Laparoscopic cholecystectomy is consi-dered the gold standard treatment for cholelithiasis.1–3 Nevertheless, traumatic injury of the cystic artery and its arterial branches remains a severe problem that may lead to morbidities or even mortality.4 According to the literature, anatomical variations of the cystic artery are frequently reported as risk factors for hemorrhage during laparoscopic cholecystectomy.1 Anatomic irregularity of the artery to the cystic duct has been reported once, posing a serious risk of accidental injury and potential bleeding during laparoscopic cholecystectomy.2 This report aims to highlight an extremely rare duplication of the artery to the cystic duct and showcase its surgical significance.
Case report
An 18-year-old Caucasian female was referred to our institution with a two-month history of colicky abdominal pain in the right upper quadrant, which had progressively become worse. The patient’s clinical examination was unremarkable, without positive Murphy’s sign, tenderness, or jaundice. The patient’s body mass index was 27.3 kg/m2. Both patient’s vital signs and laboratory data, including bilirubin, alanine aminotransferase, and aspartate aminotransferase were within the normal spectrum. Abdominal ultrasound detected multiple gallstones in the gallbladder. A laparoscopic cholecystectomy was scheduled.
Surgeons carefully exposed the operating field to detect the Calot’s triangle during the operation. Then, the Calot’s triangle was meticulously dissected, and both the cystic artery and the cystic duct were revealed. When surgeons attained to detect the typical ‘H-configuration’ (which is formed by the cystic duct, the cystic artery, and the artery to the cystic duct), they incidentally identified an accessory branch of the artery supplying the cystic duct [Figure 1]. An inferior and superior arterial branch of the artery to the cystic duct was discovered, altering the typical ‘H-configuration’.To our knowledge, this is the first reported case of an artery to the cystic duct duplication. Duplication of the artery to the cystic duct constitutes a potential risk of accidental injury and significant hemorrhage during the operation.2

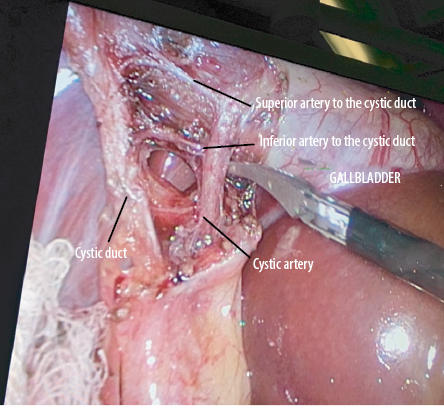 Figure 1: Duplication of the artery to the cystic duct. Presentation of both superior and inferior arterial branches in close relation to the cystic artery and the cystic duct. Alteration of the typical ‘H-configuration’.
Figure 1: Duplication of the artery to the cystic duct. Presentation of both superior and inferior arterial branches in close relation to the cystic artery and the cystic duct. Alteration of the typical ‘H-configuration’.
Both arterial branches were retracted and cauterized, so bleeding and subsequent postoperative complications could be avoided. The operation resumed in the usual fashion. Drainage was placed beneath the liver and removed on the second postoperative day. The patient was discharged on the third postoperative day with instructions. During the three-month follow-up, the patient demonstrated no complications.
Discussion
The artery to the cystic duct constitutes a sole, inferior arterial branch, emerging from the cystic artery and supplying the cystic duct, with a prevalence of 91.47%.2 The artery of the cystic duct typically originates at right angles from the cystic artery, then traverses between the junction of the cystic and the common hepatic duct and the junction of the cystic duct with the gallbladder to enter the cystic duct while forming an ‘H-configuration’.2
The artery to the cystic duct constitutes a significant risk factor for accidental injury and hemorrhage in the hepatobiliary triangle during laparoscopic cholecystectomy.2 When surgeons detect the ‘H-configuration’, the artery to the cystic duct must be carefully cauterized.2 Such a surgical step is of paramount clinical significance, especially when encountering a short cystic duct to preserve its length and avoid accidental bleeding or extrahepatic biliary radical injuries,1,2 as performed in the presented case.
It was previously reported that variant cystic arteries might not give the artery off to the cystic duct, unlike the typical cystic arteries.2 Such anatomic variations, including the branches of the artery to the cystic duct, may be detected preoperatively with the utilization of arteriography.2 However, arteriography is not included in the typical preoperative imaging of a patient with cholelithiasis. Hereby, surgeons’ thorough knowledge of all probable arterial variations, gentle maneuvers, and meticulous exposure of the Calot’s triangle are the cornerstones of a safe laparoscopic cholecystectomy.
Conclusion
Anatomical variations of the cystic artery are frequently documented, but variations of the artery to the cystic duct are extremely uncommon. Nevertheless, congenital variations of the artery to the cystic duct may not be as rare as considered. Their presence encumbers surgical maneuvers and increases intraoperative injury and hemorrhage potential.2 Herein, further research is recommended so that anatomical variations of the artery to the cystic duct are documented.
Disclosure
The authors declared no conflicts of interest. Written consent was obtained from the patient.
references
- 1. Ding YM, Wang B, Wang WX, Wang P, Yan JS. New classification of the anatomic variations of cystic artery during laparoscopic cholecystectomy. World J Gastroenterol 2007 Nov;13(42):5629-5634.
- 2. Rashid A, Mushtaque M, Bali RS, Nazir S, Khuroo S, Ishaq S. Artery to cystic duct: a consistent branch of cystic artery seen in laparoscopic cholecystectomy. Anat Res Int 2015;2015:847812.
- 3. Tebala GD, Innocenti P, Ciani R, Zumbo A, Fonsi GB, Bellini P, et al. Identification of gallbladder pedicle anatomy during laparoscopic cholecystectomy. Chir Ital 2004 May-Jun;56(3):389-396. Italian.
- 4. Thompson MH, Benger JR. Cholecystectomy, conversion and complications. HPB Surg 2000 Aug;11(6):373-378.