|
Diabetes is one of the most widely prevalent diseases with an increasing incidence worldwide. Recent estimates indicate that there were 285 million people aged 20-79 years throughout the world with diabetes in the year 2010, and this number is projected to increase to 439 million by 2030.1 The diabetic population in Pakistan is very high, ranking at number 7 among countries where high number of diabetic cases have been reported.2 in 2007, there were 6.9 million diabetic patients in Pakistan, which is expected to rise by 11.5 million by 2025 according to the International diabetic foundation.2 Good glycemic control can be considered as the cornerstone management in the prevention of diabetic complications. However, it is sometimes difficult for the patients to maintain a healthy lifestyle as standardized, resulting in suboptimal effect and minimal benefit of diabetes therapy due to increased insulin resistance and decreased glucose control, and subsequent diabetic complications.3 WHO recommended that adherence to the medications can promote the population’s health and minimize long-term complications of the disease.4 Lifestyle variables include meal habits, exercise state, drinking state and smoking state. Modification in these factors would result in improved compliance towards hypoglycemic agents.5
Hu et al.6 indicated in their study that decreased physical activity (i.e., watching TV for 2 hr/day) increases the risk of diabetes by as much as 14%, while brisk walking at least 1hr/day decreases the risk of diabetes by 34% as shown in Fig 1.
Fig. 1 clearly emphasizes the need to increase physical activity as a sedentary lifestyle increases the risk of diabetes. This assertion is also supported by another study which revealed that by increasing every 500 K-cal energy expenditure, the risk of type II diabetes mellitus can be reduced by 6%.7 Similarly in Pakistan, obesity is among the major causes of diabetes mellitus and the major reasons of obesity are high energy intake and sedentary lifestyle.8
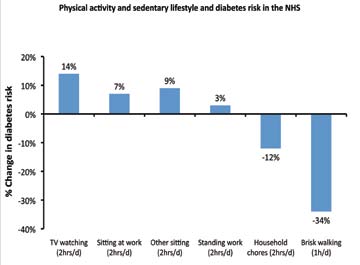
Figure 1: Physical activity and sedentary lifestyle and diabetes riskin the NHS.
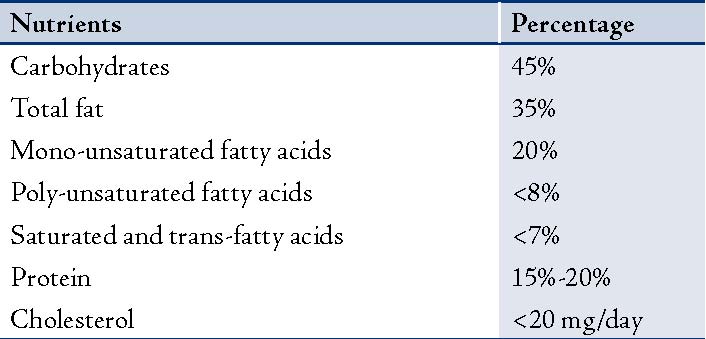
Moreover, WHO has recognized the importance of dietary control in diabetes mellitus and has given its recommendation regarding the distribution of nutrients in diabetic patients.9 This is summarized in Table 1.
Table 1: Recommended distribution of nutrients for diabetic subjects.
A general concept regarding alcohol intake is that it further deteriorates the condition; but interestingly, a Meta-analysis with 12 years of follow up showed that the controlled intake of alcohol (1-2 drinks/day) decreases the risk of diabetes by 30-40% as compared to substantial drinkers.10 It was concluded that moderate amounts of alcohol not only increase the sensitivity of insulin, but also increase HDL cholesterol levels while heavy intake of alcohol increases the triglyceride levels and impair carbohydrate and glucose metabolism. Ahmed et al. also studied the relationship between alcohol consumption and glycemic control and concluded that the relationship is inversely proportional; thus diabetic complications can be minimized by the restricting alcohol consumption.11
Smoking is also highly associated with the increased risk of diabetes mellitus. In their study, Willey et al. found that frequent smokers (≥20 cigarettes/day) were at increased risk of developing diabetes mellitus (relative risk=1.61) compared to occasional smokers (relative risk=1.29).12 The risk was further decreased to1.23 for ex-smokers compared with active smokers.
