|
Abstract
Intraoral schwannoma is a rare entity. Tongue has been reported as the most common oral site. Those involving salivary glands are unusual and parotid gland is the usual site. Literature search revealed only one case of schwannoma involving the sublingual gland. Hence, this is a presentation of another case of sublingual gland schwannoma with a review of literature, in a young female of 21 years old.
Keywords: Schwannoma; Mouth; Sublingual gland; Case report.
Introduction
Originally described by Verocay in 1910, schwannomas are benign, slow growing, mostly solitary and encapsulated tumors. It may arise from peripheral or autonomic nerves. Schwannomas in the head and neck region occur in 25% to 45% of cases, the majority being nonvestibular and extracranial.1-4 Intraoral schwannomas are rare wherein the tongue is the most common site followed by the palate and floor of the mouth.2,3
Schwannomas involving the salivary gland is relatively an uncommon form of extracranial neurogenic tumor and commonly occur in the parotid gland. Typical presentation of schwannomas involving the sublingual salivary gland is extremely rare. To date, only one case has been reported in English literature.5 This is a report of another case of intraoral schwannoma with a review of literature in a 21-year-old young female.
Case Report
A 21-year-old female presented to the hospital with complaints of slowly progressive irreducible painless swelling in the right floor of mouth for the past 2 years. The swelling was small initially but increasing in size gradually since 18 months. There was no increase of swelling during eating and it did not affect her speech, swallowing, or breathing. Oral examination revealed nontender, approximately 2 × 2 cm firm mass in the right floor of mouth which was not fixed to the surrounding tissues. The mucosa overlaying the mass was normal with no obvious opening or discharge coming out of it. Mobility of the tongue was normal and there was no evidence of neurological deficit in lingual or hypoglossal nerve. Neck examination was within normal limits.
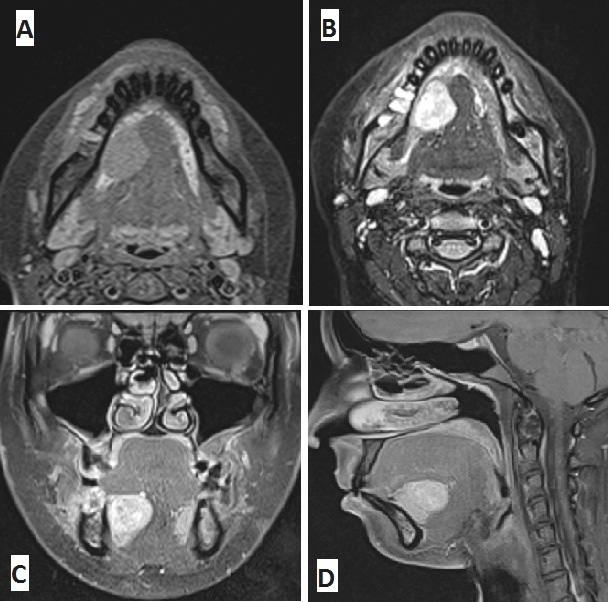
Figure 1: (A) Axial T1 weighted, (B) axial T2 weighted, (C) coronal contrast enhanced T1 and (D) sagittal T2 weighted MR images of the mass right sublingual area. The mass is well defined homogeneous hypointense on T1 weighted images, and heterogeneous hyperintense on coronal contrast enhanced T1 and sagittal T2 weighted images.
Subsequently, a CT scan was performed which revealed homogenous low density soft tissue lesion with ill-defined margins in the right floor of mouth anterior to the right submandibular gland. A further MRI scan showed well-demarcated mass showing hypointense homogeneous signals to the surrounding tissues on T1-weighted images and well-defined hyperintense heterogeneous signal intensity in T2-weighted and enhanced T1-weighted images with a measurement of 25 mm × 25 mm in size (Fig. 1). Based on clinical and radiological assessment, a presumptive diagnosis of soft tissue benign looking neoplasm in the floor of mouth probably involving the sublingual gland or a minor salivary gland tumor was made.
