Diabetes mellitus (DM) is a metabolic disease characterized by reduced insulin activity and/or insulin production. As the disease progresses, pathological alterations such as nephropathy, retinopathy, and cardiovascular problems begin to manifest.1 Diabetic retinopathy (DR) is a leading cause of visual impairment in working-age individuals.2,3 In 2019, the International Diabetes Federation estimated the global population with DM to be 463 million, projected to reach 700 million by 2045.4 A 2021 review estimated the global prevalence of diabetes at 22.7%.5 The major risk factors for DR are older age, high body mass index, duration of diabetes, high glycated hemoglobin levels, and high blood pressure.6–9
DR develops due to chronic hyperglycemia causing injury to retinal blood vessels resulting in breaches to the blood-retinal barrier leading to abnormal neovascularization, altering the retinal structure.10 Retinal microaneurysms are the first clinical sign of DR and are found in mild levels of the disease. In moderate DR, exudates, hemorrhages, and minimal intraretinal microvascular abnormalities develop, and become prominent in severe stages. The main clinical changes in proliferative DR neovascularization include macular edema.11
DM, the precursor of DR, is a public health concern in the Arab world as well. In the Gulf Cooperation Council (GCC) countries, type 2 DM is present in 8–22% of working-age people against 9.0% globally.12,13 The overall DM prevalence has been estimated at 32.8% in Saudi Arabia14 and 16.3% in the UAE.15
The global prevalence of DR among diabetic patients is estimated at 27.0% and is responsible for 0.4 million cases of blindness.16 The GCC countries have a similar prevalence of DR. A systematic review in Saudi Arabia showed a prevalence of 6.3–88.1%.17 Two other Saudi Arabian studies reported 69.8% and 19.7% prevalence.17,18 Studies from the UAE19 and Kuwait20 found DR prevalence of 19.0%, and 30.7%, respectively.
However, comparative estimates of prevalence are problematic because individual DR studies may have different patient characteristics and follow different methodologies. Studies with standardized definitions and methods are essential for generating accurate epidemiological data.21–22 The demographics of the GCC countries are unlike most others in the world. Non-nationals account for 47% of the total GCC population, and nationals are in the minority except in Oman and Saudi Arabia.11 To our knowledge, no publicly documented study has evaluated the prevalence of DR in the GCC. Therefore, we conducted a rigorous systematic review and meta-analysis to frame and answer the research questions. This study analyzes the research published between 2003 and 2019 that estimated the prevalence of DR in the GCC member nations of Saudi Arabia, the UAE, Oman, Kuwait, Qatar, and Bahrain.
Methods
This review followed the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) 2020 guidelines and checklists as shown in Figure 1.23 We conducted an organized search and review of studies in English language, published between 2003 and 2019, and available online in peer-reviewed journals, that addressed the prevalence or frequency of DR among diabetes patients in GCC countries. The dataset was collected from the Web of Sciences, Scopus, PubMed, Google Scholar, ProQuest, and Medline. A comprehensive search of the titles and abstracts was performed using the Boolean search string ῾diabetic retinopathy’ AND (prevalence OR epidemiology OR distribution OR rate OR incidence OR frequency OR proportion) AND (῾Saudi Arabia’ OR ῾United Arab Emirates’ OR Oman OR Qatar OR Kuwait OR Bahrain OR GCC).
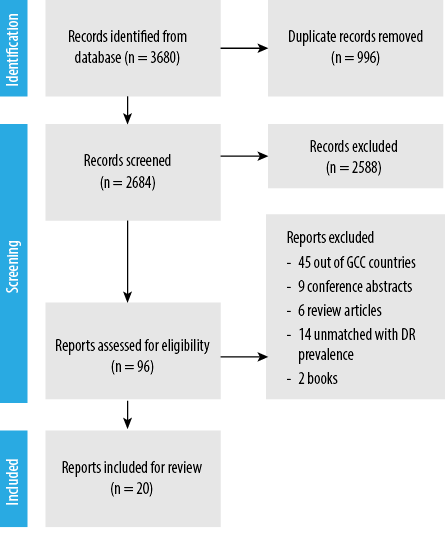 PRISMA: Preferred Reporting Items for Systematic reviews and Meta-Analyses; DR: Diabetic retinopathy; GCC: Gulf Cooperation Countries.