Diabetes mellitus is one of the most prevalent problems facing our modern civilisation, resulting in numerous complications, which can be effectively controlled by simple means, such as lifestyle modifications. Pharmacological interventions are not always necessary to control diabetes, but emphasis should also be given to non-pharmacological management. Evidence has clearly shown that lifestyle variables are highly associated in determining the relative risk of diabetes mellitus. Hence, by controlling these factors, one can effectively halt the progression of this highly penetrating disease. This can be achieved through the involvement of a multi-disciplinary team, particularly a health provider who can counsel the patient regarding the risk factors associated with diabetes; public health policies can be designed to achieve the desired results and self confidence should also be developed among the patients to improve medication adherence.13
In Pakistan, diabetic patients do not have ample information on the important role of lifestyle changes in glycemic control. There is an uttermost need to educate people in Pakistan regarding the disease and the different management options available; particularly, lifestyle habits. In a recent study conducted in Pakistan; it was revealed that only 11% of diabetic patients took part in education sessions conducted by physicians and healtheducators.14 As healthcare providers, our utmost responsibility is to promote the message of healthy lifestyle among patients with diabetes globally.
Acknowledgements
The authors reported no conflict of interest and no funding wa sreceived for this work.
References
1. Shaw JE, Sicree RA, Zimmet PZ. Global estimates of the prevalence of diabetes for 2010 and 2030. Diabetes Res Clin Pract 2010 Jan;87(1):4-14.
2. International Diabetic Federation Atlas. 2006 showing prevalence of diabetes in 2007 and future projection for 2025 [Internet]. [updated 2009]. Available from: http://www.eatlas.idf.org/index1397.html.
3. Adisa R, Alutundu MB, Fakeye TO. Factors contributing to nonadherence to oral hypoglycaemic medications among ambulatory type 2 diabete spatients in Southwestern Nigeria. Pharmacy Practice (Internet) 2009 Jul-Sep;7(3):163-169 .
4. WHO. Adherence to long-term therapies. Evidence for action. Geneva,World Health Organisation;2003.
5. Park KA, Klim JG, Kim BW, Kam S, Kim KY, Ha SW, Hyun ST. Factors that Affect Medication Adherence in Elderly Patients with Diabetes Mellitus. Korean diabetes Journal 2010;34:55-65.
6. Hu FB, Li TY, Colditz GA, Willett WC, Manson JE. Television watching and other sedentary behaviors in relation to risk of obesity and type 2 diabetes mellitus in women. JAMA 2003 Apr;289(14):1785-1791.
7. Shera AS, Rafique G, Khwaja IA, Ara J, Baqai S, King H. Pakistan national diabetes survey: prevalence of glucose intolerance and associated factors in Shikarpur, Sindh Province. Diabet Med 1995 Dec;12(12):1116-1121.
8. Asif SA, Iqbal R. Ikramullah, Hussain H, Nadeem S. Prevalence of obesity in men and its relationship with diet and physical activity. Gomal Journal of Medical Sciences 2009;7(1):35-38.
9. World Health Organization: Guidelines for the prevention, management and care of diabetes mellitus. EMRO Technical publication series 32, Geneva2006
10. Koppes LL, Dekker JM, Hendriks HF, Bouter LM, Heine RJ. Moderate alcohol consumption lowers the risk of type 2 diabetes: a meta-analysis of prospective observational studies. Diabetes Care 2005 Mar;28(3):719-725.
11. Ahmed AT, Karter AJ, Warton EM, Doan JU, Weisner CM. The relationship between alcohol consumption and glycemic control among patients with diabetes: the Kaiser Permanente Northern California Diabetes Registry. J Gen Intern Med 2008 Mar;23(3):275-282.
12. Willi C, Bodenmann P, Ghali WA, Faris PD, Cornuz J. Active smoking and the risk of type 2 diabetes: a systematic review and meta-analysis. JAMA2007 Dec;298(22):2654-2664.
13. Glasgow RE, Toobert DJ. Brief, computer-assisted diabetes dietary self management counseling: effects on behavior, physiologic outcomes, and quality of life. Med Care 2000 Nov;38(11):1062-1073.
14. Shaikh ZA, Shaikh MZ, Ali G. Diabetic patients; awareness about life style modifications. Prof Med J 2011;18(2):265-268.
|