Urinary catheterization using feeding tubes (FTs) is a common procedure in neonatal intensive care units (NICU).1 Urinary catheterization is often required to relieve fluid retention, to collect urine, and occasionally for radiological studies.2 FTs sizes Fr 5, Fr 6, or Fr 8 are commonly used due to their availability and ease of use.3 Although the procedure is safe, complications have been reported, including trauma during insertion, hematuria, and tube knotting within the urinary bladder.3 Removal of a knotted tube from the bladder can be a major challenge. We report a case of spontaneous knotting of the FT within the bladder of a late preterm female infant.
Case Report
A 44-year-old woman (multigravida 9, multipara 6) delivered a late preterm female infant at 34 weeks of gestation by cesarean section under general anesthesia due to the baby being in a transverse lie. The mother had gestational diabetes. During her previous pregnancy, she had been positive for Group B Streptococcus infection.
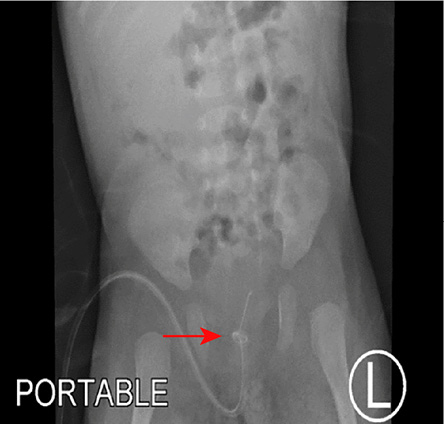
Figure 1: X-ray showing the knotted catheter (arrow) in the bladder of a late preterm
female infant.
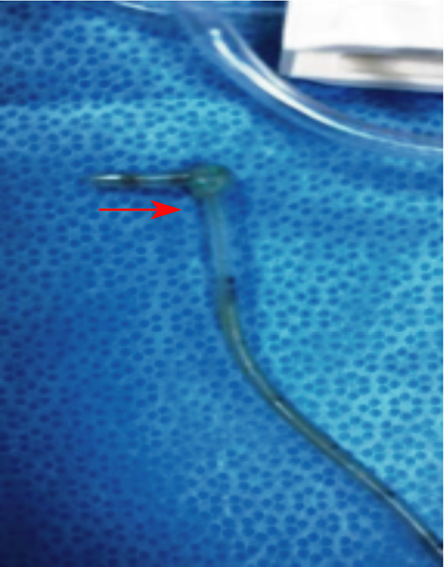
Figure 2: Post-operative photo showing the knotted catheter (arrow).
Antenatal steroids were administered four hours prior to delivery. The newborn’s Apgar scores were 7 and 9 at one and five minutes, respectively. Her birth weight was 1.68 kg (3–10th percentile), head circumference 31 cm (10–50th percentile), and length 45 cm (50th percentile). She also had asymmetrical intra-uterine growth restriction.
The baby developed respiratory distress and was admitted to the NICU where she was put on nasal continuous positive airway pressure and started on intravenous antibiotics ampicillin and gentamycin. The respiratory support was weaned off after seven days. However, nasogastric feeding continued for four weeks due to difficulty to establish oral feeding. Therefore, further investigations were performed, including head ultrasound, tandem mass spectrometry, serum ammonia, and urine for organic acid. The infant was catheterized with an Fr 6 infant FT to collect urine for organic acid analysis.
While removing the catheter 24 hours later, the nurse and the on-call physician noticed significant resistance. Examination showed that the catheter was deeply introduced into the bladder and was lodged at catheter level 11 cm. A supine x-ray of the abdomen showed a spontaneous true knot in the FT in the bladder [Figure 1]. Attempts by the pediatric surgical team to pull out the tube were unsuccessful.
The infant went for surgical intervention under general anesthesia. Following failed attempts of a guide-wire endoscopic retrieval, suprapubic cystotomy was successfully performed. The FT was found knotted in the urinary bladder. The knot was about 4 cm from the tip of the catheter [Figure 2]. After removing the tube, the urethra and the bladder mucosa were evaluated, and no further complications were detected. A Foley catheter was inserted into the bladder for urinary drainage for five days, during which the infant was administered antibiotics. She made a good post-operative recovery and was discharged after seven days.