PRISMA: Preferred Reporting Items for Systematic reviews and Meta-Analyses; DR: Diabetic retinopathy; GCC: Gulf Cooperation Countries.
Figure 1: PRISMA 2020 flow diagram model for systematic reviews used in the prevalence of DR in the GCC countries.
All population-based and cross-sectional studies on the prevalence of DR in males and females among diabetic patients in the GCC countries were considered. To be included in the review, a paper was required to have an observational research design with a thorough description of data collection approaches, such as sampling. Articles using secondary data were excluded; for example, a 2020 study in Oman.24
The collected information — first author’s name, year of publication, country, sample size, prevalence (%), frequency of retinopathy, participants’ sex, mean age, mean duration of diabetes, and the type of DR (proliferative or non-proliferative)— was tabulated in a Microsoft Excel sheet.
MedCalc-Version 19.6.1 software (MedCalc, Mariakerke, Belgium) was used for meta-analyzing the prevalence of DR. The heterogeneity among the selected studies was measured by a Q-statistic that was assigned as chi-square under the given homogeneity of effect sizes. The I2 index I2 scale ranges from no heterogeneity (0%) to high heterogeneity (75%). The overall pooled prevalence of DR was measured using a random-effects model and its associated 95% CI. A p-value ≤ 0.05 was considered statistically significant.
Results
Study details
Our search initially returned 3680 articles. After removing duplicates, we reviewed the titles of 2684 studies, of which 2588 were excluded after reading their abstracts because they did not meet the inclusion criteria of the study. Then, 76 studies were excluded due to the inability to extract the required information. Finally, 20 articles that met the selection criteria were chosen for the study.
Description of the included articles
Table 1 shows the fundamental features of the articles included in our meta-analysis. The dataset comprised 20 cross-sectional and population-based studies from the GCC countries, published between 2003 and 2019 which provided information on the prevalence of retinopathy in patients with diabetes. The sample sizes of these studies ranged widely between 92 and 50 464, with a total of 61 855 patients. Ten (50.0%) studies investigated the prevalence of DR in individuals with type 2 diabetes, while the other nine studied patients with both type 1 and type 2 diabetes. The mean duration of diabetes ranged between 8.61 ± 5.96 and 13.40 ± 8.24 years.
Table 1: Basic characteristics of the articles in DR review.
|
Al-Otaibi et al,17 2017
|
Saudi Arabia
|
400
|
1 & 2
|
279
|
69.8
|
NA
|
NA
|
NA
|
NA
|
NA
|
|
|
Al-Rubeaan et al,18 2014
|
Saudi Arabia
|
50 464
|
2
|
9936
|
19.7
|
9.1
|
10.6
|
59.7
|
12.8
|
13.4 ± 8.2
|
|
|
Al-Maskari et al,19 2007
|
UAE
|
513
|
1 & 2
|
97
|
