The incidence and mortality of cancer are rapidly growing worldwide. Lung cancer is not an exception. Despite being a preventable disease, as more than 85% of the cases are caused by smoking, the incidence of lung cancer has increased in many countries since 1987 due to the increase in smoking prevalence.1 Globally, lung cancer is the most commonly diagnosed cancer and the leading cause of cancer death for both sexes combined. It is also the most commonly occurring cancer in men and the third most commonly occurring cancer in women.2 In 2018, 2.1 million new lung cancer cases and 1.8 million lung cancer-related deaths (representing close to 1 in 5 (18.4%) cancer deaths) were reported.2 The association of lung cancer with smoking is strong, dose-related, and is evident for all types of lung cancer, which emphasizes the causal nature of the relationship.3 Despite the high prevalence of cigarette and water-pipe smoking in Gulf Cooperation Council (GCC) countries, a significant challenge is obtaining accurate data about lung cancer incidence due to the lack of comprehensive, up-to-date population registries.1 In Qatar, tobacco use remains a significant public health concern, with an estimated smoking prevalence of 36.5%.4 Furthermore, like in many other GCC countries, the water-pipe smoking epidemic is on the rise and is replacing cigarettes as the most popular method of tobacco use, particularly among youths.5,6 In 2010, Ibrahim et al,7 first reported the clinical and epidemiological characteristics of lung cancer in Qatar from 1998 to 2005. The age-standardized incidence rate (ASIR) over the study period was estimated to be 8.95 per 100 000 persons for the total population (15.20 per 100 000 for males and 3.95 per 100 000 for females).7 Since, Qatar has witnessed a significant reform in its health system, including the care of cancer patients. In 2011, the National Cancer Strategy was published with the aim to deliver a high standard of care to cancer patients across the country.8 The National Center for Cancer Care and Research (NCCCR), a well-equipped and sophisticated center, has been established as the premier healthcare facility to deliver such care for all cancer patients in the country. Our study aimed to report the trends in lung cancer epidemiological and clinical characteristics since the publication of the National Cancer Strategy and compare the results with the previously reported data in 2010.7
Methods
This was a retrospective cohort study documenting the epidemiological and clinical characteristics of all primary lung cancer cases diagnosed from 1 January 2011 to 31 December 2018 in Qatar. Patients with lung metastasis due to primary malignancy originating outside the lungs were excluded.
Data related to lung cancer epidemiological and clinical characteristics during the study period were obtained from two primary sources; the Qatari National Cancer Registry Database and extensive search of the patient’s electronic medical records. Considering the challenges encountered in many international cancer registries regarding the quality, reliability, and completeness of cancer registration data, we performed an extensive search in patients’ electronic medical records to confirm the consistency and completeness of the information obtained from the registry. Utilizing the patient’s medical records and the cancer registry data, patients in our study were censored until any of the following happened (a) a patient died, (b) a patient has not yet died by the time of the close of the study, or (c) the time of the last follow-up if a patient was lost to follow-up. All data were recorded in a structured data collection sheet.
To ensure consistency of the data, all investigators involved in data collection received prior training on how to complete the datasheet. Furthermore, two senior investigators (WI and KS) independently reviewed the data collected by other investigators for accuracy and reliability.
Qualitative and quantitative data were expressed as the frequency with percentage and mean±standard deviation (SD) with median and range. Descriptive statistics were used to summarize the demographic and all other clinical characteristics of the participants. Associations between at least two qualitative or categorical variables were assessed using the chi-squared test. For small cell frequencies, the chi-squared test with a continuity correction factor or the Fisher’s exact test was applied. Pictorial presentations of the key results were made using appropriate statistical graphs. Incidence and mortality rates were expressed as new cases per 100 000 person-years with 95% confidence intervals (CIs) and age standardization using the World Health Organization world standard population 2000–2025. Survival tables and Kaplan-Meier curves were utilized to calculate both one- and three-year survival probabilities with log-rank analysis to compare the variables. A Poisson regression model was used to test the time trend in five-year relative survival. A two-sided p-value < 0.050 was considered statistically significant. Statistical analyses related to demographic and subject characteristics were performed using SPSS Statistics (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp.). Mortality and survival statistics were computed using StataCorp (StataCorp. 2015. Stata Statistical Software: Release 14. College Station, TX: StataCorp LP.).
