Cyst of the orofacial region can be grouped into odontogenic and nonodontogenic, epithelial or non-epithelial, and developmental or inflammatory in origin.1,2 Odontogenic cysts, most commonly affecting the jaw, are known as osseous-destructive. Odontogenic cysts are formed as a result of activation of entrapped odontogenic rest cells (Malassez, Serres, or enamel organ) within the jaw bones or gingivae. Activation of rest cells by the inflammatory process gives rise to inflammatory odontogenic cysts.3
Based on diagnosis, jaw cysts distribution is as follows: radicular cysts 56%, dentigerous cysts 17%, nasopalatine duct cysts 13%, odontogenic keratocysts 11%, globulomaxillary cysts 2.3%, traumatic bone cysts 1.0%, and eruption cysts 0.7%.1 In 2005, the World Health Organization (WHO) classified odontogenic keratocyst (OKC) as a keratocystic odontogenic tumor (KCOT). It is of odontogenic origin, intraosseous, uni- or multicystic and lined by potentially aggressive parakeratinized stratified squamous epithelium.1 Odontogenesis of primary and secondary dentition and the three-dimensional growth of the oral and maxillofacial skeleton are some of the developmental processes occurring in the maxillofacial area during childhood involved in cyst formation. In adulthood, secondary dentition may be affected by caries and/or trauma leading to cyst formation.1
True cysts of the orofacial region are those lined with epithelium (e.g., dentigerous cyst) while those not lined by epithelium are referred to as pseudocysts. Typical examples are the solitary and aneurysmal bone cyst and mucous extravasation cyst.4 Cysts, especially epithelial types, are more commonly seen in jaw bones than other parts of the body because of numerous epithelial rests that develop an intimate relationship with developing bone. A search of the literature has revealed various classifications of orofacial cyst.4 There have been few reports on the presentation of cyst in Nigeria. This study analyzes the types and pattern of presentation of 64 cases of orofacial cysts seen in a Nigerian referral center.
Methods
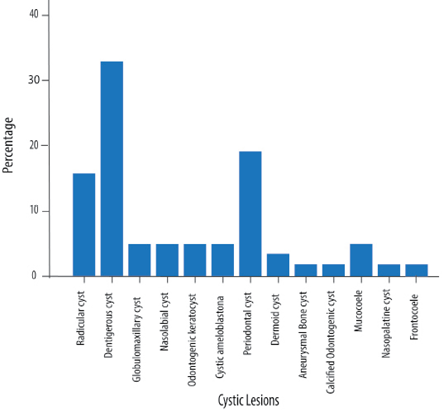
Figure 1: Percentage of cystic lesions by type.
A retrospective study of all orofacial lesion diagnosed histologically as cysts seen at the Maxillofacial Clinic of the Ahmadu Bello University Teaching Hospital, Nigeria, between January 2003 and December 2012 was undertaken. Cysts diagnosed as OKC were included in the study. Information concerning cyst type, age at the time of diagnosis, and gender of patients were retrieved.
Data was analyzed using SPSS Statistics (SPSS Statistics Inc., Chicago, US) version 13. The results were presented as frequencies and percentages for discrete variables, and mean and standard deviation (SD) for continuous variables. Statistical significance was set at a p-value < 0.050.
Results
Table 1: Distribution of cystic lesions of the oral and maxillofacial region according to gender.
|
Radicular cyst |
4 |
6 |
10 |
15.6 |
|
Dentigerous cyst |
15 |
6 |
21 |
32.8 |
|
Globulo-maxillary cyst |
3 |
0 |
3 |
4.7 |
|
Nasolabial cyst |
0 |
3 |
3 |
4.7 |
|
Odontogenic keratocyst |
3 |
0 |
3 |
4.7 |
|
Cystic ameloblastona |
3 |
0 |
3 |
4.7 |
|
Periodontal cyst |
4 |
8 |
12 |
18.8 |
|
Dermoid cyst |
2 |
0 |
2 |
3.1 |
|
Aneurysmal bone cyst |
0 |
1 |
1 |
1.6 |
|
Calcified odontogenic cyst |
0 |
1 |
1 |
1.6 |
|
Mucocoele |
0 |
3 |
3 |
4.7 |
|
Nasopalatine cyst |
0 |
1 |
1 |
1.6 |
|
Frontocoele |
1 |
0 |
1 |
1.6 |
X2 = 23.47; p = 0.002.