19.0
|
15.2
|
3.8
|
53.3
|
NA
|
≥ 10
|
|
|
Al Sarraf et al,20 2010
|
Kuwait
|
704
|
1 & 2
|
216
|
30.7
|
NA
|
NA
|
NA
|
NA
|
NA
|
< 0.001
|
|
Khan et al,25 2010
|
Saudi Arabia
|
473
|
1 & 2
|
142
|
30.0
|
27.7
|
2.3
|
NA
|
NA
|
8.6 ± 6.0
|
|
|
Al Ghamdi et al,26 2012
|
Saudi Arabia
|
612
|
NA
|
206
|
33.7
|
31.0
|
3.5
|
63.3
|
NA
|
NA
|
|
|
El-Bab et al,27 2012
|
Saudi Arabia
|
690
|
1 & 2
|
249
|
36.1
|
29.7
|
6.4
|
46.1
|
11.9
|
11.9 ± 7.9
|
|
|
Ahmed et al,28 2016
|
Saudi Arabia
|
401
|
2
|
146
|
36.4
|
32.2
|
4.2
|
54.6
|
12.3
|
13.4 ± 7.9
|
|
|
Yasir et al,29 2019
|
Saudi Arabia
|
395
|
1 & 2
|
133
|
33.7
|
39.7
|
5.0
|
NA
|
NA
|
NA
|
|
|
Khandekar et al,30 2003
|
Oman
|
2249
|
1 & 2
|
365
|
16.2
|
NA
|
NA
|
NA
|
NA
|
NA
|
< 0.001
|
|
Elshafei et al,31 2011
|
Qatar
|
483
|
1 & 2
|
153
|
31.7
|
NA
|
NA
|
< 40.0
|
NA
|
12.9 ± 9.1
|
|
|
Al-Adsani,32 2007
|
Kuwait
|
165
|
2
|
66
|
40.0
|
37.0
|
3.0
|
NA
|
NA
|
NA
|
|
|
Al Alawi et al,33 2012
|
Bahrain
|
736
|
1 & 2
|
190
|
25.8
|
24.8
|
1.0
|
24.0–8.0
|
NA
|
NA
|
|
|
Al-Zuabi et al,34 2005
|
Kuwait
|
92
|
2
|
7
|
7.6
|
NA
|
NA
|
NA
|
NA
|
NA
|
|
|
Ageely,35 2019
|
Saudi Arabia
|
281
|
2
|
91
|
32.4
|
NA
|
NA
|
NA
|
NA
|
NA
|
|
|
Khan et al,36 2014
|
Saudi Arabia
|
506
|
2
|
90
|
17.8
|
18.3
|
1.4
|
57.4
|
NA
|
10.2 ± 6.0
|
|
|
Szabo et al37 2015
|
UAE
|
150
|
2
|
9
|
6.0
|
NA
|
NA
|
58.0
|
NA
|
14.2
|
|
|
Jelinek et al,38 2017
|
UAE
|
490
|
2
|
65
|
13.3
|
NA
|
NA
|
60.6
|
11.3
|
NA
|
|
|
Alfadda et al,39 2006
|
Saudi Arabia
|
99
|
2
|
25
|
25.3
|
NA
|
NA
|
57.0
|
NA
|
11.8
|
|
DR: diabetic retinopathy; DM: diabetes mellitus PDR: proliferative diabetic retinopathy; NPDR: non-proliferative diabetic retinopathy; NA: not available.
Prevalence of DR among DM patients
The results of the meta-analysis to evaluate the prevalence of DR among diabetic patients in the GCC countries are presented in Table 2. The pooled prevalence of DR was found to be 20.5% (CI: 20.212–20.850; p < 0.001). The majority (n = 13; 65.0%) reviewed studies reported a significantly higher prevalence of DR compared to global prevalence, while seven (35.0%) studies reported lower-than-global prevalence.
Table 2: Meta-analysis of studies on the prevalence of diabetic retinopathy (DR) among diabetic individuals in the Gulf Cooperation Council (GCC) countries.
|
Al-Otaibi et al,17 2017
|
Saudi Arabia
|
400
|
69.75 (64.989–74.216)
|
0.7
|
|
Al-Rubeaan et al,18 2014
|
Saudi Arabia
|
50 464
|
19.69 (19.343–20.039)
|
81.6
|
|
Al-Maskari et al,19 2007
|
UAE
|
513
|
18.90 (15.610–22.570)
|
0.8
|
|
Al-Sarraf et al,20 2010
|
Kuwait
|
704
|
30.68 (27.291–34.235)
|
1.1
|
|
Khan et al,25 2010
|
Saudi Arabia
|
473
|
30.02 (25.921–34.373)
|
0.8
|
|
Al Ghamdi et al,26 2012
|
Saudi Arabia
|
612
|
33.66 (29.921–37.558)
|
1.0
|
|
El-Bab et al,27 2012
|
Saudi Arabia
|
690
|
36.09 (32.497–39.796)
|
1.1
|
|
Ahmed et al,28 2016
|
Saudi Arabia
|
401
|
