Bell’s palsy, also known as acute peripheral facial palsy of unidentified reason, is caused by the acute onset of problems with the facial nerve’s lower motor neuron (LMN).1 Several etiologies have been proposed to explain facial nerve palsy (FNP). Some emphasize that this is due to a viral infection that results in inflammation. Some studies revealed herpes simplex virus (HSV) as the likely cause of most cases of Bell’s palsy.2 However, other viruses might be responsible for this phenomenon. Furthermore, recent studies have shown that COVID-19 or SARS-CoV-2 infection might also lead to neurological symptoms. In the course of the COVID-19 pandemic, several neurological manifestations of the disease have been reported, and there are still many unknown aspects. The possibility of COVID-19 as a cause of Bell’s palsy should be considered. The neurologic manifestations of COVID-19 most commonly include myalgia, headache, altered sensorium, hyposmia or anosmia, and hypogeusia or dysgeusia.3 But, COVID-19 can also present with other central nervous system manifestations such as stroke, encephalo-myelitis, or peripheral nervous manifestations such as Guillain-Barré syndrome (GBS) and Bell’s palsy. Here, we present a COVID-19 patient who developed Bell’s palsy.
Case report
A 64-year-old woman with type 2 diabetes presented to the neurology department with abrupt onset left hemifacial weakness. She did not mention any preceding malaise, fever, myalgia, arthralgia, respiratory, or gastrointestinal symptoms, but she complained of a new-onset headache. Her medical history was not significant, but she reported close contact with her husband, who was hospitalized for COVID-19 pneumonitis. On admission, her vital signs were stable, with oxygen saturation (SpO2) of 97%. On exam, her left hemifacial expression ability was impaired so that her face seemed asymmetrical during smiling, and numbness around the left nasolabial fold was detected [Figure 1]. Her ability to wink was impaired, and her eyebrow drooped, but her speech had not changed. No lymphadenopathy or rigor was found. Other neurological exams were normal. Her extremities forces were of full strength with no focal neurological deficit.
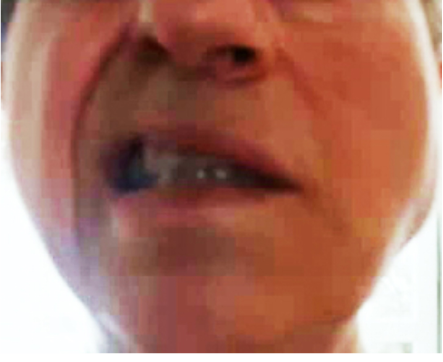
Figure 1: Face of 64-year-old patient who presented to the neurology department with abrupt onset left hemifacial weakness. Her face was asymmetrical during smiling, and she had numbness around the left nasolabial fold.
Her laboratory tests, including HIV antibody and serologic tests of HSV and varicella-zoster virus were negative for active disease. Brain computed tomography (CT) scans and brain magnetic resonance imaging (MRI) did not show abnormalities. However, a lung CT scan was performed because of the current COVID-19 pandemic and the patient’s history of close contact with a confirmed COVID-19 case. Some patients with COVID-19 have a clear and typical involvement of the disease in pulmonary CT scan, although they have no signs of pulmonary involvement, so in some cases, CT is used as a diagnostic tool for the disease. Our patient demonstrated bilateral ground-glass opacity (GGO), indicative of COVID-19 on CT. The patient underwent specimen collection for real-time reverse-transcriptase polymerase chain reaction (RT-PCR) for SARS-CoV-2, which confirmed COVID-19 infection. Also, the anti-SARS-CoV-2 IgM titer was higher than the upper limit of normal (ULN), suggesting recent COVID-19 infection.
A diagnosis of FNP in the setting of COVID-19 infection was made; therefore, the patient was advised to take precautionary isolation measures, along with antiviral medications lopinavir/ritonavir (Kaletra) 400 mg BID and dexamethasone 4 mg BID. At two week follow-up, her symptoms had improved significantly, with a reduced degree of her facial weakness and complete recovery of her smell and taste. One month later, her facial palsy improved but was not resolved, and her repeated nasopharyngeal COVID19 RT-PCR was negative. We then lost the patient to follow-up.
Discussion
Bell’s palsy presents with abrupt onset of unilateral weakness of the face. FNP can be partial or complete. Facial paralysis is either due to a central pathology in the upper motor nerves above the pons or a peripheral lesion of the seventh cranial nerve below the pons.4 The hallmark to distinguish between these two conditions is the involvement of the upper face in the peripheral type and sparing of this anatomic region in the central type. Our patient seemed to be involved with the peripheral type.
Peripheral FNP can be either idiopathic (Bell’s palsy) or secondary to underlying reasons. The most common underlying causes of secondary FNP include infections, surgery, trauma, autoimmune disorders, cancer, or medications.5 Our patient’s precipitating factor appeared to be COVID-19 infection. However, due to the absence of any symptoms attributable to this infection, CT scan findings and serology test results might have been mere incidental findings of asymptomatic COVID-19 infection, with no association with her Bell’s palsy.