Table 2: Distribution of cystic lesions according to age.
|
Radicular cyst |
0 |
4 |
2 |
3 |
1 |
0 |
10 |
15.6 |
|
Dentigerous cyst |
2 |
8 |
7 |
2 |
1 |
1 |
21 |
32.8 |
|
Globulomaxillary cyst |
0 |
0 |
2 |
1 |
0 |
0 |
3 |
4.7 |
|
Nasolabial cyst |
1 |
0 |
0 |
0 |
0 |
2 |
3 |
4.7 |
|
Odontogenic keratocyst |
0 |
1 |
1 |
1 |
0 |
0 |
3 |
4.7 |
|
Cystic ameloblastona |
0 |
1 |
1 |
1 |
0 |
0 |
3 |
4.7 |
|
Periodontal cyst |
1 |
3 |
3 |
2 |
2 |
1 |
12 |
18.8 |
|
Dermoid cyst |
1 |
0 |
0 |
1 |
0 |
0 |
2 |
3.1 |
|
Aneurysmal bone cyst |
0 |
1 |
0 |
0 |
0 |
0 |
1 |
1.6 |
|
Calcified odontogenic cyst |
0 |
0 |
0 |
0 |
1 |
0 |
1 |
1.6 |
|
Mucocoele |
0 |
1 |
1 |
1 |
0 |
0 |
3 |
4.7 |
|
Nasopalatine cyst |
0 |
0 |
1 |
0 |
0 |
0 |
1 |
1.6 |
|
Frontocoele |
0 |
0 |
1 |
0 |
0 |
0 |
1 |
1.6 |
X2 = 56.44; p = 0.801.
Over the 10-year study period, 64 cases of cystic lesions of the orofacial region were seen out in 1162 pathological specimen submitted, representing 5.5%. Of these, there were 35 (54.7%) lesions in males and 29 (45.3%) lesions in females giving a M:F ratio of 1.2:1. The age of the patients ranged from 4–64 years old, with a mean age of 26.3±13.9 years.
The most predominant cyst type was dentigerous (n = 21; 32.8%), followed by periodontal cyst (n = 12; 18.8%) and radicular cysts (n = 10; 15.6%) [Figure 1]. The gender distribution was significant (X2 = 23.5; p = 0.002) with certain lesions such as the dentigerous cysts and OKC having a male predilection. In contrast, periodontal and radicular cysts were found to be more common in females [Table 1]. There was a wide age distribution of the cystic conditions, spanning from the first to the sixth decades of life with more lesions occurring in the second and fourth decades [Table 2]. However, the age group distribution was not significant (X2 = 56.4; p = 0.801).
The most common clinical feature was swelling, which was found in all patients. Others included spontaneous drainage of fluids, infection, pain, teeth mobility, and paresthesia. A combination of these complaints was found in a large number of patients. The majority of radiological appearance images were unilocular (n = 53; 82.8%). Others were unclear since we only used plain radiographs.
All patients underwent marsupialization, cystectomy, and resection. The majority (n = 59; 92.2%) were carried out under general anesthesia and the rest (7.8%) under local anesthesia; 73.4% were odontogenic cysts and 26.6% were nonodontogenic. Of the odontogenic cysts, 78.7% were developmental and 21.3% inflammatory.