36.41 (31.690–41.330)
|
0.7
|
|
Yasir et al,29 2019
|
Saudi Arabia
|
395
|
33.67 (29.022–38.567)
|
0.6
|
|
Khandekar et al,30 2003
|
Oman
|
2249
|
16.23 (14.728–17.819)
|
3.6
|
|
Elshafei et al,31 2011
|
Qatar
|
483
|
31.68 (27.548–36.032)
|
0.8
|
|
Al-Adsani,3 2007
|
Kuwait
|
165
|
40.00 (32.464–47.902)
|
0.3
|
|
Al Alawi et al,33 2012
|
Bahrain
|
736
|
25.82 (22.688–29.138)
|
1.2
|
|
Al-Zuabi et al,3 2005
|
Kuwait
|
92
|
7.61 (3.114–15.050)
|
0.2
|
|
Ageely,35 2019
|
Saudi Arabia
|
281
|
32.38 (26.947–38.198)
|
0.5
|
|
Khan et al,36 2014
|
Saudi Arabia
|
506
|
17.79 (14.552–21.403)
|
0.8
|
|
Szabo et al,37 2015
|
UAE
|
150
|
6.00 (2.780–11.084)
|
0.2
|
|
Jelinek et al,38 2017
|
UAE
|
490
|
13.27 (10.389–16.593)
|
0.8
|
|
Alfadda et al,39 2006
|
Saudi Arabia
|
99
|
25.25 (17.056–34.982)
|
0.2
|
|
Alwakeel et al,40 2008
|
Saudi Arabia
|
1952
|
16.70 (15.072–18.431)
|
3.2
|
|
Total
|
|
61 855
|
100.0
|
|
|
Mean prevalence of diabetic retinopathy in GCC
|
|
|
20.53 (20.212–20.850)
|
|
|
Heterogeneity between groups
|
|
|
p < 0.001
|
|
The study conducted by Al-Otaibi et al,17 among Saudi Arabian patients indicated the highest prevalence of DR (69.75%; CI: 64.989– 4.216) with diabetes type 1 and 2. The lowest prevalence of DR was reported by Szabo et al,37 from UAE (6.0%; CI: 2.780–11.084). Our meta-analysis revealed a high degree of heterogeneity between the reviewed studies (p < 0.001), with an I2 value of 98.0%.
DR classification in the GCC diabetic patients
Table 3 displays the classification of DR in the GCC countries, which was reported in 11 out of 20 studies. Both the lowest (9.1%) and the highest (39.7%) proportions of non-proliferative DR were reported by studies conducted in Saudi Arabia.19 Additionally, proliferative DR was most prevalent in Saudi Arabian diabetic patients (10.6%).18
Table 3: The types of diabetic retinopathy in the Gulf Cooperation Council countries (2003–2019).
|
Al-Maskari et al,19 2007
|
UAE
|
15.2
|
3.8
|
|
Al-Rubeaan et al,18 2014
|
Saudi Arabia
|
9.1
|
10.6
|
|
Khan et al,25 2010
|
Saudi Arabia
|
27.7
|
2.3
|
|
Al Ghamdi et al,26 2012
|
Saudi Arabia
|
31.0
|
3.5
|
|
El-Bab et al,27 2012
|
Saudi Arabia
|
29.7
|
6.4
|
|
Ahmed et al,28 2016
|
Saudi Arabia
|
32.2
|
4.2
|
|
Yasir et al,29 2019
|
Saudi Arabia
|
39.7
|
5.0
|
|
Al-Adsani 200732
|
Kuwait
|
37.0
|
3.0
|
|
Al Alawi et al,33 2012
|
Bahrain
|
24.8
|
1.0
|
|
Khan et al,36 2014
|
Saudi Arabia
|
18.3
|
1.4
|
NPDR: non-proliferative diabetic retinopathy; PDR: proliferative diabetic retinopathy.
Discussion
To the best of our knowledge, this is the first systematic review and meta-analysis on the prevalence of DR among people with type 1 and 2 diabetes in the GCC countries. Eleven of the 20 reviewed studies were from Saudi Arabia, three each from UAE and Kuwait, and one each from Oman, Qatar, and Bahrain. The review revealed an overall DR prevalence of 20.5% in the region.
