frequency of occurrence is about 1 in 100000 individuals. The characteristic features of the syndrome include craniosynostosis, broad thumbs, broad great toes, and occasionally a partial syndactyly involving the second and third digits.1-4 Three clinical subtypes and new findings have been described subsequently.3,4 The authors describe type 3 variety of the syndrome in a neonate with additional associations, which were not reported earlier.
Case Report
A female neonate born at term, to a 24-years old primigravida by elective lower segment cesarian section in view of antenatally detected ventriculomegaly, was referred to our centre at 4 hours of life. Parentage was non-consanguineous and there was no family history of craniosynostosis. Birth weight was 3185 grams, length 50cm and head circumference was 37.5cm. Anterior fontanel measured 2cm × 2cm, and posterior and lateral fontanels were open. Further examination in this propositus revealed bilateral extreme proptosis (Figs. 1A & B), hypertelorism, small nose, midface contraction, choanal stenosis on right side, bulky tongue, short neck, broad thumbs (Figure1C), medially rotated broad great toes (Fig. 1D), bilateral elbow ankylosis, extremely anteriorly placed anus close to vulva (Fig. 1E) and human tail like appendage. (Fig. 1F)
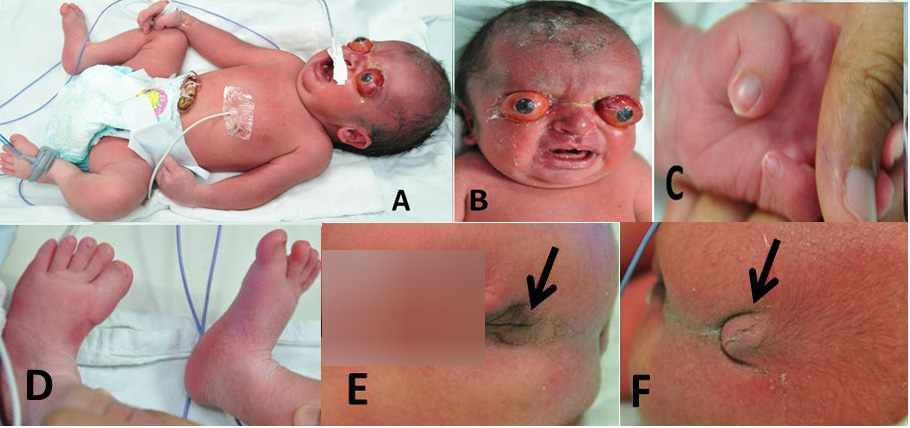
Figure 1:Extreme proptosis (A&B), hypertelorism, small nose, midface contraction (B), broad deviated thumbs (A,C), broad great toes (D), extremely anteriorly placed anus close to vulva (E) and human tail like appendage (F).
Investigation revealed T3 of 2.03ng/mL (normal: 4.04-7.04ng/mL), very high thyroid stimulating hormone (TSH) of >100 µIU/mL, (normal: 3-18 µIU/mL) and T4 of 11.2 µg/dL (normal: 10-16 µg/dL). Thyroid ultrasound scan and iodine scintigraphy were planned later. Complete blood count and renal functions were normal. Magnetic resonance imaging (MRI) of brain did not reveal any intracranial malformations. MRI of the orbit revealed shallow orbit and bilateral proptosis with preseptal edema, more on the left side (Fig. 2). Lens was normal in position and shape on both sides. Anterior chamber, posterior chamber, vitreous compartment, optic nerves, extra ocular muscles and intra orbital soft tissues were normal on both sides. Ultrasonography of the abdomen was normal. Echocardiography revealed 2 mm patent ductus arteriosus. Bilateral canthotomy, temporary tarsorrhaphy and Gunderson’s flap for right eye were performed. Neonate had stridor and required oropharyngeal airway for some days. Upper airway endoscopy revealed anteriorly placed vocal cords. She tolerated tube feeds well. L-thyroxine 10 µg/kg body weight per day was added. Ultrasonography of the lumbosacral region revealed a dermal appendage with no neural or bony components. Three weeks later TSH returned to normal levels (7.57µIU/ml). The patient was discharged with an advice to have close follow ups.
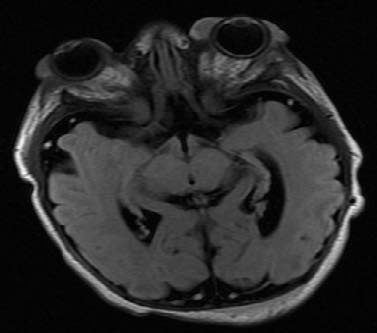
Figure 2: Magnetic resonance imaging of the orbit showing bilateral proptosis and shallow orbit.