Discussion
Cysts of the jaws are either odontogenic or nonodontogenic, developmental, or inflammatory in origin.1
Our study had a male to female ratio of 1.2:1, which was similar to studies conducted in Kano5 (1.4:1), in Enugu6 (1.5:1), and Ibadan4 (1.1:1) in the Northwestern, Southeastern, and Southwestern regions of Nigeria, respectively. In addition, our gender ratio was similar to that of Portuguese,7 Libyan,3 and Indian3 studies (1.4:1, 1.3:1, 1.2:1, respectively). On the other hand, two Brazilian studies reported a slight female preponderance.7,8 Male dominance, especially for radicular cysts, has been associated with increased maxillofacial trauma and poor oral hygiene.9 Although increased risk of maxillofacial trauma is admissible, evidence to support poor oral hygiene in men is weak. Furthermore, early childhood caries would have taken place when there is no significant gender disparity. We observed a significant gender predilection among patients with radicular cysts, and this was corroborated by a Brazilian study.8
The mean age of patients was 26.3 years (range = 4–64 years). This was similar to previous studies conducted in Nigeria and India.3,4 However, the mean was much lower than the mean age of 36.7 years observed by Oti et al2 in Ghana.
Orofacial cysts constituted only 64 (5.5%) of all specimens submitted for histology, and this frequency was slightly higher than the 54 cases in Kano,5 20 cases in Enugu,6 and 92 cases in Ibadan.4 In contrast, the observed prevalence of 5.5% was lower than the prevalence of 8.5% in India,3 9.6% in Ghana,2 10.3% in Italy,10 and 14.3% in Kuwait.11 Most cysts were odontogenic (73.4%), and 26.6% were nonodontogenic. This was lower than the percentage of odontogenic cyst reported in Brazil (96.7%) but higher than the 67.3% reported in Ghana.2 Lower percentages were reported in Canada and the UK (17.2% and 12.8%, respectively).2 A study from Israel reported 81% odontogenic cysts, 10% OKC, and 9% nonodontogenic cysts.1
Of the odontogenic cyst, 78.7% were developmental and 21.3% inflammatory. This was higher than the 51.4% developmental cysts and 48.6% inflammatory cysts reported by Oti et al.2 Manor et al,1 found more inflammatory cysts (48%) than developmental cysts. This was also similar to the results of Lawal et al4 and Monteiro et al7 who also reported more inflammatory cyst (59.8% and 69.5%, respectively). Dentigerous cyst (n = 21; 32.8%) were predominant followed by periodontal cysts (n = 12; 18.8%) and radicular cysts (n = 10; 15.6%). The gender distribution was significant (p = 0.002) with the dentigerous cysts and OKC having a male predilection. This is in agreement study results from Ghana, which found dentigerous cysts to be the most common (27.1%) with a male predilection. 2 Manor et al1 also found that dentigerous cysts were the most common cysts in children (44%) and the second most common type in adults (18%). The study conducted in Ibadan found that dentigerous cysts were only 12% and the second most common.4 Similarly, Iyogun et al5 found dentigerous cysts (48.6%) were the most common, and the second most common in the study from Portugal.7 Dentigerous cysts made up 20.3% of cysts in the study from India.3
OKC represented 4.7% of cysts in our study and had a male predilection. On the contrary, Oti et al2 in Ghana reported OKC at 1.6% with a female predilection. Manor et al1 had a much higher prevalence of 10% in Israel. They were the second most common cyst in Turkey with no male predilection12 and the third most common (12.1%) cyst type in Portugal with a female predilection.7 They made up 5.2% of cysts in the study from India.3
Although there is a consensus that neoplastic features, like high proliferation rate of epithelial cells, are present in OKC, the behavior and management are still controversial. The majority of surgeons advocate a more conservative approach, such as marsupialization and decompression, despite the reclassification of OKC.13 Recurrence can be avoided by complete removal of the cystic lining in and around the region.12
Radicular cysts are inflammatory cysts from the rest cells of Malassez.12 Also called periapical cysts, radicular cysts, are the most common inflammatory cysts and derive from the residues of epithelium after necrosis and death of the pulp from apical periodontitis.3 They represented 15.6% of cysts in this study, which was lower than that reported in Turkey (59%),12 Portugal (48.4%),7 and India (69.3%).3 The study conducted in Ibadan found that these cysts constituted 50% of all inflammatory cysts.4 Commonly found in those aged 20 to 60 years old, radicular cysts are rare in children less than 10 years of age.12 This was corroborated by our findings, with most radicular cysts presenting between the second and fourth decades of life. Radicular cysts were found to be more common in females in this study, which corroborated with Selvamani et al3 but was contrary to Koseoglu et al,12 who found a male preponderance.