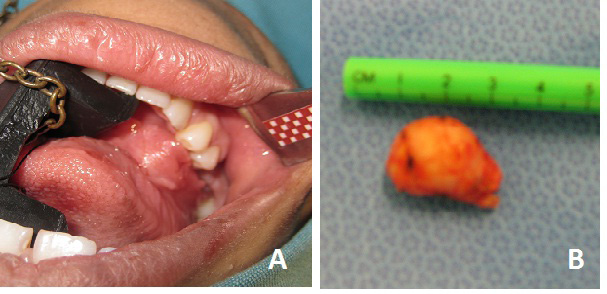
Figure 2: (A) Mucosa covered swelling in right floor of mouth and (B) the gross surgical specimen.
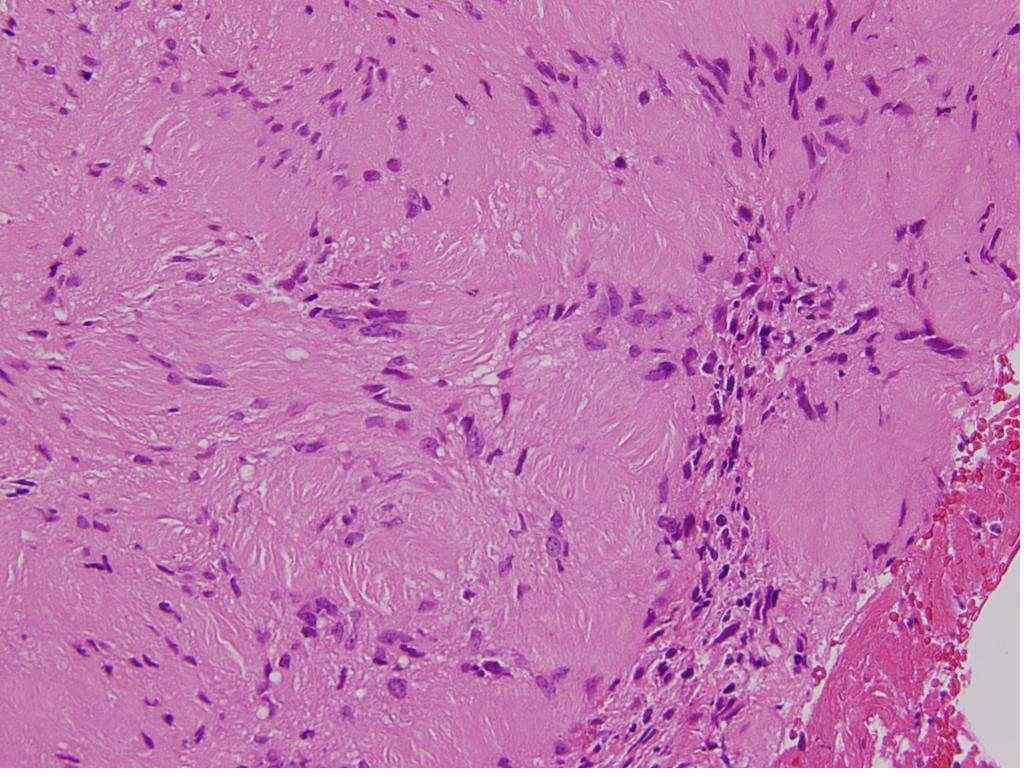
Figure 3: Hematoxylin and eosin staining of the specimen showing proliferated spindle shaped tumor cells with palisading. (× 40)

Figure 4: Immunohistochemical staining of the tumor cells showing strong immunpositivity for S-100 protein. (× 20).
Fine needle aspiration cytology was inconclusive and hence an incisional frozen section biopsy was performed on the operating table under local anesthesia which yielded a diagnosis of schwannoma. The patient then underwent complete excision of the tumor by intraoral approach (Fig. 2). There was no involvement of the lingual nerve or hypoglossal nerve observed during the procedure. Final histopathological examination confirmed the tumor to be schwannoma arising from the right sublingual gland due to the presence of nests of gland remnants and ducts in the vicinity of the tumor without a capsule. Microscopically, the lesion was a benign spindle cell lesion showing fascicular arrangement and orderly nuclear palisading around eosinophilic stromal material with Verocay bodies. There was no nuclear pleomorphism, degenerative changes, atypia or necrosis. Typically, the cells were positive for S100 and negative for CD34, NFP and EMA (Figs. 3 and 4). Regular follow-up did not reveal any recurrence to date.