Results
Table 1: Demographic characteristics of lung cancer patients, N = 428.
|
Age, years |
|
< 40 |
30 (7.0) |
|
40–49 |
64 (15.0) |
|
50–59 |
115 (26.9) |
|
60–69 |
125 (29.2) |
|
70–79 |
71 (16.6) |
|
80+ |
23 (5.4) |
|
Gender |
|
Male |
337 (78.7) |
|
Female |
91 (21.3) |
|
Nationality |
|
Qatari |
89 (20.8) |
|
Non-Qatari |
339 (79.2) |
|
Smoking history (n = 387) |
|
Yes |
257 (66.4) |
|
Number of cigarettes smoked per day for smokers (n = 156) |
|
Average |
26.0 |
|
1–10 |
24 (15.4) |
|
11–20 |
77 (49.4) |
|
21–30 |
7 (4.5) |
|
> 30 |
48 (30.8) |
|
Duration of smoking, years (n = 172) |
|
Mean ± SD |
30.0 ± 13.0 |
|
Median |
30 |
|
Minimum |
2 |
|
Maximum |
73 |
|
Smoking history by gender (n = 387), p-value ≤ 0.001 |
|
Yes |
|
|
Males |
235 |
|
Females |
22 |
|
No |
|
|
Males |
71 |
Table 2: Clinical characteristics of lung cancer patients.
|
Cough (n = 407) |
279 (68.6) |
|
Hemoptysis (n = 404) |
83 (20.5) |
|
Dyspnea (n = 404) |
188 (46.5) |
|
Chest pain (n = 406) |
174 (42.9) |
|
Hoarseness of voice (n = 401) |
21 (5.2) |
|
Malaise (n = 400) |
98 (24.5) |
|
Weight loss (n = 398) |
132 (33.2) |
|
Symptoms related to distant metastasis (n = 402) |
216 (53.7) |
|
Asymptomatic (n = 404) |
31 (7.7) |
|
Finger clubbing (n = 363) |
15 (4.1) |
|
SVC obstruction (n = 404) |
21 (5.2) |
|
Hypercalcemia (n = 414) |
51 (12.3) |
|
Lung involved (n = 418) |
|
Right |
237 (56.7) |
|
Left |
150 (35.9) |
|
Both |
31 (7.4) |
|
Method of diagnosis (n = 383) |
|
Bronchoscopy |
131 (34.2) |
|
CT guided biopsy of the lung lesion |
184 (48.0) |
|
VATS lung biopsy |
17 (4.4) |
|
Pleural biopsy |
27 (7.0) |
|
Mediastinoscopy |
3 (0.8) |
|
Biopsy from distant metastasis |
17 (4.4) |
|
Thoracocentesis |
4 (1.0) |
|
Treatment received |
|
Surgery (n = 375) |
86 (22.9) |
|
Chemotherapy (n = 377) |
259 (68.7) |
|
Radiotherapy (n = 370) |
164 (44.3) |
SVC: superior vena cava; CT: computed tomography; VATS: video-assisted thoracic surgical.
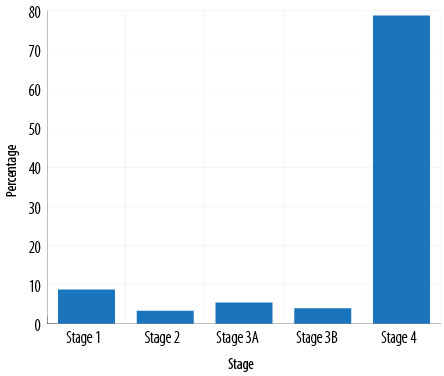
Figure 1: Stage of lung cancer at the time of diagnosis.
Table 3: Associations between the three main histologic types and other variables.