Periodontal cysts in this study were the second most common (18.8%) cysts. They constituted 7.6% of cysts in the study from Ibadan.4 According to Monteiro et al,7 these results are more population-based than character-based.
The most common nonodontogenic cysts were globulomaxillary, nasolabial, and mucocele (21.4% each). Oti et al,2 reported a nasolabial cyst as the most common nonodontogenic cyst at 61%, which is far above the 21.4% in this study.
Plain radiographs were adequate for the majority of cysts. The use of computed tomography (CT) with multiplanar program has proven to be more effective in detecting jaw abnormality and pathology and has been advocated.1 It shows a cross-section of anatomical structures (mandibular canal, mental foramen, incisive foramen, and maxillary antrum) and has been used to monitor bone regeneration after cyst marsupialization.1
It has been said that cysts are a result of unintentional findings.7 In this regard, 36.0% of cases by Monteiro et al,7 in India were radiological findings. This was, however, not the case in our study as none of our patients was an accidental finding.
The treatment modalities included marsupialization (n = 2), cystectomy (n = 49), and resection (n = 3). None of our cases had bone grafting. Some patients benefited from the use of Carnoy’s solution for chemical treatment. Ultrasonic surgery has been advocated for cystectomy as it appears safe and effective. It is a new tool with a wide range of indications in oral and maxillofacial surgery. A major controversy surrounding the use of ultrasonic surgery in cystectomy has been the disadvantage of increased operation time.14
Early diagnosis can have a major impact in treatment modality. When lesions are 10 to 15 mm in diameter, and there is an associated tooth, pulpectomy is the treatment of choice. When the lesion persists, or there are signs and symptoms, an apicoectomy is recommended.15 Bearing in mind that lesions 40 to 50 mm in diameter develop in three to four years, even though patients give history of slow growth, early and prompt diagnosis will avoid the risk of pathological fracture, root resorption, and compromising adjacent structures.16 A less than 5% complication rate can be achieved when defects are closed primarily on solid margins together with a course of antibiotics even in more than 3 cm diameter defects. Infection is the major complication, with fracture being rare with a 3% maximum rate when located at the angle.17
In terms of bone regeneration, complete ossification takes about 12 months after cystectomy for defects ≤ 3 cm and 24 months for larger defects.17 Preservation of bone wall and periosteum is the most vital condition for bone healing.17,18 The endosteum seems to have a key role in providing osteoprogenitor cells for spontaneous regeneration of bone from residual walls defects.18 Delay is observed in defects of the anterior maxilla or in circular or bicortical defects in older patients.17,18 An established radiolucent area, a residual fibrous scar is the result of incomplete bone fill.18
In the early healing period, the autologous spongiosa has shown the highest rate of ossification. Early prosthetic rehabilitation with dental implant after cystectomy may be achieved with an iliac bone graft.17 This is a matter of choice as other operators prefer regenerated new bone when dental implants are considered. However, not using bone grafts does not exclude the subsequent resolution with implants.18
Collagen in recent times has been popularized for the stability of blood clot.17 The future treatment is the use of recombinant human bone morphogenetic protein-2(rhBMP-2) either alone or combination with a bone graft.18
Conclusion
Cysts of the orofacial region are common in this environment and like previous Nigerian studies odontogenic cysts are not uncommon, the most predominant being dentigerous cysts. However, our findings differed from previous reports, especially within Nigeria, in that periodontal cysts were the second most commonly occurring cyst and not radicular cysts.