Discussion
Schwannomas pose some challenge in the diagnosis because of their nonspecific history and clinical examination.4 They usually present as longstanding, firm, well-defined painless mass having a predilection for the peripheral portion of cranial nerves but with no neurological defects in the majority of cases.6 It can affect any age but mostly occur in patients between the age of 20 and 50 years.7 Exact causation of schwannoma is unknown and is believed to originate from the proliferation of Schwann cells in the perineurium.8 Around 25% to 45% of extra cranial schwannomas occur in the head and neck region with the usual presenting symptom as being an enlarging neck mass. Pain and neurological deficits are ominous signs and may indicate malignant change.9 Intraoral schwannomas are rare. Pattani et al. reported only 31 cases in their literature review. The tongue is the most common site of occurrence in the mouth.10-12 Those affecting the floor of mouth are extremely rare and have been reported to involve the hypoglossal nerve, mylohyoid and lingual. Additionally, those involving the facial nerve, mandibular bone, soft palate and maxillary sinus have also been reported.4,7,8,13-15
There is a paucity of literature about the neurogenic mesenchymal tumors involving the salivary glands. Seventy percent of salivary gland tumors occur in the parotid gland and predominantly epithelial in origin. Oral ranulas which are extravasation psudocysts of the sublingual glands are common,16 but the tumors arising from the sublingual gland account only for 0.3% to 1% of all epithelial tumors and the majority are malignant neoplasm.5 Okada et al. reported the first case of schwannoma arising from the sublingual gland in a 70-year-old woman. Mohiuddin et al.6 and Naik et al.17 have reported sublingual schwannoma in the literature but neither commented the site of origin as the sublingual gland nor identified the nerve of possible involvement. Hence, the authors presume that this case is the second addition to the literature occurring in a young female of 21 years old.5
Various mesenchymal tumors of sublingual space arising from nonepithelial components have rarely been reported in the literature. Gunhan et al. and Ogawa et al.18,19 reported solitary fibrous tumors arising from the sublingual gland in which remnant of the ducts within the tumor have been demonstrated, and both were mesothelioma. Okada et al.5 presented the schwannoma in the sublingual gland with embedded sublingual gland remnant. The evidence of gland remnant or duct without a capsule within the tumor is highly confirmatory that the tumor is arising from the gland itself.5 In the presented case too, there were gland remnants with no demonstrable capsule. Nerve infiltration was not evident. Wakoh et al.20 has reported that most schwannomas in the oral region have their origin in the hypoglossal or vagal nerve. However, in this case, no nerve involvement was encountered during surgery, and hence, it is believed that it wa not related to these nerves in the floor of mouth.
Because of its rarity and broad range of morphological appearances, schwannomas of the sublingual salivary gland can be confused with a variety of benign and malignant neoplasms. The extent to which a given histopathological feature is present can help determine the most appropriate diagnosis. The characteristic histological pattern is one of alternating Antoni type A and type B areas. Antoni type A consists of compact spindle shaped cells with indistinct cytoplasmic borders and occasional clear intranuclear vacuoles. The cells may exhibit nuclear palisading and Verocay bodies. Antoni B consists of distinct loose microscopic tissues with less cellularity.15 Immunohistochemical staining with anti-S-100 protein antibody demonstrates an intensely positive staining of Schwann cells which is the most valuable finding in diagnosis. Leu-7 antigen, vimentin and glial fibrillary acidic protein also provide useful immunostaining.15 In the presented case, the tumor showed spindle cell pattern with fascicular arrangement showing nuclear palisading and Verocay bodies indicating Antoni type A pattern. Typically, these cells were positive for S100 and negative for CD34, NFP and EMA.
The role of preoperative diagnostic imaging like CT/MRI scans has not been properly established in the literature.6 Kawakami et al.7 reported no diagnostic findings for sublingual schwannoma by imaging. Kun et al. were able to reach a correct diagnosis in only 4 cases of the 49 cases studied and concluded that diagnosis based on imaging is extremely difficult.21 However, the imaging is of paramount importance in preoperative planning and to rule out the possibility of malignancy such as local infiltration. The mainstay of treatment is complete surgical excision and failure to get adequate wide excision is generally associated with an unacceptably high local recurrence rate. Lymphatic metastases are rare and, hence, routine lymphadenectomy is not recommended.21
Conclusion
Salivary gland schwannomas represent a lesion not often encountered in clinical practice. The rarity of sublingual gland schwannomas makes it usually indistinguishable from other benign neoplasms. The final diagnosis should be made after histopathological and immunohistochemical analysis. Complete surgical excision is recommended. Recurrences and malignant transformations are rare.
