Accidental foreign body ingestion is more frequently seen in the pediatric age group, where the incident is usually witnessed by a family member or reported by the child.1 However, intentional ingestion was reported in 85% of cases related to adults with psychiatric illness, and 84% occurred in patients who had history of recurrent ingestions.2 Patients with poorly controlled psychiatric conditions are more susceptible to repeated incidences of deliberate self-harm and suicidal attempts.3 The management of those patients is a challenge and requires a multidisciplinary approach to treat and prevent further incidences.4
Multiple factors affect the intervention method for the foreign body ingestion, such as location, nature (sharp versus blunt), and size. However, if it causes complications, like perforations, and affects the patients’ hemodynamic stability, a more invasive intervention will be necessary. Endoscopic retrieval of a foreign body is the most common method used with a success rate of up to 50%.5
Surgical intervention is indicated in cases with failed endoscopy. Laparotomy is the conventional used method. However, laparoscopic retrieval is a new promising era with more trained hands for the laparoscopic approach.6
Case report
A 15-year-old female with known schizophrenia and mental retardation but with good functional capacity presented to the emergency department with a history of foreign body ingestion. She ingested a knife without its handle, with the intention of suicide. She had a history of ingesting a metal object. She was asymptomatic and generally well. There was no abdominal or chest pain, nausea or vomiting, and no signs of bleeding. Her vitals were normal, and she was not in distress. The abdomen was soft, not tender.
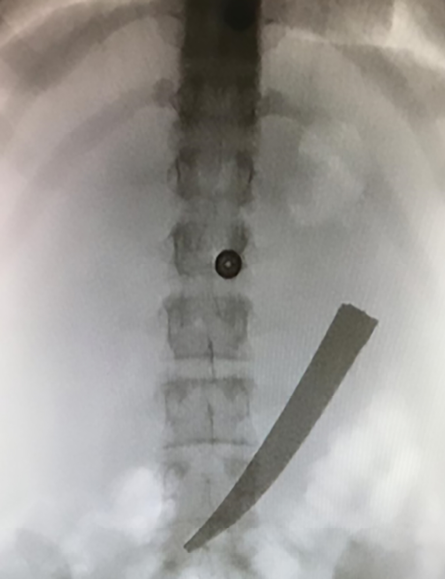
Figure 1: Fluoroscopy revealed a sharp, blunt object in the upper abdomen.

Figure 2: Blunt sharp knife measuring 12 cm retrieved from the stomach of a 15-year-old female.
Fluoroscopy was done and showed a sharp knife, 12 cm long in the stomach [Figure 1]. Diagnostic laparoscopy was performed and showed normal abdominal viscera with no signs of perforation and collection. A small bowel follow through was done, and no perforation or foreign body was observed. The stomach was assessed carefully. It was distended, and after manipulation, a sharp object was found pointing to the greater curvature. A small gastrostomy opening was performed in the antrum, and the sharp object was retrieved carefully and laid above the liver, then gently retrieved out through the umbilical port [Figure 2]. No injuries were detected in the surrounding structures and bowel. The nasogastric tube passed to the stomach, and laparoscopic closure of the gastrostomy was done. Methylene blue was used to assess any probable leak through the nasogastric tube. A drain was inserted through a 5 mm port and kept in the subhepatic area. Postoperatively, the patient remained hemodynamically and vitally stable and was transferred to the psychiatric hospital on day three postoperative because of the high risk of suicidal ideation and poor insight.