|
Smoking history |
|
Yes |
122 |
48 |
25 |
≤ 0.001 |
|
No |
92 |
8 |
5 |
|
Gender |
|
Male |
172 |
61 |
25 |
≤ 0.001 |
|
Female |
66 |
1 |
6 |
|
Nationality |
|
Qatari |
38 |
19 |
7 |
0.030 |
|
Non-Qatari |
200 |
43 |
24 |
|
Lung involved |
|
Right |
141 |
35 |
12 |
0.172 |
|
Left |
73 |
25 |
14 |
|
Both |
18 |
2 |
3 |
|
Stage at diagnosis |
|
Stage 1 |
16 |
3 |
0 |
|
|
Stage 2 |
4 |
2 |
2 |
|
Stage 3A |
7 |
5 |
1 |
|
Stage 3B |
3 |
6 |
1 |
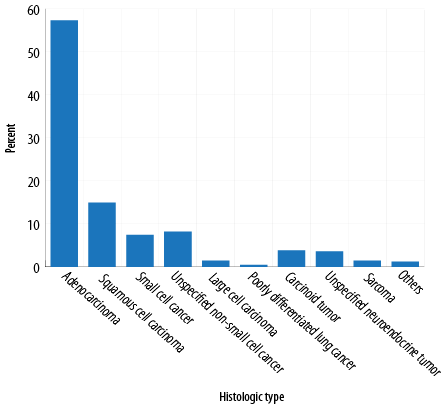
Figure 2: Histologic types of lung cancer.
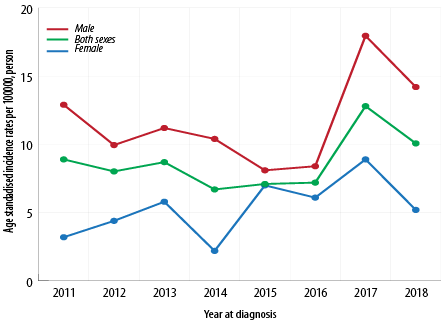
Figure 3: ASIR of lung cancer in Qatar between 2011 and 2018 (per 100 000 person-years).
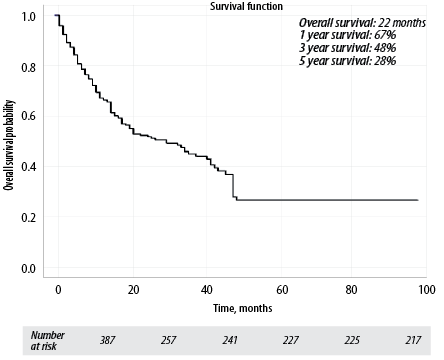
Figure 4: Overall survival of lung cancer patients.
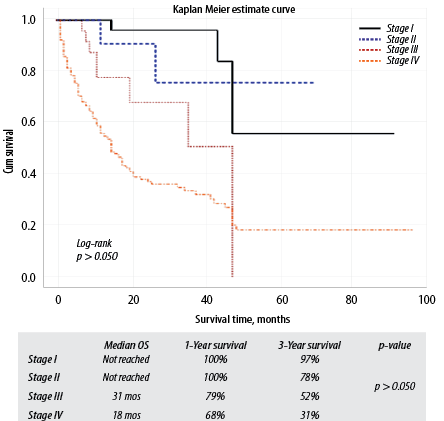
Figure 5: Lung cancer survival by cancer stage.
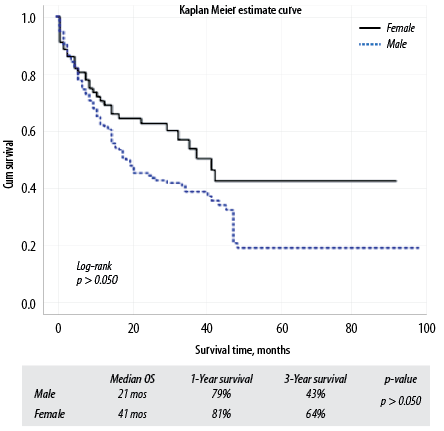
Figure 6: Lung cancer survival by gender.
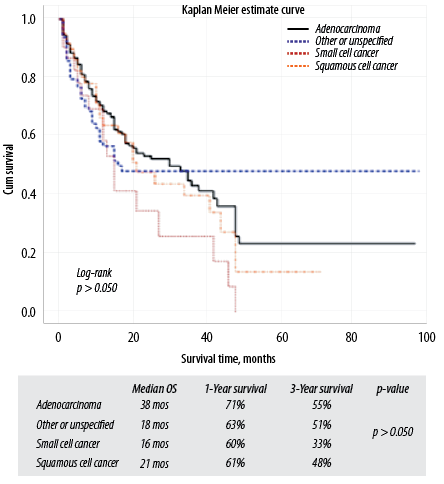
Figure 7: Lung cancer survival by histologic type.