Discussion
Although urinary bladder catheterization is a common and safe procedure in neonatal practice, it is not free of complications.1 FTs are commonly used in neonates due to the shortage of suitably sized Foley catheters. It has been reported that knotting of catheters is more frequent in male neonates, with an incidence of 0.2 per 100 000.3,4 Other complications include trauma during insertion and hematuria. Risk factors of pediatric catheter knotting are related to the length of insertion, physical properties of the tubing, catheterization technique, and the patient’s anatomical characteristics.5
Great care and expertise are required for inserting neonatal catheters. Among the reported strategies to minimize complications are using short catheters of standard lengths and adopting intermittent catheterization.6 When inserting a Foley catheter, its balloon should be fully inside the bladder before inflating to avoid urethral trauma. At birth, the length of the male urethra is about 5 cm and that of the female is about 2.2 cm.7 The insertion length of catheter should not exceed 5–6 cm in term newborns of either sex or 2.5–5 cm in premature babies.6 In the present case, excessive insertion length of the catheter (11 cm) was the main reason for knotting of the tube. The most common reported reasons for knotting are inserting the catheter > 10 cm and incorrectly inserting and securing the tube.8,9 Other risk factors include over-distended urinary bladder, bladder spasm, and using small sized catheters (Fr 10),4,10 and failing to externally secure the tube to prevent further progression into the bladder.3,4,10
Conservative management strategies should be attempted before surgical intervention, such as untangling the knot using an endoscopic retrieval guidewire, or applying constant traction under anesthesia.9,11,12 The constant traction method carries the risk of urethral injury and is unsuitable for bulky knots and true knots. The current case featured a true knot.
The endoscopic retrieval guidewire manipulation technique is sometimes effective if the knot is loose. We attempted this but unsuccessfully. Therefore, suprapubic cystotomy was performed to remove the knotted catheter from the bladder. This surgical procedure has been reported to be practical and cost effective in such cases.4,8 The reported risks include post-operative complications, such as bladder dysfunction and urethral stricture, as well as the need for long-term follow-up.13
Conclusion
Insertion of a FT for urinary catheterization in neonates requires caution, precision, and training. It is essential to select the catheter insertion length according to the age and sex of the infant. Complications, though rare, could be hazardous, which should always be kept in mind. Where suprapubic cystotomy is performed to take out the knotted catheter, long-term monitoring for postoperative complications may be required.
Disclosure
The authors declared no conflicts of interest. No funding was received for this study. Consent has been obtained from the parents of the neonate to publish this case report.
references
- 1. Sugar EC, Firlit CF. Knot in urethral catheter due to improper catheterization technique. Urology 1983 Dec;22(6):673-674.
- 2. Tang PM, Chung KL, Leung YC, Hung JW, Liu CC, Chao NS, et al. Intra-vesical knot of bladder catheter in an extremely low birthweight neonate: A case report. J Pediatr Surg Case Rep 2015;3(7):295-297.
- 3. Arena B, McGillivray D, Dougherty G. Urethral catheter knotting: Be aware and minimize the risk. CJEM 2002 Mar;4(2):108-110.
- 4. Raveenthiran V. Spontaneous knotting of urinary catheters: clinical and experimental observations. Urol Int 2006;77(4):317-321.
- 5. Singh VP, Sinha S. Spontaneous knotting of urinary catheters placed with nonindwelling intent: Case series and literature review. Urol Ann 2019 Oct-Dec;11(4):443-446.
- 6. Carlson D, Mowery BD. Standards to prevent complications of urinary catheterization in children: should and should-knots. J Soc Pediatr Nurs 1997 Jan-Mar;2(1):37-41.
- 7. Smith AB, Adams LL. Insertion of indwelling urethral catheters in infants and children: a survey of current nursing practice. Pediatr Nurs 1998 May-Jun;24(3):229-234.
- 8. Foster H, Ritchey M, Bloom D. Adventitious knots in urethral catheters: report of 5 cases. J Urol 1992 Nov;148(5):1496-1498.
- 9. Pearson-Shaver AL, Anderson MH. Urethral catheter knots. Pediatrics 1990 May;85(5):852-854.
- 10. Arda İS, Özyaylali I. An unusual complication of suprapubic catheterization with Cystofix: catheter knotting within the bladder. Int J Urol 2001 Apr;8(4):188-189.
- 11. Harris VJ, Ramilo J. Guide wire manipulation of knot in a catheter used for cystourethrography. J Urol 1976 Oct;116(4):529.
- 12. Dogra PN, Nabi G, Goel R. Endoscopic removal of knotted urethral catheter: a point of technique. Urol Int 2003;71(1):8-9.
- 13. Taneja SS, Shah O. Complications of Urologic Surgery E-Book: Prevention and Management 5th Edition. Amsterdam, Netherlands: Elsevier Health Sciences, 2017.