Infertility is a global health problem, affecting approximately 17.5% of individuals of reproductive age.1,2 Primary infertility refers to a couple’s inability to conceive despite ≥ 12 months of regular, unprotected sexual intercourse; secondary infertility refers to inability to conceive following at least one previous pregnancy.
Although infertility may arise from male or female factors, its psychosocial burden disproportionately affects women. A systematic review of 32 studies reported significant psychological impact, mainly depression (46.3%), among the affected women.3
Worldwide studies, including a major systematic review by Mascarenhas et al, indicate that primary infertility prevalence in the Middle East and North Africa region exceeds the global average, leading to high psychosocial burden.3–7 Polycystic ovary syndrome (PCOS) additionally affects nearly one in three infertile women in several Gulf Cooperation Council countries.8 In the traditional, collectivist culture of the region, the sociocultural impact of a couple’s inability to conceive often falls on the woman.4–11 Overall infertility rates are increasing in the Middle Eastern countries with multiple factors affecting both genders.3,4,7 For example, smoking has been identified to be a major factor in male infertility in Saudi Arabia.12
Across the Middle East and North Africa region, infertility prevalence, etiology, and sequelae are shaped by interacting biological, environmental, and sociocultural factors.13 Other risk factors for infertility include obesity, consanguinity, vitamin D deficiency, age > 35 years, alcohol consumption, and smoking.7,13,14 Psychosocial stressors such as shame, stigma, and social isolation have been implicated as indirect barriers. Some Omani women with long term infertility expressed concern that they could be divorced.8 Limited availability of infertility treatment and financial burden—such as in parts of Algeria—may also cause stress to couples seeking treatment.9
Ovulation disorders represent the most prominent etiological factor in women, followed by endometriosis, tubal factors, and uterine abnormalities.4 Others include pelvic adhesion, thyroid problems, cancer, chemotherapy, cesarean section, amenorrhea, delayed puberty, obesity, tobacco and alcohol use, genetic abnormalities, and vitamin D deficiency.15 In a study from Nepal, almost half of all infertility cases (48.8%) involved only a female factor, half of which were ovulation related.16 The most reported etiological factors in Eastern Algeria were varicocele in men (28.3% of cases) and ovulation disorders in women (49.1%).7 Different results emerged in a meta-analysis of 41 Iranian studies comprising 35 683 infertility. Here, male factors were higher (43.3%) than female factors (32.0%). The authors also reported that infertility rates in Iran remained the same from 1990 to 2017.4
In Oman, fertility rates have declined sharply over recent decades.17 This demographic trend does not necessarily reflect an increase in infertility. However, several modifiable risk factors of infertility, such as obesity and hypothyroidism, have risen regionally, including in Oman.14 A recent study among Omani women with polycystic ovarian syndrome and infertility also reported major psychological challenges.10 Therefore, our study aimed to investigate the etiology and risk factors of infertility among Omani couples aged 18–49 years.
Methods
Data for this retrospective cross-sectional study were sourced from hospital records of couples who attended the infertility clinic at Sultan Qaboos University Hospital, Muscat, a major national referral center for infertility.
Ethical approval for the study was obtained from the medical research and ethics committee of Sultan Qaboos University (Ref. MREC #2972, April 2023). Using purposive sampling, we collected the data of 259 infertile married Omani couples aged 18–49 years, who were diagnosed with infertility over an eight-year period from 1 January 2015 to 31 December 2022.
Infertility was defined according to World Health Organization criteria as the failure to achieve a clinical pregnancy after 12 months or more of regular, unprotected sexual intercourse. Primary infertility referred to couples who had never achieved a pregnancy, whereas secondary infertility referred to couples who were unable to conceive following at least one previous pregnancy, irrespective of its outcome.18
Data collected included demographic and biometric information and gender-specific risk factors. Female factors included menstrual cycle history, cycle regularity, hormonal evaluation (follicle-stimulating hormone, luteinizing hormone, thyroid function, prolactin, and testosterone), previous surgeries, and uterine, fallopian tube, and ovarian abnormalities. Male factors included semen abnormalities (sperm count, sperm motility, and abnormal forms).