Acknowledgements
The authors reported no conflict of interest and no funding was received for this work.
References
1. Verocay J. Zur Kenntnis der. "Neurofibrome. Beitr Pathol Anat Pathol 1910;48:1-69.
2. Colreavy MP, Lacy PD, Hughes J, Bouchier-Hayes D, Brennan P, O’Dwyer AJ, et al. Head and neck schwannomas–a 10 year review. J Laryngol Otol 2000 Feb;114(2):119-124.
3. Hatziotia JC, Asprides H. Neurilemoma (schwannoma) or the oral cavity. Oral Surg Oral Med Oral Pathol 1967 Oct;24(4):510-526.
4. Kang GC, Soo KC, Lim DT. Extracranial non-vestibular head and neck schwannomas: a ten-year experience. Ann Acad Med Singapore 2007 Apr;36(4):233-238.
5. Okada H, Tanaka S, Tajima H, et al. Schwannoma arising from the sublingual gland Annals of Diganostic Pathology 2012;16:141-44.
6. Mohiuddin SA, Badal S. Sublingual swelling- schwannoma: A rare case report Indian. J Oral Sci 2012;3(1):42-44.
7. Kawakami R, Kaneko T, Kadoya M, et al. Schwannoma in the sublingual space Dentomaxillofac Radio 2004;333:259-26.
8. Parikh N, Desai N. Intraoral schwannoma (neurilemmoma): An unusual anterior palatal swelling- A Case report J Int. Oral Health 2010;2(4):87-91.
9. Colreavy MP, Lacy PD, Hughes J, Bouchier-Hayes D, Brennan P, O’Dwyer AJ, et al. Head and neck schwannomas–a 10 year review. J Laryngol Otol 2000 Feb;114(2):119-124.
10. Gallo WJ, Moss M, Shapiro DN, Gaul JV. Neurilemoma: review of the literature and report of five cases. J Oral Surg 1977 Mar;35(3):235-236.
11. Das Gupta TK, Brasfield RD, Strong EW, Hajdu SI. Benign solitary Schwannomas (neurilemomas). Cancer 1969 Aug;24(2):355-366.
12. Wright BA, Jackson D. Neural tumors of the oral cavity. A review of the spectrum of benign and malignant oral tumors of the oral cavity and jaws. Oral Surg Oral Med Oral Pathol 1980 Jun;49(6):509-522.
13. Martins MD, Taghloubi SA, Bussadori SK, Fernandes KP, Palo RM, Martins MA. Intraosseous schwannoma mimicking a periapical lesion on the adjacent tooth: case report. Int Endod J 2007 Jan;40(1):72-78.
14. Drevelengas A, Kalaitzoglou I, Lazaridis N. Sublingual hypoglossal neurilemmoma. Case report. Aust Dent J 1998 Oct;43(5):311-314.
15. Pattani KM, Dowden K, Cherie-Ann O, et al. unique case of a sublingual- space shwannoma arising from the mylohyoid nerve ENT Journal 2010;89(7):31-3.
16. Bahnassy M. A huge oral ranula. Oman Med J 2009 Oct;24(4):306-307.
17. Naik SM, Goutham MK, Ravishankara S, et al. Sublingual schwannoma: A rare clinical entity reported in a hypothyroid female. International Journal of Head and Neck Surgery 2012;3(1):33-39.
18. Günhan O, Yildiz FR, Celasun B, Onder T, Finci R. Solitary fibrous tumour arising from sublingual gland: report of a case. J Laryngol Otol 1994 Nov;108(11):998-1000.
19. Ogawa I, Sato S, Kudo Y, Miyauchi M, Sugiyama M, Suei Y, et al. Solitary fibrous tumor with malignant potential arising in sublingual gland. Pathol Int 2003 Jan;53(1):40-45.
20. Wakoh M, Yonezu H, Otonari T, Sano T, Matsuzaka K, Inoue T, et al. Two cases of schwannoma with marked cystic changes. Dentomaxillofac Radiol 2005 Jan;34(1):44-50.
21. Kun Z, Qi DY, Zhang KH. A comparison between the clinical behavior of neurilemmomas in the neck and oral and maxillofacial region. J Oral Maxillofac Surg 1993 Jul;51(7):769-771.
|