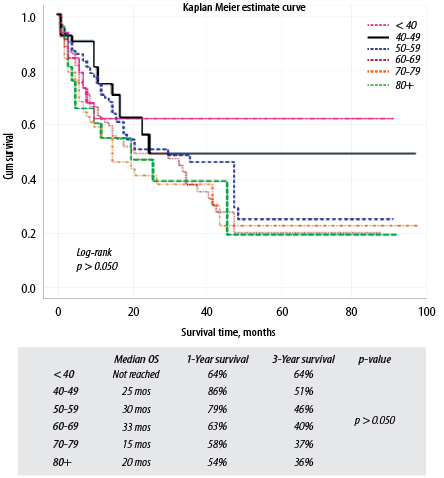
Figure 8: Lung cancer survival by age at diagnosis.
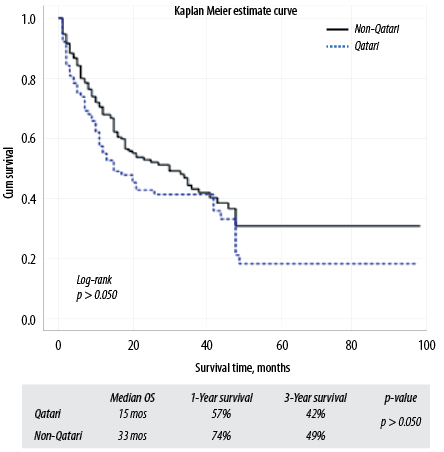
Figure 9: Lung cancer survival by nationality.
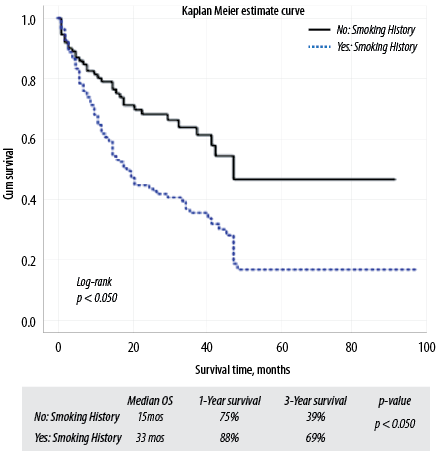
Figure 10: Lung cancer survival by smoking history.
Tables 1 and 2 show the demographic and clinical characteristics of lung cancer patients. A total of 428 patients were diagnosed with lung cancer during the study period. The mean age at diagnosis was 59.6±12.6 years (59.3 years for males and 60.5 years for females). The median age, minimum age, and maximum age at diagnosis were 60 years, 30 years, and 104 years, respectively. Males constituted 78.7% and females 21.3% of lung cancer cases. About 66.4% of patients had a positive history of smoking. Cough was the most common symptom in 68.6% of cases, followed by dyspnea in 46.5%. About 53.7% of patients had symptoms related to distant metastasis at presentation, whereas 7.7% were asymptomatic at the time of diagnosis. Computed tomography (CT) guided biopsy was the most common method of confirming the diagnosis in 48.0% of cases, followed by bronchoscopy in 34.2%. The majority of patients (78.7%) were in stage IV at the time of diagnosis [Figure 1]. Adenocarcinoma was the most common histologic type of lung cancer in 57.4% of cases and the most common in males and females [Figure 2]. About 22.9% of patients received surgical treatment, 68.7% received chemotherapy, and 44.3% received radiotherapy. Targeted therapy was provided to 44.3% of patients with adenocarcinoma [Table 2]. There is a significant association between smoking and the three main histologic types of lung cancer (adenocarcinoma, small cell cancer, and squamous cell cancer) [Table 3].
The overall ASIR was 8.7 per 100 000 persons. The ASIR for males and females were 11.6 per 100 000 and 5.4 per 100 000 persons, respectively [Figure 3]. The median follow-up time was nine months (range 1–89 months). The one, three, and five-year overall survival rates calculated by the Kaplan-Meier method were 67.0%, 48.0%, and 28.0%, respectively [Figure 4]. The three-year overall survival rates for stages I, II, III, and IV were 97.0%, 78.0%, 52.0%, and 31.0%, respectively (p-value = 1.670) [Figure 5]. The three-year survival rates for males and females were 43.0% and 64.0%, respectively (p-value = 0.029) [Figure 6], for adenocarcinoma, small cell cancer, and squamous cell cancer types were 55.0%, 33.0%, and 48.0%, respectively (p-value = 0.088) [Figure 7], for patients < 40 years old was 64.0% [Figure 8], for Qatari and non-Qatari nationals were 42.0% and 49.0%, respectively (p-value = 0.252) [Figure 9], and for smokers and non-smokers were 39.0% and 69.0%, respectively (p-value ≤ 0.001) [Figure 10]. The overall age-standardized mortality rate (ASMR) was 5.5 per 100 000 persons. The ASMR for males and females were 7.6 per 100 000 and 3.1 per 100 000 persons, respectively.