Data were analyzed using SPSS (IBM Corp. Released 2015. IBM SPSS Statistics for Windows, Version 23.0 Armonk, NY: IBM Corp). Mean, SD, and median were calculated for patient age. Body mass index (BMI) was computed from patients' weight and height.
Results
The study included 259 Omani couples (518 individuals) with infertility. Primary infertility was present in 101 (39.0%) couples, and the mean female age in this group was 37.0 ± 7.1 years. Secondary infertility was present in 158 (61.0%) couples, with a mean female age of 43.0 ± 5.5 years. Female factors were identified in 139 (53.7%) couples, male factors in 108 (41.7%) couples, combined male and female factors in 37 (14.3%) couples, and unexplained infertility in 12 (4.6%) couples. A quarter (24.4%) of female partners were overweight and 15.2% were obese [Figure 1]. Sixty-two (23.9%) women reported irregular menstrual cycles [Table 1].
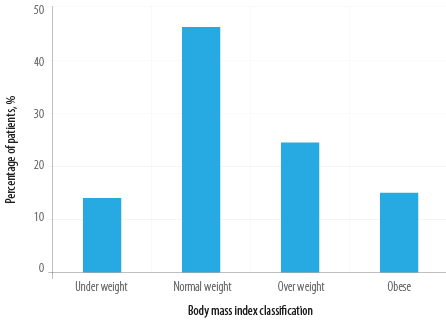 Figure 1: Body mass index distribution in female partners (N = 259).
Figure 1: Body mass index distribution in female partners (N = 259).
Table 1: Demographic and baseline characteristics of infertile Omani couples (N = 259).
|
Couple characteristics
|
|
|
Number of couples
|
259 (100.0)
|
|
Primary infertility
|
101 (39.0)
|
|
Secondary infertility
|
158 (61.0)
|
|
Female partner
|
|
|
Age, mean ± SD, years
|
40 ± 6.3
|
|
Female-factor infertility
|
139 (53.7)
|
|
Irregular menstrual cycles
|
62 (23.9)
|
|
Male partner
|
|
|
Age, mean ± SD, years
|
NA
|
|
Male-factor infertility
|
108 (41.7)
|
|
Combined or unexplained
|
|
|
Combined male and female factors
|
37 (14.3)
|
NA: not available.
Hysterosalpingography revealed that 12 (4.6%) women had bilateral blockage of their fallopian tubes, while 9.3% had one patent tube. Pelvic ultrasound showed that 37/231 (16.0%) women had fibroids, 50 had PCOS, 18 had endometriosis. Out of 51 women with a history of gynecologic surgery, 43.1% underwent ovarian cystectomy, while myomectomy was performed on 27.5% and polypectomy on 29.4% [Table 2].
Table 2: Female partners: clinical investigations and surgical history (n = 259).
|
Hysterosalpingography (n = 259)
|
|
|
Test not indicated
|
133 (51.4)
|
|
Normal
|
90 (34.7)
|
|
One tube blocked
|
24 (9.3)
|
|
Both tubes blocked
|
12 (4.6)
|
|
Pelvic ultrasound (n = 231)
|
|
|
Normal
|
126 (54.5)
|
|
Fibroids
|
37 (16.0)
|
|
Polycystic ovarian syndrome
|
50 (21.6)
|
|
Endometriosis
|
18 (7.8)
|
|
Surgical history (n = 51)
|
|
|
Ovarian cystectomy
|
22 (43.1)
|
|
Myomectomy
|
14 (27.5)
|
The most identified female factors were anovulatory disorders such as PCOS and hyperprolactinemia (63/139; 45.3%), followed by uterine disorders including fibroids, adenomyosis, and congenital uterine anomalies (38; 27.3%), and tubal factors, such as bilateral fallopian tube blockage or a history of salpingectomy, (20; 14.4%). Endometriosis was identified as a cause of infertility in women (7.8%). There was also a positive correlation between prevalence of fibroids and female age (r = 0.211; p < 0.001).
Male infertility factors were present in 41.7% couples. Out of 244/259 (94.2%) men who underwent semen analysis, asthenozoospermia was identified in 20 (18.5%), oligospermia in 49 (45.4%), multiple semen abnormalities in 25 (23.1%), azoospermia in 12 (11.1%) and teratozoospermia in 2 (1.9%) [Table 3].