The highest prevalence of DR was found among Saudi Arabian diabetic patients17 and the lowest among the patients in UAE.37 Most (82.8%) of our participants were from a single study by Al-Rubeaan et al,18 which might explain the similarity between the pooled prevalence of DR in our review and theirs. Moreover, different Saudi Arabian studies reported widely differing DR prevalence (69.8%,17 36.4%,28 and 17.8%),37 perhaps because of the large differences in sample sizes and other study specifics. Our finding of an overall DR prevalence of 20.5% in the GCC is lower than the global prevalence of 25.2% reported by the International Diabetes Federation15 and elsewhere.41,42 Conversely, our DR prevalence exceeds that of Southeast Asia (17.0%) and South and Central America (13.4%).15
The GCC populations are known to be at high risk for lifestyle diseases including DM.42 However, the prevalence of DR in the GCC countries is still lower compared to the global and regional estimates, which can be attributed to better screening measures and quality of care in this relatively affluent region. This study also observed that the duration of DM is an important DR risk factor, which was consistent with studies elsewhere.43,44 The GCC countries should place more emphasis on educating the youth regarding the importance of a healthy lifestyle. Diabetic and pre-diabetic individuals should be identified by pro-active screening and encouraged to make healthy lifestyle changes. The GCC primary care physicians should be made aware of the proliferation of unhealthy lifestyles among the residents, their consequent vulnerability to lifestyle diseases such as DM, and the growing prevalence of DR.45,46
The most important limitation of our study is that its source studies were highly heterogeneous in terms of sample sizes, inclusion criteria, definitions, overall study parameters, and methodology. This may have led to wide variations in their findings. Additionally, most selected studies were from a single country, Saudi Arabia, and most of the patients were from a single study. Therefore, we advise caution in generalizing our findings to the individual countries of the GCC.
Conclusion
This study presents the first comprehensive analysis of the prevalence of DR in the GCC countries. Our data, derived from 20 studies involving a total of 61 855 patients with diabetes, indicates an overall prevalence of 20.5% of DR in this region. Our findings emphasize the need for enhancement in targeted diabetes screening and management, eye examinations for retinopathy, controlling risk factors, and healthy lifestyle education. However, owing to the high interstudy heterogeneity, our review findings should be applied cautiously to individual GCC countries.
Disclosure
The authors declared no conflicts of interest. No funding was received for this study.
Acknowledgments
We wish to acknowledge the kind support we received from the University of Buraimi, Oman.
references
- 1. Padhi S, Nayak AK, Behera A. Type II diabetes mellitus: a review on recent drug based therapeutics. Biomed Pharmacother 2020 Nov;131:110708.
- 2. Li X, Tan TE, Wong TY, Sun X. Diabetic retinopathy in China: epidemiology, screening and treatment trends-A review. Clin Exp Ophthalmol 2023 Aug;51(6):607-626.
- 3. Chistiakov DA. Diabetic retinopathy: pathogenic mechanisms and current treatments. Diabetes Metab Syndr 2011;5(3):165-172.
- 4. Yau JW, Rogers SL, Kawasaki R, Lamoureux EL, Kowalski JW, Bek T, et al; Meta-Analysis for Eye Disease (META-EYE) Study Group. Global prevalence and major risk factors of diabetic retinopathy. Diabetes Care 2012 Mar;35(3):556-564.
- 5. Teo ZL, Tham YC, Yu M, Chee ML, Rim TH, Cheung N, et al. Global prevalence of diabetic retinopathy and projection of burden through 2045: systematic review and meta-analysis. Ophthalmology 2021 Nov;128(11):1580-1591.
- 6. Alharbi AM, Alhazmi AM. Prevalence, risk factors, and patient awareness of diabetic retinopathy in Saudi Arabia: a review of the literature. Cureus 2020 Dec;12(12):e11991.
- 7. McKay R, McCarty CA, Taylor HR. Diabetic retinopathy in Victoria, Australia: the visual impairment project. Br J Ophthalmol 2000 Aug;84(8):865-870.
- 8. Gallego PH, Craig ME, Hing S, Donaghue KC. Role of blood pressure in development of early retinopathy in adolescents with type 1 diabetes: prospective cohort study. BMJ 2008 Aug;337:a918.
- 9. Distefano LN, Garcia-Arumi J, Martinez-Castillo V, Boixadera A. Combination of anti-VEGF and laser photocoagulation for diabetic macular edema: a review. J Ophthalmol 2017;2017:2407037.
- 10. Claramunt J. Diabetic retinopathy. Rev Med Clin Las Condes 2009;20(5):670-679.
- 11. Aljulifi MZ. Prevalence and reasons of increased type 2 diabetes in Gulf Cooperation Council Countries. Saudi Med J 2021 May;42(5):481-490.
- 12. World Health Organization. Regional Office for the Eastern Mediterranean. The work of WHO in the Eastern Mediterranean Region: annual report of the Regional Director 2014. 2015 [cited October 2023]. Available from: https://iris.who.int/handle/10665/198942.
- 13. Meo SA. Prevalence and future prediction of type 2 diabetes mellitus in the Kingdom of Saudi Arabia: a systematic review of published studies. J Pak Med Assoc 2016 Jun;66(6):722-725.
