|
Introduction
Unstable angina (UA) is defined as bothersome to excruciating angina pectoris that occurs at rest, often lasting >20 minutes and of new onset and/or with a crescendo pattern.1 Rest angina is commonly used to exclude patients from exercise-based cardiac rehabilitation. However, it is this patient subset that may, in fact, benefit most from rehabilitation.2 This case report describes the rehabilitation of a patient who was experiencing rest angina.
Case report
A 42-year-old male presented with anginal chest pain at rest and a history of progressive dyspnea and symptomatology over the last two months. His medical history included a previous (10 months earlier) inferior wall myocardial infarction (ST elevation MI) for which emergent percutaneous transluminal coronary angioplasty was unsuccessfully attempted. He was treated medically but continued to experience anginal symptoms. Coronary angiography revealed a 50% ostial stenosis, 100% occlusion of the mid RCA short segment with discernible collaterals distal to the occlusion and a 50% ostial stenosis of the first diagonal branch (D1). Medical management was advised in view of the above-referenced coronary morphology. Echocardiographic studies, at that time, revealed mild systolic dysfunction with a hypokinetic apex.
On hospital admission, he had class III dyspnea according to the New York Heart Association (NYHA) functional classification and class 4 anginal symptoms. His resting heart rate and blood pressure (BP) were 80 beats per minute (bpm) and 140/90 mmHg, respectively. A systemic evaluation revealed basal crackles bilaterally with an S3 gallop. His resting ECG showed marked ST depression (>2 mm) in the anterolateral leads. Other clinical studies were within normal limits. He was treated with nitrates, antiplatelet agents, diuretics, beta-blockers and ACE inhibitors and referred to physical therapy for exercised-based cardiac rehabilitation.
The patient was initially examined (Day 0) by a physical therapist and had a resting pulse rate of 80 bpm and BP of 120/80 mmHg. At this time, he described episodes of angina which occurred during minimal exertion. His rate-pressure product (RPP), (i.e., pulse rate × systolic BP) at the onset of anginal symptoms was 9360 (i.e., 78 × 120), (Table 1). A six-minute walk test (6 MWT) could not be conducted at this point in time as the patient was still experiencing rest angina. With the patient asymptomatic on Day 2, the 6 MWT was conducted; however, it was prematurely terminated after 1.5 min because of anginal symptoms. The ECG revealed no additional ST segment displacement. Rehabilitation goals were to increase his anginal threshold, walking distance and functional capacity. The risks and benefits of an exercise rehabilitation program were explained to the patient and informed consent was obtained.
Table 1: Summary of the exercise program with outcomes and six minute walk test.HR - heart rate; BP- blood pressure; RPP - rate-pressure product; 6 MWT - Six-minute walk test.
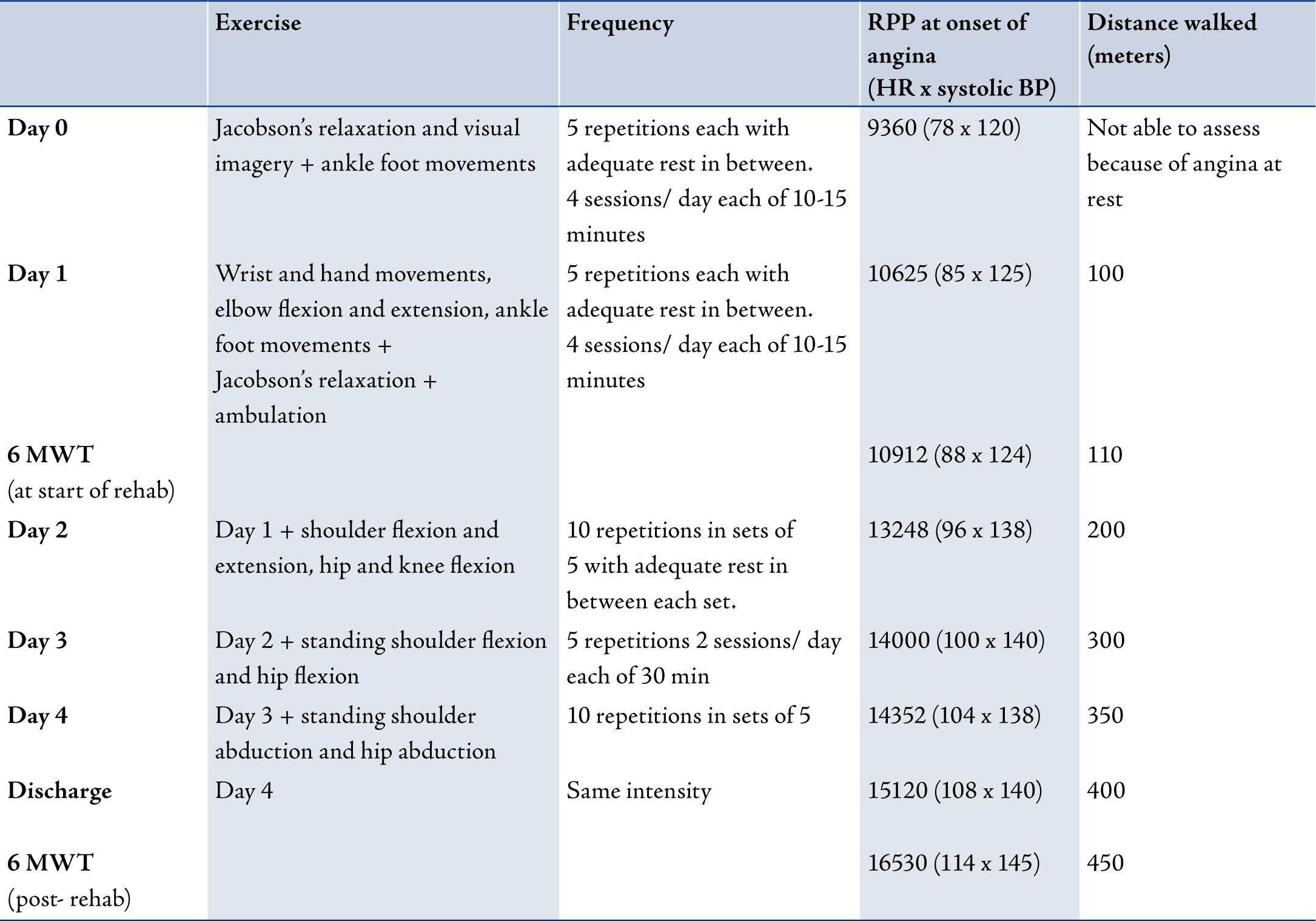
Exercise began with low-level aerobic exercises of the upper and lower limbs at an intensity that was below his anginal threshold. The repetitions were gradually progressed to ensure the patient remained symptom free during the exercise regimen. As adjunctive therapy, relaxation using Jacobson’s technique, breathing and visual imagery were taught to help him manage his anginal episodes. Brief sessions of 10 to 15 minutes in duration, 4 times a day were implemented.