Discussion
Pfeiffer syndrome is an autosomal dominant craniosynostosis syndrome with characteristic anomalies of the face and extremities. Other anomalies and visceral malformations may occasionally be associated with the syndrome. We have described associations of hypothyroidism and tail-like appendage, which were not reported earlier. The syndrome has three clinical subtypes with varying clinical features and prognostic implications.1 Type 1, the classic syndrome consists of craniosynostosis, brachycephaly, midface deficiency, broad thumbs, broad great toes, brachydactyly, and variable syndactyly. Type 2 consists of cloverleaf skull with Pfeiffer hands and feet, together with ankylosis of the elbows and severe proptosis. Type 3 is similar to type 2 with severe ocular proptosis but without cloverleaf skull and accounts for 14%.1-4 Considerable clinical overlap may occur between the three subtypes. Type 1 is compatible with life while early demise is characteristic of types 2 and 3. Mutations in fibroblast growth factor receptor (FGFR) genes cause Pfeiffer (OMIM 101600) syndrome and mutations in FGFR2 gene causes type 3.1-4 The present case had extreme ocular proptosis and typical hand and feet anomalies without cloverleaf skull and hence considered as type 3 variety. FGFR mutations could not be obtained in this case.
The ocular manifestations in Pfeiffer syndrome include hypertelorism, downslanting palpebral fissures, strabismus, and anterior chamber dysgenesis including Peter’s anomaly, corneal scleralisation, atypical iris, colobomata, retinal detachment and atrophic optic nerve heads.1-3 Cloverleaf skull, hypertelorism and extreme ocular proptosis may mimic conditions like thanatophoric dysplasia1,5 and other craniosynostosis syndromes.1 Severe proptosis may lead to corneal ulcer, endophthalmitis and globe rupture. Corrective surgery aim at decompression of the brain and remodeling of the skull, elongation and expansion of the bony orbits to accommodate the globes and enable eyelid closure, and opening of the nasopharyngeal airways by advancement of the naso-maxillary-zygomatic complex.1-4
Congenital upper airway anomalies related to midface hypoplasia may cause chronic hypoventilation and hypoxia leading to neurodevelopment deficits and mortality in severe Pfeiffer Syndrome.1-4 The present case had right sided choanal stenosis and anteriorly placed vocal cords.
Additional anomalies in Pfeiffer syndrome may include low-set ears, external auditory canal stenosis or atresia, aqueductal stenosis, hydrocephalus, cerebellar and brain stem herniation, hydronephrosis, pelvic kidney, hypoplastic gallbladder and visceral malformations particularly in type 3.1
True human tail arises from the most distal remnant of the embryonic tail and contains adipose tissue, connective tissue, central bundles of striated muscle, blood vessels and nerves, and is covered by skin.6 Human tail usually occurs in the lumbosacral region, can move and contract. Pseudo-tails are anomalous prolongation of the coccygeal vertebrae and resemble true tails. In the present case, the dermal appendage in the sacral region resembled human tail but there was no movement.
We observed an association of hypothyroidism with Pfeiffer syndrome. Congenital hypothyroidism in association with several congenital malformations have been described earlier.7 In addition, defects in a gene that maps to human chromosome 8 associated with both Pfeiffer syndrome and congenital hypothyroidism has been recognised.8 Hence, it is important to consider thyroid function tests in Pfeiffer syndrome patients.
Conclusion
Pfeiffer syndrome continues to have new associations since the first report. It is worth to consider thyroid function tests in Pfeiffer syndrome patients.
Acknowledgements
The authors reported no conflict of interest and no funding was received on this work.
References
1. Vogels A, Fryns JP. Pfeiffer syndrome. Orphanet J Rare Dis 2006;1:19. .
2. Koga H, Suga N, Nakamoto T, Tanaka K, Takahashi N. Clinical expression in Pfeiffer syndrome type 2 and 3: surveillance in Japan. Am J Med Genet A 2012 Oct;158A(10):2506-2510.
3. Greig AV, Wagner J, Warren SM, Grayson B, McCarthy JG. Pfeiffer syndrome: analysis of a clinical series and development of a classification system. J Craniofac Surg 2013 Jan;24(1):204-215. .
4. Fearon JA, Rhodes J. Pfeiffer syndrome: a treatment evaluation. Plast Reconstr Surg 2009 May;123(5):1560-1569. .
5. Naveen NS, Murlimanju BV, Kumar V, Pulakunta T, Jeeyar H; Jeeyar H. Thanatophoric dysplasia: a rare entity. Oman Med J 2011 May;26(3):196-197. .
6. Mukhopadhyay B, Shukla RM, Mukhopadhyay M, Mandal KC, Haldar P, Benare A. Spectrum of human tails: A report of six cases. J Indian Assoc Pediatr Surg 2012 Jan;17(1):23-25. .
7. Razavi Z, Yavarikia A, Torabian S. Congenital anomalies in infant with congenital hypothyroidism. Oman Med J 2012 Sep;27(5):364-367. .
8. PFEIFFER SYNDROME #101600. Online Mendelian Inheritance in Man (OMIM), available at http://omim.org/entry/101600.
|