- 14. International Diabetes Federation. IDF diabetes atlas. 9th ed. Brussels, Belgium: International Diabetes Federation; 2020. p. 7-44.
- 15. Thomas RL, Halim S, Gurudas S, Sivaprasad S, Owens DR. IDF diabetes atlas: a review of studies utilising retinal photography on the global prevalence of diabetes related retinopathy between 2015 and 2018. Diabetes Res Clin Pract 2019 Nov;157:107840.
- 16. Aljehani EA, Alhawiti AE, Mohamad RM. Prevalence and determinants of diabetic retinopathy among type 2 diabetic patients in Saudi Arabia: a systematic review. Cureus 2023 Jul;15(7):e42771.
- 17. Al-Otaibi H, Al-Otaibi MD, Khandekar R, Souru C, Al-Abdullah AA, Al-Dhibi H, et al. Validity, usefulness and cost of RETeval system for diabetic retinopathy screening. Transl Vis Sci Technol 2017 May;6(3):3.
- 18. Al-Rubeaan K, Youssef AM, Subhani SN, Ahmad NA, Al-Sharqawi AH, Al-Mutlaq HM, et al. Diabetic nephropathy and its risk factors in a society with a type 2 diabetes epidemic: a Saudi national diabetes registry-based study. PLoS One 2014 Feb;9(2):e88956.
- 19. Al-Maskari F, El-Sadig M. Prevalence of diabetic retinopathy in the United Arab Emirates: a cross-sectional survey. BMC Ophthalmol 2007 Jun;7:11.
- 20. Al Sarraf A, Al-Bannai S, Al-Furaih S, El-Shazly M. Prevalence and factors associated with diabetic retinopathy, a multi-centric study in Kuwait. Alex J Med 2010;46(2):99-108.
- 21. Ruta LM, Magliano DJ, Lemesurier R, Taylor HR, Zimmet PZ, Shaw JE. Prevalence of diabetic retinopathy in type 2 diabetes in developing and developed countries. Diabet Med 2013 Apr;30(4):387-398.
- 22. Salti HI, Nasrallah MP, Taleb NM, Merheb M, Haddad S, El-Annan J, et al. Prevalence and determinants of retinopathy in a cohort of Lebanese type II diabetic patients. Can J Ophthalmol 2009 Jun;44(3):308-313.
- 23. Page MJ, Moher D, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. PRISMA 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ 2021 Mar;372(160):n160.
- 24. Al-Rashdi FA, Al-Mawali A. Prevalence of diabetic retinopathy in Oman: a two decade national study. Oman Med J 2021 Mar;36(2):e238.
- 25. Khan AR, Wiseberg JA, Lateef ZA, Khan SA. Prevalence and determinants of diabetic retinopathy in Al Hasa region of Saudi Arabia: primary health care centre based cross-sectional survey, 2007-2009. Middle East Afr J Ophthalmol 2010 Jul;17(3):257-263.
- 26. Al Ghamdi AH, Rabiu M, Hajar S, Yorston D, Kuper H, Polack S. Rapid assessment of avoidable blindness and diabetic retinopathy in Taif, Saudi Arabia. Br J Ophthalmol 2012 Sep;96(9):1168-1172.
- 27. El-Bab MF, Shawky N, Al-Sisi A, Akhtar M. Retinopathy and risk factors in diabetic patients from Al-Madinah Al-Munawarah in the Kingdom of Saudi Arabia. Clin Ophthalmol 2012;6:269-276.
- 28. Ahmed RA, Khalil SN, Al-Qahtani MA. Diabetic retinopathy and the associated risk factors in diabetes type 2 patients in Abha, Saudi Arabia. J Family Community Med 2016;23(1):18-24.
- 29. Yasir ZH, Hassan AD, Rajiv K. Diabetic retinopathy (DR) among 40 years and older Saudi population with diabetes in Riyadh governorate, Saudi Arabia - a population based survey. Saudi J Ophthalmol 2019;33(4):363-368.
- 30. Khandekar R, Al Lawatii J, Mohammed AJ, Al Raisi A. Diabetic retinopathy in Oman: a hospital based study. Br J Ophthalmol 2003 Sep;87(9):1061-1064.