Disclosure
The authors declared no conflicts of interest. No funding was received for this study.
references
- Manor E, Kachko L, Puterman MB, Szabo G, Bodner L. Cystic lesions of the jaws - a clinicopathological study of 322 cases and review of the literature. Int J Med Sci 2012;9(1):20-26.
- 2. Oti AA, Donkor P, Owusu-Afriyie O. Orofacial Cysts at Komfo Anokye Teaching Hospital, Ghana. Surgical Science 2013;4:65-67.
- 3. Selvamani M, Donoghue M, Basandi PS. Analysis of 153 cases of odontogenic cysts in a South Indian sample population: a retrospective study over a decade. Braz Oral Res (São Paulo) 2012 Jul-Aug;26(4):330-334.
- 4. Lawal A, Adisa A, Sigbeku O. Cysts of the oro-facial region: A Nigerian experience. J Oral Maxillofac Pathol 2012 May;16(2):167-171.
- 5. Iyogun CA, Ochicha O, Sule AA, Adebola RA. Jaw Cysts in Kano: Northern Nigeria. International Journal of Oral & Maxillofacial Pathology 2013;4(3):08-12.
- 6. Oji CH. Statistical observations on jaw cysts in Enugu, Nigeria, 1987-1996. Odontostomatol Trop 1999;22(85): 33-36.
- 7. Monteiro L, de la Peña J, Fonseca L, Paiva A, do Amaral B. Odontogenic cysts - A descriptive clinicopathological study. Braz J Oral Sci 2005;4(12):670-675.
- 8. de Souza LB, Gordón-Núñez MA, Nonaka CF, de Medeiros MC, Torres TF, Emiliano GB. Odontogenic cysts: demographic profile in a Brazilian population over a 38-year period. Med Oral Patol Oral Cir Bucal 2010 Jul;15(4):e583-e590.
- 9. Meningaud JP, Oprean N, Pitak-Arnnop P, Bertrand JC. Odontogenic cysts: a clinical study of 695 cases. J Oral Sci 2006 Jun;48(2):59-62.
- 10. Tortorici S, Amodio E, Massenti MF, Buzzanca ML, Burruano F, Vitale F. Prevalence and distribution of odontogenic cysts in Sicily: 1986-2005. J Oral Sci 2008 Mar;50(1):15-18.
- 11. Ali MA. Biopsied jaw lesions in Kuwait: a six-year retrospective analysis. Med Princ Pract 2011;20(6):550-555.
- 12. Koseoglu BG, Atalay B, Erdem MA. Odontogenic cysts: a clinical study of 90 cases. J Oral Sci 2004 Dec;46(4):253-257.
- 13. Li TJ. The odontogenic keratocyst: a cyst, or a cystic neoplasm? J Dent Res 2011 Feb;90(2):133-142.
- 14. Yaman Z, Suer BT. Clinical comparison of ultrasonic surgery and conventional surgical techniques for enucleating jaw cysts. Int J Oral Maxillofac Surg 2013 Nov;42(11):1462-1468.
- 15. Nuñez-Urrutia S, Figueiredo R, Gay-Escoda C. Retrospective clinicopathological study of 418 odontogenic cysts. Med Oral Patol Oral Cir Bucal 2010 Sep;15(5):e767-e773.
- 16. Farah CS, Savage NW. Pericoronal radiolucencies and the significance of early detection. Aust Dent J 2002 Sep;47(3):262-265.
- 17. Etti T, Gsau M, Saber R, Reichert TE. Jaw Cysts. Filling or no filling after enucleation? A review. J Craniomaxillofac Surg 2012;40(6):4485-4493.
- 18. Rubio ED, Mombrú CM. Spontaneous Bone Healing after Cysts Enucleation without Bone Grafting Materials: A Randomized Clinical Study. Craniomaxillofac Trauma Reconstr 2015 Mar;8(1):14-22.