Table 3: Male partners: clinical investigations and surgical history (n =259).
|
Male partners (total)
|
259 (100)
|
|
Underwent semen analysis
|
244 (94.2)
|
|
Surgical history (n = 259)
|
|
|
Varicocele excision
|
8 (3.2)
|
|
Others
|
13 (5.0)
|
|
Semen analysis results (n = 244)
|
|
|
Abnormal semen parameters
|
108 (44.3)
|
|
Normal semen
|
136 (55.7)
|
|
Types of semen abnormalities (n = 108)
|
|
|
Asthenozoospermia
|
20 (18.5)
|
|
Oligospermia
|
49 (45.4)
|
|
Teratozoospermia
|
2 (1.9)
|
|
Azoospermia
|
12 (11.1)
|
Percentages are calculated using the denominator specified for each section.
Various combinations of both male and female infertility factors were identified in 37 couples. The most prevalent combination of male factors were associated with the following female factors: anovulation (9; 24.3%), tubal factors (3; 8.1%), uterine factors (2; 5.4%), and endometriosis (2; 5.4.%). Sperm motility was < 40.0% in most infertile men.
Further, the majority of women with PCOS were overweight or had obesity [Table 4].
Table 4: Distribution of PCOS cases in women according to BMI (n = 50).
|
Underweight
|
4 (8.0)
|
|
Normal weight
|
16 (32.0)
|
|
Overweight
|
16 (32.0)
|
|
Obese
|
11 (22.0)
|
PCOS: polycystic ovarian syndrome; BMI: body mass index.
Discussion
This study investigated the etiology and risk factors of infertility among Omani couples aged 18–49 years. A major risk factor was advanced age of the female partner, 37.0 and 43.0 years for primary and secondary infertility, respectively. An increasing preference for late marriages in Oman might be a reason.17 In addition, many Omani couples initially seek traditional therapies, leading to late presentations. The threshold for advanced reproductive age lacks a generally agreed-upon definition; yet age ~ 35 years is a widely accepted cutoff in terms of fertility.1 A study among Qatari women reported > 35 years as a significant risk factor, and similar findings have been reported from studies worldwide.1,7,19 A study from Lebanon reported a mean age of 34.8 ± 8 years in infertile women.9
Women who develop obesity early in life are more likely to experience irregular menstruation and infertility.5 In our cohort, 39.6% of infertile women were overweight or obese, highlighting BMI as an important modifiable risk factor. Similar associations between elevated BMI and infertility have been reported elsewhere.20 A Korean study reported that women with BMI ≥ 25.0 kg/m2 had more than twice the odds for infertility than normal weight women.11
Secondary infertility (61.0%) was more common than primary infertility (39.0%) among the couples we studied. A study from the neighboring Qatar showed similar results (68.4% and 31.6%, respectively).1 In contrast, a Bangladeshi study reported 81% of cases were primary infertility.18 This may reflect differences in population characteristics and/or health-seeking behavior between Gulf Cooperation Council and South Asian populations, prompting the need for more international comparative studies.
Ovulation disorders are the leading cause of female infertility, as reported in various studies. The most identified infertility-linked factors in our cohort were anovulatory disorders, particularly PCOS, similar to findings from Lebanon.9 Among the 51 infertile women who underwent various gynecologic surgical procedure, ovarian cystectomy (n =22; 43.1%) was the most common. A large study in the US revealed that women with a history of ovarian cystectomy were more likely to report infertility.19 The authors concluded that both ovarian surgeries to remove cysts and the conditions that lead women to develop cysts requiring surgery may affect subsequent successful conception.19
Our study found 45.3% of infertile women having an anovulation problem. A Bangladeshi study reported comparable findings among infertile women: ovulation failure (60%), polycystic ovarian disease (32%), bilateral tubal blockage (8%), and pelvic adhesions (24%).21 A previous retrospective study among infertile Omani women reported congenital uterine anomaly and tubal block.22
Endometriosis is a common condition affecting 5–10% of women of reproductive age globally, with correlation with infertility.23 The prevalence of endometriosis in our study was 7.8% among 231 women who underwent ultrasound. If only female factors (n = 139) are taken into account this proportion will increase to 12.9%. Even then, it remained lower than the commonly reported infertility rate of 30–50% among women with endometriosis.24
The second most common cause of female infertility identified in our study was uterine conditions (27.3%) including fibroids and adenomyosis. Tubal factors that included the blockage of both fallopian tubes and a history of salpingectomy were present in 20 infertile women.