- 31. Elshafei M, Gamra H, Khandekar R, Al Hashimi M, Pai A, Ahmed MF. Prevalence and determinants of diabetic retinopathy among persons ≥ 40 years of age with diabetes in Qatar: a community-based survey. Eur J Ophthalmol 2011;21(1):39-47.
- 32. Al-Adsani AM. Risk factors for diabetic retinopathy in Kuwaiti type 2 diabetic patients. Saudi Med J 2007 Apr;28(4):579-583.
- 33. Al Alawi E, Ahmed AA. Screening for diabetic retinopathy: the first telemedicine approach in a primary care setting in Bahrain. Middle East Afr J Ophthalmol 2012;19(3):295-298.
- 34. Al-Zuabi H, Al-Tammar Y, Al-Moataz R, Al-Sabti K, Wani VB, Hamama F, et al. Retinopathy in newly diagnosed type 2 diabetes mellitus. Med Princ Pract 2005;14(5):293-296.
- 35. Ageely H. Long-term diabetes-related severe complications among individuals with T2DM in Jazan, Saudi Arabia. J Acute Dis 2019 Mar;8(2):72-77.
- 36. Khan AR, Al Abdul Lateef ZN, Fatima S, Al Yousuf SA, Khan Afghan SZ, Al Marghani S. Prevalence of chronic complication among type 2 diabetics attending primary health care centers of Al Ahsa district of Saudi Arabia: a cross sectional survey. Glob J Health Sci 2014 Apr;6(4):245-253.
- 37. Szabo SM, Osenenko KM, Qatami L, Korenblat Donato BM, Korol EE, Al Madani AA, et al. Quality of care for patients with type 2 diabetes mellitus in Dubai: a HEDIS-like assessment. Int J Endocrinol 2015;2015:413276.
- 38. Jelinek HF, Osman WM, Khandoker AH, Khalaf K, Lee S, Almahmeed W, et al. Clinical profiles, comorbidities and complications of type 2 diabetes mellitus in patients from United Arab Emirates. BMJ Open Diabetes Res Care 2017 Aug;5(1):e000427.
- 39. Alfadda A, Abdulrahman KA. Assessment of care for type 2 diabetic patients at the primary care clinics of a referral hospital. J Family Community Med 2006 Jan;13(1):13-18.
- 40. Alwakeel JS, Sulimani R, Al-Asaad H, Al-Harbi A, Tarif N, Al-Suwaida A, et al. Diabetes complications in 1952 type 2 diabetes mellitus patients managed in a single institution in Saudi Arabia. Ann Saudi Med 2008;28(4):260-266.
- 41. Heiran A, Azarchehry SP, Dehghankhalili S, Afarid M, Shaabani S, Mirahmadizadeh A. Prevalence of diabetic retinopathy in the Eastern Mediterranean Region: a systematic review and meta-analysis. J Int Med Res 2022 Oct;50(10):3000605221117134.
- 42. Atlas D. International diabetes federation. IDF diabetes atlas. 7th ed. Brussels, Belgium: International Diabetes Federation; 2015.
- 43. Hainsworth DP, Bebu I, Aiello LP, Sivitz W, Gubitosi-Klug R, Malone J, et al; Diabetes Control and Complications Trial (DCCT)/Epidemiology of Diabetes Interventions and Complications (EDIC) Research Group. Risk factors for retinopathy in type 1 diabetes: the DCCT/EDIC study. Diabetes Care 2019 May;42(5):875-882.
- 44. Song KH, Jeong JS, Kim MK, Kwon HS, Baek KH, Ko SH, et al. Discordance in risk factors for the progression of diabetic retinopathy and diabetic nephropathy in patients with type 2 diabetes mellitus. J Diabetes Investig 2019 May;10(3):745-752.
- 45. Al-Sinani S, Al-Mamari A, Woodhouse N, Al-Shafie O, Amar F, Al-Shafaee M, et al. Quality of diabetes care at outpatient clinic, Sultan Qaboos University Hospital. Oman Med J 2015 Jan;30(1):48-54.
- 46. Alawadi F, Abdelgadir E, Bashier A, Hassanein M, Rashid F, Alsaeed M, et al. Glycemic control in patients with diabetes across primary and tertiary government health sectors in the Emirate of Dubai, United Arab Emirates: a five-year pattern. Oman Med J 2019 Jan;34(1):20-25.