Infections are among the most prevalent causes of FNP. The most well-known cause has been reactivation of latent HSV from the seventh cranial nerve ganglion leading to inflammation. SARS-CoV-2 in the current pandemic has been manifested by a broad range of symptoms such as various neurological complications. Some of these complications include cerebrovascular accidents, GBS, encephalopathies, and encephalitis.6 Up to now, COVID-19 as an underlying reason for Bell’s palsy has been reported rarely. A broad differential diagnosis exists for peripheral FNP. Not considering her lung CT scan and serology test results, the most common underlying condition might have been HSV and HZ infections, which are usually accompanied by severe pain and sometimes cutaneous eruptions.7 Our patient did not demonstrate any listed above symptoms. However, cerebrovascular events, either primary or in the context of COVID-19 must be considered in these conditions. Our patient had no risk factors of cerebral ischemia or hemorrhage, and her consciousness, extremity motor, and sensory exams were intact. Furthermore, malignancies of the head and neck region should be considered, which may manifest as inflammation and resulting compression of cranial nerves. But neither was presented in our patient.
Brain MRI may demonstrate facial nerve enhancement in Bell’s palsy, although we saw no abnormality in our patient.8 MRI and cerebrospinal fluid (CSF) analysis might be beneficial in investigating the presence and causes of FNP. Nevertheless, FNP is mainly diagnosed on a clinical basis, similar to our patient who had inconclusive imaging results and did not consent to lumbar puncture. Only history and physical exam helped us make a diagnosis. Electrodiagnostic testing is beneficial in differentiating the severity of nerve fibers involvement and conduction impairment. The electromyography (EMG) and nerve conduction velocity (NCV) testing of the facial nerve in our patient revealed abnormality of the left facial nerve.9
The treatment with corticosteroids is the most widely accepted medication for Bell’s palsy.10 Steroids exert their maximum benefit when administered as soon as possible, preferably within three days of FNP onset. However, their benefit in the settings of COVID-19 is somehow controversial. In the recent case, we agreed to try a short course of prednisolone treatment, along with being aware of the potential adverse effects of COVID-19 infection. Our patient received 60 mg of oral prednisone per day, started on the second day of admission. With tight blood glucose control, we tapered the prednisolone dose after the sixth day of treatment, up to the total ten days of therapy.
It is not yet agreed upon to add antiviral agents to corticosteroids for FNP treatment in the setting of HSV infection; however, many believe the additional efficacy of antivirals in FNP treatment.10 In our patient, our primary purpose for starting on Kaletra was preventing further SARS CoV-2 replication.
Conclusion
During the current COVID-19 epidemic, any newly occurred neurological symptom or sign should raise the suspicion of COVID-19. Therefore, being aware of these complications is vital to prevent any delay in the diagnosis and treatment.
Disclosure
The authors declared no conflicts of interest. The patient gave his consent for the information about himself to appear in a journal article.
Acknowledgements
All of the authors wish to thank all the staff of Kermanshah University of Medical Sciences affiliated hospitals.
references
- 1. Yoo MC, Soh Y, Chon J, Lee JH, Jung J, Kim SS, et al. Evaluation of Factors Associated With Favorable Outcomes in Adults with Bell Palsy. JAMA Otolaryngol Head Neck Surg 2020 Mar;146(3):256-263.
- 2. Zhao H, Zhang X, Tang YD, Zhu J, Wang XH, Li ST. Bell’s Palsy: Clinical Analysis of 372 Cases and Review of Related Literature. Eur Neurol 2017;77(3-4):168-172.
- 3. Balkhair A, Al Jufaili M, Al Wahaibi K, Al Riyami D, Al Azri F, Al Harthi S, et al. “Virtual Interdisciplinary COVID-19 Team”: A Hospital Pandemic Preparedness Approach. Oman Med J 2020 Oct;35(6):e190.
- 4. Toulgoat F, Sarrazin JL, Benoudiba F, Pereon Y, Auffray-Calvier E, Daumas-Duport B, et al. Facial nerve: from anatomy to pathology. Diagn Interv Imaging 2013 Oct;94(10):1033-1042.
- 5. Toulgoat F, Sarrazin JL, Benoudiba F, Pereon Y, Auffray-Calvier E, Daumas-Duport B, et al. Facial nerve: from anatomy to pathology. Diagn Interv Imaging 2013 Oct;94(10):1033-1042.
- 6. Owusu JA, Stewart CM, Boahene K. Facial Nerve Paralysis. Med Clin North Am 2018 Nov;102(6):1135-1143.
- 7. Shah S, Singaraju S, Einstein A, Sharma A. Herpes zoster: A clinicocytopathological insight. J Oral Maxillofac Pathol 2016 Sep-Dec;20(3):547.
- 8. Gupta S, Mends F, Hagiwara M, Fatterpekar G, Roehm PC. Imaging the facial nerve: a contemporary review. Radiol Res Pract 2013;2013:248039.
- 9. Yamout B, Zaytoun G, Nuweihed I. The role of facial nerve conduction studies and electromyography in predicting the outcome of Bell’s palsy. Eur J Neurol 2011;4:348-351 .
- 10. Numthavaj P, Thakkinstian A, Dejthevaporn C, Attia J. Corticosteroid and antiviral therapy for Bell’s palsy: a network meta-analysis. BMC Neurol 2011 Jan;11:1-1.