Discussion
Our study has demonstrated some striking features related to the epidemiological and clinical characteristics of lung cancer in Qatar. The overall ASIR of lung cancer remains one of the lowest in the world (8.7 per 100 000 persons), with a noticeable rise in ASIR among females (5.5 per 100 000 persons) compared to the previously published data (3.95 per 100 000 persons).7 Data from the Qatari National Cancer Registry revealed that lung cancer ranked fifth among the most common cancers in Qatar for both sexes from 2009 to 2018, third for men, and eighth for non-Qatari women resident in the country. It was not among the 10 most common cancers for Qatari women. This finding is exciting and may reflect the higher prevalence of smoking among non-Qatari residents in the country.4
Lung cancer does show wide geographic variations in its incidence rates across the world. The highest incidence rates are observed in Micronesia/Polynesia, in Eastern Asia (rates are > 40 per 100 000 persons in China, Japan, and the Republic of Korea), and in much of Europe, especially in Eastern Europe, with an ASIR in Hungary as high as 77.4 per 100 000 males. Incidence rates generally remain low in West and Central Africa (ASIR of 2.8 and 3.1 per 100 000 persons, respectively).2 It is well-known that lung cancer incidence and mortality are tightly linked to cigarette smoking patterns. As smoking rates peak, lung cancer incidence and mortality rise in subsequent decades.9,10 The low incidence of lung cancer despite the previously reported high smoking prevalence in Qatar is a fascinating observation in the current study and is difficult to explain. Nevertheless, this finding is not peculiar to Qatar and has also been observed in many other countries of the GCC and the Middle East and North African (MENA) origin. In some of these countries, smoking rates are even higher than in western countries like the USA and the UK and are comparable with France and Japan. For example, Kuwait has the highest smoking prevalence in the region at 46%, yet the ASIR of lung cancer is only 7.3 per 100 000 persons. In Egypt, where tobacco products are widespread, and approximately 20 billion cigarettes are smoked annually, the ASIR of lung cancer remains low at 7.6 per 100 000 persons.1,11–13 Some plausible explanations for this observation are the younger populations in these countries compared to the high lung cancer risk countries, genetic variations, and the inherited susceptibility theory. A fact that supports the theory of genetic and inherited susceptibility is that lung cancer occurs in only a minority of cigarette smokers, even though cigarette smoking is the predominant cause of lung cancer. Furthermore, a family history of lung cancer has been observed to be a risk factor for lung cancer in non-smoking populations.14 Compared to the previously published data from Qatar in 2010,7 there seems to be a decline in the overall ASIR of lung cancer in men and a rise in women. This finding has also been observed in industrialized countries over the past 40 years. In the USA, the incidence and mortality rates of lung cancer in women have risen markedly and are becoming nearly identical to men’s. Similar trends have also been observed in the UK and central and eastern Europe. Such gender trends have been attributed to the rising tobacco epidemic in these countries, the changes in the histologic pattern over time, and the socioeconomic and educational inequalities.9,15,16 Similar to previous data,7 the current study has shown that adenocarcinoma is the most common histologic type of lung cancer in Qatar. Adenocarcinoma incidence rates have risen and surpassed those of squamous cell carcinoma (historically the most frequent subtype) in many industrialized countries since the 1990s, and its rates continue to increase in populations from other nations. This rise has been in parallel with the increased incidence of lung cancer in women. Different reasons have been postulated to explain the rise in the incidence of adenocarcinoma, including the change in the type of tobacco smoked, genetic predisposition, and environmental exposures.9,17 One of the most striking findings in the current study is the higher survival rates among patients with lung cancer in Qatar than the international figures. Our study’s one, three, and five-year overall survival rates were 67.0%, 48.0%, and 28.0%, respectively. Recent estimates showed that Japan had the highest five-year relative survival worldwide at 30%, while Libya, Mongolia, Chile, Bulgaria, and Thailand had the lowest survival rates of < 10%.18 The five-year lung cancer survival rates in the USA, Canada, France, Germany, Italy, and the UK are 18.7%, 17.3%, 13.6%, 16.2%, 14.7%, and 9.6%, respectively.19 When compared to the neighboring GCC countries, Qatar has a higher lung cancer five-year survival rate. Recent data from Oman revealed a median overall survival of seven months and a five-year survival rate of 7% for non-small cell lung cancer (NSLC).20 In Bahrain, lung cancer five-year survival is only 3%.21 Data regarding lung cancer survival in Saudi Arabia and the UAE are scarce. Nevertheless, the most favorable lung cancer five-year survival for NSLC reported from one tertiary center in Saudi Arabia is 26%.22 Several factors can explain the better survival rates in Qatar compared to other countries, including improved coordination of care of cancer patients at the national level, the timely access to expert opinion and treatment, the utilization of state-of-the-art testing for genetic mutations in NSLC, the availability of sophisticated radiologic investigations, the advanced treatment options that are provided free of charge to all cancer patients resident in the country, and the standardized long-term surveillance of lung cancer survivors.