Discussion
Unusual and strange foreign body ingestion is more common in patients with psychiatric illnesses. Deliberate self-harm behavior is common in patients with severe personality disorders, post-traumatic stress disorders, and some psychotic disorders.7 The intention of suicide is one of the reasons for this action. As a result, they can present late with complications like choking and obstruction or symptoms suggestive of perforation such as fever, tachycardia, and severe abdominal or chest pain radiating to the back. Investigations to locate and confirm the presence of a foreign body are essential. A plane radiograph with two views can demonstrate the location. On the other hand, contrast study is essential in non-opaque structures.8 A foreign body impacted in the esophagus can be identified if the distance is increased between the cervical vertebrae and the larynges and the trachea or if air is present in the cervical vertebrae.9 Presenting symptoms are the best indicator of the site of impaction and for selecting the appropriate approach in terms of urgency and the method of retrieval.10 Spontaneous passage of the foreign body is observed in most cases, especially in small blunt objects. Endoscopic removal is indicated in 10% to 20% of the patients, whereas surgical removal is indicated in 1% of patients.11 A flexible endoscope can be used to diagnose and treat foreign bodies’ ingestion with a success rate of > 95%.12 However, endoscopic retrieval of sharp and long objects is challenging because of the increased risk of complications like esophageal perforation, which can be fatal, so surgery is considered a safer method for the patient.13 Furthermore, surgical intervention like exploratory laparotomy is considered an option, especially in cases of perforation and unsuccessful endoscopic recovery or when the foreign body is impacted and has remained in the body for a week or more.14 After extraction of the foreign body, post-procedure observation is indicated to assess the patient for signs and symptoms of perforation.
Patients who ingested foreign bodies with the intention of suicide should be evaluated by the psychiatric team to decide if they require further management.
Conclusion
Clinical presentation and the characteristic of the foreign body are the key factors to determine the appropriate approach to avoid any possible complications. Laparoscopic retrieval is considered a safe option in long sharp foreign body ingestion cases. Multidisciplinary management is essential in psychiatric patients presenting with recurrent history of foreign body ingestion.
Disclosure
The authors declared no conflicts of interest. Informed consent was obtained from the patient's legal guardian.
references
- 1. Jayachandra S, Eslick GD. A systematic review of paediatric foreign body ingestion: presentation, complications, and management. Int J Pediatr Otorhinolaryngol 2013 Mar;77(3):311-317.
- 2. Palta R, Sahota A, Bemarki A, Salama P, Simpson N, Laine L. Foreign-body ingestion: characteristics and outcomes in a lower socioeconomic population with predominantly intentional ingestion. Gastrointest Endosc 2009 Mar;69(3 Pt 1):426-433.
- 3. Grimes IC, Spier BJ, Swize LR, Lindstrom MJ, Pfau PR. Predictors of recurrent ingestion of gastrointestinal foreign bodies. Can J Gastroenterol 2013 Jan;27(1):e1-e4.
- 4. Poynter BA, Hunter JJ, Coverdale JH, Kempinsky CA. Hard to swallow: a systematic review of deliberate foreign body ingestion. Gen Hosp Psychiatry 2011 Sep-Oct;33(5):518-524.
- 5. Dalal PP, Otey AJ, McGonagle EA, Whitmill ML, Levine EJ, McKimmie RL, et al. Intentional foreign object ingestions: need for endoscopy and surgery. J Surg Res 2013 Sep;184(1):145-149.
- 6. Omejc M. Laparoscopic removal of an ingested pin migrating into the liver. Surg Endosc 2002 Mar;16(3):537.
- 7. Santa Mina EE, Gallop RM. Childhood sexual and physical abuse and adult self-harm and suicidal behaviour: a literature review. Can J Psychiatry 1998 Oct;43(8):793-800.
- 8. Mosca S, Manes G, Martino R, Amitrano L, Bottino V, Bove A, et al. Endoscopic management of foreign bodies in the upper gastrointestinal tract: report on a series of 414 adult patients. Endoscopy 2001 Aug;33(8):692-696.
- 9. Saki N, Nikakhlagh S. An overview of 11-year experience on opaque esophageal foreign bodies in adults. International Journal of Pharmaceutical Research & Allied Sciences 2016;5(2):159-164.
- 10. Al-Qudah A, Daradkeh S, Abu-Khalaf M. Esophageal foreign bodies. Eur J Cardiothorac Surg 1998 May;13(5):494-498.
- 11. Bendig DW, Mackie GG. Management of smooth-blunt gastric foreign bodies in asymptomatic patients. Clin Pediatr (Phila) 1990 Nov;29(11):642-645.
- 12. Carp L. Foreign bodies in the intestine. Ann Surg 1927 Apr;85(4):575-591.
- 13. Ambe P, Weber S, Schauer M, Knoefel W. Swallowed foreign bodies in adults. Deutsches Ärzteblatt International 2012 Dec;109(50):869.
- 14. Webb WA. Management of foreign bodies of the upper gastrointestinal tract: update. Gastrointest Endosc 1995 Jan;41(1):39-51.