Unexplained infertility is a diagnosis of exclusion that is made only after assessing both partners. In this cohort, 4.6% couples had unexplained infertility, which is much lower than the rates reported from other developing countries (19–34%), possibly because of differences in diagnostic technology.15,25
To assess male infertility, we studied semen parameters. Among 108 (44.3%) men with semen abnormalities the most prevalent were, oligospermia (45.4%) asthenozoospermia (18.5%) and multiple semen abnormalizes (23.1%). This ‘abnormality mix’ differed from those elsewhere in the world. In a Nepali cohort, the leading causes of male infertility were oligospermia (55%) and asthenozoospermia (45%).26 In Iran, azoospermia (56.4%) and oligospermia (24.5%) were the predominant abnormalities.13 These differences might be due to methodological differences between studies, including different cutoff values. Our study followed World Health Organization laboratory manual for semen analysis: for example, a sperm sample was labelled as asthenozoospermia if the motile sperms were ≤ 42%.27 Another possibility is ethnogeographic variations in sperm abnormality types between different populations.
The findings strongly indicate the need for early detection, treatment, and accessibility to affordable infertility treatment facilities. Enhanced community-based awareness programs are recommended to prevent infertility related modifiable risk factors. Similar recommendations have been made elsewhere, including in a Lebanese study. 9
This study has limitations, mainly due to its retrospective design. For example, data regarding certain modifiable risk factors such as smoking, other lifestyle-related factors, including BMI of male partners and occupation of some couples were not available. We were also unable to collect data on patients’ quality of life, barriers to seeking fertility treatment, stigma and attitudes around infertility, or the social, cultural, and religious issues related to infertility, despite the high impact of psychosocial barriers in traditional collective cultures, as a recent pan-African scoping review.28
Future studies should include multiregional data from both the public and private sectors and capture variables that are often unavailable in retrospective studies such as ours, to improve comprehensiveness and generalizability. Data from both women and men should be equally detailed. A major challenge for patients in Oman is the logistical difficulty of accessing treatment. Although infertility diagnosis and treatment are provided free of charge, facilities comparable to our center are not widely available across the country, placing a substantial burden on couples living in remote areas. We therefore recommend expanding access by establishing advanced infertility clinics throughout Oman.
Conclusion
This study identified the major etiologies and risk factors associated with infertility among Omani couples. Advanced female age was a major risk factor, and anovulatory disorders were the leading female causes of infertility. In addition, the significant association between increasing female BMI and PCOS highlights an important modifiable and treatable risk factor. Addressing these factors and improving awareness of modifiable risks may help reduce infertility in Oman.
Acknowledgements
The authors are grateful to the hospital information center and the statistical departmental staff who helped in tracing medical records of participants.
Disclosure
The authors declare no conflicts of interest. No funding was received for this study.
references
- 1. Musa S, Osman S. Risk profile of Qatari women treated for infertility in a tertiary hospital: a case-control study. Fertil Res Pract 2020 Jul;6:12.
- 2. Ibitoye BO, Fasasi OA, Ibitoye FO, Akadiri O. WHO fact sheet on infertility (definition of infertility), published in global reproductive health (2021). Glob Reprod Health 2023;8:e60.
- 3. Nik Hazlina NH, Norhayati MN, Shaiful Bahari I, Nik Muhammad Arif NA. Worldwide prevalence, risk factors and psychological impact of infertility among women: a systematic review and meta-analysis. BMJ Open 2022 Mar;12(3):e057132.
- 4. Abangah GH, Rashidian T, Parizad Nasirkandy M, Azami M. A meta-analysis of the prevalence and etiology of infertility in Iran. Int J Fertil Steril 2023 Apr;17(3):160-173.