Our study has described the most recent trends in the epidemiological and clinical characteristics of lung cancer in Qatar and has highlighted some of the outcomes in the care of lung cancer patients following the publication of the National Cancer Strategy in 2011.8 It is the first to describe the details of lung cancer survival and mortality in the country. Among the strengths of this study is the extensive search in the patient’s medical records that was performed to overcome the deficiency in the cancer registry and ensure consistency and accuracy of the collected data. Furthermore, the results of our study can be generalized to the whole country as all patients with lung cancer are referred to and treated in the NCCCR from which the study data were obtained.
Nevertheless, the current study has important limitations. Besides the limitations inherited in retrospective studies, one of the major challenges we encountered during data collection was the incomplete cancer registry database that lacks comprehensive and up-to-date information. Nevertheless, this problem was anticipated at the start, and we decided to search the patient’s electronic medical records as well. Another important limitation is the inability to examine the contribution of water-pipe smoking to the burden of lung cancer. As we highlighted earlier, the prevalence of this type of smoking is on the rise in the country, and it would be interesting if its contribution to the development of lung cancer, particularly among non-Qatari females was examined. The study’s retrospective nature did not permit the examination of smoking and other risk factor characteristics among Qatari and non-Qatari patients, which, in turn, limited proper characterization of the two populations.
Conclusion
Despite the low overall incidence of lung cancer in Qatar, its incidence in females is rising. Lung cancer has a favorable survival in Qatar when compared to other countries. Patients in Qatar have good access to standard and advanced cancer care. Policymakers in Qatar should also consider the changing patterns in lung cancer incidence, such as its rise in non-Qatari women, when planning future preventive strategies. Since many lung cancer patients in the country are diagnosed at advanced stages, early detection programs should be considered. Furthermore, an initiative for a cancer registry improvement program is needed in the country. This program should include training of cancer registry staff and could play a crucial role in ensuring good-quality data and adequate data analysis, interpretation, and dissemination.
Disclosure
The authors declared no conflicts of interest. This research was funded by the Medical Research Council of Hamad Medical Corporation, which had no role in the study design, data collection, analysis and interpretation of data, writing of the report, and the decision to submit the article for publication.
Data availability statement
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request.
references
- 1. Jazieh AR, Algwaiz G, Errihani H, Elghissassi I, Mula-Hussain L, Bawazir AA, et al. Lung cancer in the middle east and north Africa region. J Thorac Oncol 2019 Nov;14(11):1884-1891.
- 2. Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018 Nov;68(6):394-424.
- 3. Lee PN, Forey BA, Coombs KJ. Systematic review with meta-analysis of the epidemiological evidence in the 1900s relating smoking to lung cancer. BMC Cancer 2012 Sep;12:385.
- 4. Al-Mulla A, Bener A. Cigarette smoking habits among the Qatari population. Public health medicine 2003;4(3):41-44.
- 5. Moh’d Al-Mulla A, Abdou Helmy S, Al-Lawati J, Al Nasser S, Ali Abdel Rahman S, Almutawa A, et al. Prevalence of tobacco use among students aged 13-15 years in Health Ministers’ Council/Gulf Cooperation Council Member States, 2001-2004. J Sch Health 2008 Jun;78(6):337-343.