The patient was discharged in 8 days after having completed another 6 MWT. The test was terminated with the onset of chest pain after 3.5 minutes, having covered a distance of 400 m. His symptom-limited RPP was ~ 15,000 at this point in time. The ECG showed no signs of exercise induced myocardial ischemia, and the patient was referred to a home-based rehabilitation program. He was counseled to continue brisk walking for two minutes twice a day and gradually encouraged to progress the weekly walking distance as tolerated. Patient education regarding the taking of sublingual nitroglycerin and recognition of adverse signs and symptoms was given. Follow up telephone interviews were conducted every week.
At four and eight weeks follow up, he was asymptomatic and ambulant in the community. His exercises were progressed and he was encouraged to continue them until his next follow up. At six months, he was no longer plagued by anginal symptoms and was able to walk 1 km a day. At nine months follow up, he had class 2 anginal symptoms. Although he was compliant with his medications and was still able to walk 1 km a day, he had stopped exercising.
Discussion
The primary aim of exercise rehabilitation in chronic stable angina is to increase the ischemic threshold so that higher levels of physical exertion can be undertaken before the onset of limiting symptoms. Angina management programs have been shown to decrease the episodes of chest pain by 70%, reduce nitrate use by 65% and improve exercise tolerance by 57%.3 In this case report, profound increases in the symptom-limited RPP, ischemic threshold and distance walked were observed, (Table 1). The improvement seen cannot be entirely attributed to the exercise rehabilitation program, since the patient was simultaneously treated with an array of anti-anginal medications. However, it appears that the home-based physical conditioning program further improved functional capacity in this patient. Recent guidelines,4 further support the reduced cardiac demands resulting from regular physical activity and exercise-based rehabilitation in patients with exertional angina.
The first widely cited example of exercise being beneficial for symptomatic cardiovascular disease was a case chronicled by William Heberden in 1772, in his writings on angina pectoris:5 "I knew of one case who set himself the task of sawing wood for half an hour each day, and was nearly cured." Thus, Heberden unwittingly documented the first known example of exercise-based cardiac rehabilitation. Although the cause of angina pectoris remained a mystery to Heberden, he identified the cure without knowing the nature of the disease.
The ability of the patient to continue walking 1 km a day at nine months, suggests that the improvement in exercise tolerance was largely maintained, despite symptoms. Nevertheless, whether an increase in functional capacity invariably translates to an improved quality of life remains unclear, and requires future investigation. Larger well-controlled randomized trials are needed to substantiate the favorable adaptations observed in this case report.
Conclusion
Exercise-based cardiac rehabilitation likely benefits symptomatic patients with angina when revascularization is not possible and aggressive medical management is pursued.
Acknowledgements
The authors reported no conflict of interest and no funding was received on this work.
References
1. Libby P, Bonow RO, Mann DL, et al. Braunwald's heart disease: a textbook of cardiovascular medicine 8th ed. Saunders Elsevier, Philadelphia: pg. 1319.
2. Lewin RJ. Improving quality of life in patients with angina. Heart 1999 Dec;82(6):654-655.
3. Lewin RJ, Furze G, Robinson J, et al. A randomized controlled trial of a self-management plan for patients with newly diagnosed angina. Br J Gen Pract 2002; 52:194-196:199-201.
4. Anderson JL, Adams CD, Antman EM, Bridges CR, Califf RM, Casey DE Jr, et al; American College of Cardiology; American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the Management of Patients With Unstable Angina/Non-ST-Elevation Myocardial Infarction); American College of Emergency Physicians; Society for Cardiovascular Angiography and Interventions; Society of Thoracic Surgeons; American Association of Cardiovascular and Pulmonary Rehabilitation; Society for Academic Emergency Medicine. ACC/AHA 2007 guidelines for the management of patients with unstable angina/non ST-elevation myocardial infarction. J Am Coll Cardiol 2007 Aug;50(7):e1-e157.
5. Heberden W. Some account of a disorder of the breast. Medical Transactions of the Royal College of Physicians 1772;2:59-67.
|