A 52-year-old man with no comorbidities was seen in the emergency department with a two-day history of right-sided dull aching, non-radiating upper abdominal pain. He had no symptoms of liver or peptic ulcer disease. His general examination was unremarkable. Abdominal examination revealed a palpable, non-tender, hard gall bladder (GB). Carcinoma of the GB was suspected, and the patient was investigated. Liver function tests (LFTs) were normal, and ultrasonography (USG) and computed tomography (CT) of the abdomen revealed a calcified structure in the GB fossa [Figure 1]. He underwent an uneventful laparoscopic cholecystectomy. Intraoperatively, the GB was stony hard with a thick and fibrosed wall. The GB lumen was occupied by a large gall stone [Figure 2]. Histopathology revealed a calcified, fibrotic GB with chronic inflammation with no evidence of dysplasia or neoplastic change. He made a good postoperative recovery and has been kept under close follow-up, and after three years, is asymptomatic and doing well.
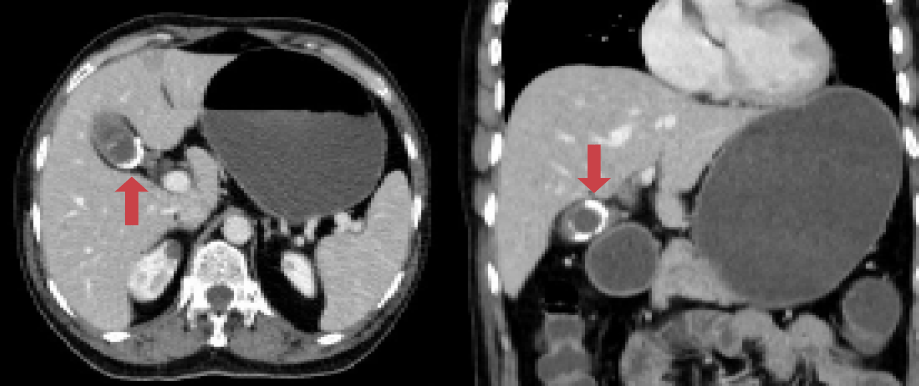
Figure 1: Axial and coronal CT showing a calcified structure in the gall bladder fossa (red arrows).

Figure 2: Large gall stone that occupied the whole gall bladder lumen.
Question
What is most likely the diagnosis?
a. Porcelain gall bladder.
b. Chronic calculous cholecystitis.
c. Gall bladder empyema.
d. Periampullary carcinoma.
Answer
a. Porcelain gall bladder.
Discussion
Dystrophic calcification of the GB, predominantly occurring in middle-aged, obese women, is termed as porcelain GB (PGB). Though disorders of calcium metabolism are implicated, the exact cause of PGB is not known, and it has gained importance only because it has been considered as a premalignant condition for GB cancer and a prophylactic cholecystectomy is indicated in these patients.1 Initial studies showed that the incidence of GB malignancy is around 60% in patients with PGB.2 Schnelldorfer, in a systematic review of the association of PGB with GB cancer, analyzed 111 articles detailing 340 patients with GB wall calcification. The incidence of GB cancer was 21%.3 Surprisingly, the definitive nature of the association between PGB and GB cancer is still uncertain, but the presence of other risk factors (e.g., multiple gallstones, GB polyps, cholecystoenteric fistulae, choledochal cysts) might augment the malignant process. Patients with PGB are usually asymptomatic and frequently diagnosed incidentally when imaging is done for some other reasons. A fraction of patients might present with symptoms of acute cholecystitis (AC).2 The timing of surgical intervention depends on the duration of the acute process. A plain X-ray of the abdomen (AXR) might show a calcified GB, but for a definitive diagnosis, an USG and CT of the abdomen is required.1
Calculous cholecystitis is a common differential diagnosis in patients with right hypochondriac pain and can be confirmed by an USG of the abdomen, which usually reveals multiple stones. AXR, in the majority of the cases, will be negative as only 10% of gall stones are radio-opaque. However, in chronic calculous cholecystitis, GB will not be palpable as it is fibrotic and shrunken.1,3 GB empyema occurs when a stone blocks the cystic duct and the contained GB bile gets infected. It is an acute condition, and patients usually present with symptoms and signs of AC with a tender palpable GB and sepsis. USG of the abdomen is usually conclusive, and either an emergency cholecystectomy or decompression of the GB has to be done.4 Periampullary carcinoma with a palpable GB is not uncommon in male patients. Though the GB is enlarged and clinically palpable, LFTs will be deranged with deep jaundice. A contrast-enhanced CT of the abdomen is required to assess the tumor operability.5
references
- 1. Gupta S, Jauhari RK. Rare presentation of porcelain gall bladder: carcinoma gall bladder with a large intra-abdominal cystic swelling. BMJ Case Rep 2012 Oct;2012:bcr2012006894.
- 2. Goel A, Agarwal A, Gupta S, Bhagat TS, Kumar G, Gupta AK. Porcelain Gallbladder. Euroasian J Hepatogastroenterol 2017 Jul-Dec;7(2):181-182.
- 3. Schnelldorfer T. Porcelain gallbladder: a benign process or concern for malignancy? J Gastrointest Surg 2013 Jun;17(6):1161-1168.
- 4. Khan ML, Abbassi MR, Jawed M, Shaikh U. Male gender and sonographic gall bladder wall thickness: important predictable factors for empyema and gangrene in acute cholecystitis. J Pak Med Assoc 2014 Feb;64(2):159-162.
- 5. Siddique K, Ali Q, Mirza S, Jamil A, Ehsan A, Latif S, et al. Evaluation of the aetiological spectrum of obstructive jaundice. J Ayub Med Coll Abbottabad 2008 Oct-Dec;20(4):62-66.