- 6. Mogassabi W, Hassen SS, Mahadik SA, Mubarak RS, Ibrahim WH. Acute and long-term effects of water-pipe smoking on the respiratory system: A narrative review. Ibnosina J Med Biomed Sci 2019;11(4):142-150.
- 7. Ibrahim WH, Rasul KI, Khinji A, Ahmed MS, Bener A. Clinical and epidemiological characteristics of lung cancer cases in Qatar. East Mediterr Health J 2010 Feb;16(2):166-170.
- 8. Ministry of Public Health (The State of Qatar). National cancer framework. [cited 2020 April 13]. Available from: https://www.moph.gov.qa/english/strategies/Supporting-Strategies-and-Frameworks/thenationalcancerFramework/Pages/default.aspx Accessed: April 13th, 2020.
- 9. Barta JA, Powell CA, Wisnivesky JP. Global epidemiology of lung cancer. Ann Glob Health 2019 Jan;85(1):8.
- 10. Youlden DR, Cramb SM, Baade PD. The international epidemiology of lung cancer: geographical distribution and secular trends. J Thorac Oncol 2008 Aug;3(8):819-831.
- 11. Global Health Observatory Geneva: International Agency for Research on Cancer/World Health Organization. Estimated age-standardized incidence rates (World) in 2020, all cancers, both sexes, all ages. 2018 [cited 2020 April 17]. Available from: https://gco.iarc.fr/today/online-analysis-map?projection=globe.
- 12. Hamadeh RR. Smoking in the Gulf Cooperation Council (GCC) countries. Bahrain Med Bull 1998;20(3):91-94.
- 13. World Health Organization. WHO report on the global tobacco epidemic, 2017: monitoring tobacco use and prevention policies. Geneva, Switzerland: World Health Organization; 2017.
- 14. Alberg AJ, Nonemaker J. Who is at high risk for lung cancer? Population-level and individual-level perspectives. Semin Respir Crit Care Med 2008 Jun;29(3):223-232.
- 15. Thun MJ, Carter BD, Feskanich D, Freedman ND, Prentice R, Lopez AD, et al. 50-year trends in smoking-related mortality in the United States. N Engl J Med 2013 Jan;368(4):351-364.
- 16. Freedman ND, Abnet CC, Caporaso NE, Fraumeni JF Jr, Murphy G, Hartge P, et al. Impact of changing US cigarette smoking patterns on incident cancer: risks of 20 smoking-related cancers among the women and men of the NIH-AARP cohort. Int J Epidemiol 2016 Jun;45(3):846-856.
- 17. Lortet-Tieulent J, Soerjomataram I, Ferlay J, Rutherford M, Weiderpass E, Bray F. International trends in lung cancer incidence by histological subtype: adenocarcinoma stabilizing in men but still increasing in women. Lung Cancer 2014 Apr;84(1):13-22.
- 18. Cheng TY, Cramb SM, Baade PD, Youlden DR, Nwogu C, Reid ME. The international epidemiology of lung cancer: latest trends, disparities, and tumor characteristics. J Thorac Oncol 2016 Oct;11(10):1653-1671.
- 19. Allemani C, Weir HK, Carreira H, Harewood R, Spika D, Wang XS, et al; CONCORD Working Group. Global surveillance of cancer survival 1995-2009: analysis of individual data for 25,676,887 patients from 279 population-based registries in 67 countries (CONCORD-2). Lancet 2015 Mar;385(9972):977-1010.
- 20. Furrukh M, Kumar S, Zahid KF, Al-Shamly HS, Al-Jabri ZA, Burney IA, et al. Trends and outcomes of non-small-cell lung cancer in Omani patients: experience at a university hospital. Sultan Qaboos Univ Med J 2017 Aug;17(3):e301-e308.
- 21. Abulfateh NM, Hamadeh RR, Fikree M. Lung cancer epidemiology among the Bahraini population, 1998-2011. Gulf J Oncolog 2018 Jan;1(26):18-22.
- 22. Jazieh AR, Algwaiz G, Alshehri SM, Alkattan K. Lung cancer in Saudi Arabia. J Thorac Oncol 2019 Jun;14(6):957-962.