- 5. Mascarenhas MN, Flaxman SR, Boerma T, Vanderpoel S, Stevens GA. National, regional, and global trends in infertility prevalence since 1990: a systematic analysis of 277 health surveys. PLoS Med 2012;9:e1001356.
- 6. Fatima W, Akhtar AM, Hanif A, Gilani A, Farooq SM. Predicted risk factors associated with secondary infertility in women: univariate and multivariate logistic regression analyses. Front Med (Lausanne) 2024 Mar;10:1327568.
- 7. Harbouche A, Debbache A, Zoghmar A, Rouabah A-E, Benmerzoug M, Benbouhedja S, et al. Risk factors and etiology linked to infertility in a sample of Eastern Algerian couples. SAJEB 2021;11(4):458-465.
- 8. Al-Rifai R. Polycystic ovary syndrome in infertile women in Gulf cooperation council countries: a meta-analysis. European Journal of Public Health 2025;35.
- 9. Dia N, Mansour S, Kharaba Z, Malaeb B, Sarray El Dine A, Kokash S, et al. Factors associated with infertility among the Lebanese population: a cross-sectional study. Int J Environ Health Res 2024 Feb;34(2):934-942.
- 10. ALSumri H, Szatkowski L, Gibson J, Fiaschi L, Bains M. Psychosocial impacts of infertility among Omani women with polycystic ovarian syndrome: a qualitative study. Int J Fertil Steril 2023 Feb;17(2):107-114.
- 11. Lee J, Choo C-W, Moon KY, Lyu SW, Kim H, Lee JY, et al. Risk factors for infertility in Korean women. J Korean Med Sci 2024 Mar;39(10):e85.
- 12. Qutub J, Sharee M, Murad BA, Alsadiq A, Dakhil SA, Alofi N. Smoking and infertility in Saudi Arabian males: a systematic review. JOHS 2022;2(11):469-477.
- 13. Lawrenz B, Coughlan C, Melado L, Fatemi HM. Ethnical and sociocultural differences causing infertility are poorly understood--insights from the Arabian perspective. J Assist Reprod Genet 2019 Apr;36(4):661-665.
- 14. Moridi A, Yaghoobi H, Shahrahmani N, Dashti S, Soltani S, Banaei M, et al. Etiology and risk factors associated with infertility. Int J Women’s Health Reprod Sci 2019;7:346-353.
- 15. Deshpande PS, Gupta AS. Causes and prevalence of factors causing infertility in a public health facility. J Hum Reprod Sci 2019;12(4):287-293.
- 16. Tamrakar SR, Bastakoti R. Determinants of infertility in couples. J Nepal Health Res Counc 2019 Apr;17(1):85-89.
- 17. Islam MM. Rapid fertility decline in Oman: understanding the role of proximate determinants. Middle East Fertil Soc J 2017;22:275-284.
- World Health Organization. Infertility. Geneva; 2025 [cited 2026 Feb 22]. Available from: https://www.who.int/news-room/fact-sheets/detail/infertility.
- 19. Shandley LM, Spencer JB, Kipling LM, Hussain B, Mertens AC, Howards PP. The risk of infertility after surgery for benign ovarian cysts. J Womens Health (Larchmt) 2023 May;32(5):574-582.
- 20. Vitale SG, La Rosa VL, Petrosino B, Rodolico A, Mineo L, Laganà AS. The impact of lifestyle, diet, and psychological stress on female fertility. Oman Med J 2017 Sep;32(5):443-444.
- 21. Sultana A, Keya KA, Adhikary S, Akhter S, Tanira S. Explained infertility among the couple attending the infertility unit of Bangabandhu Sheikh Mujib Medical University (BSMMU), Bangladesh. J Dhaka Med Coll 2015;23:114-120.
- 22. Albalushi H, Ba-Alawi A, Aljabri R, Al Khaduri M. Prevalence of congenital uterine anomalies and tubal blockage in infertile Omani women: a retrospective study. Oman Med J 2023 Jan;38(1):e463.
- 23. Taylor HS, Kotlyar AM, Flores VA. Endometriosis is a chronic systemic disease: clinical challenges and novel innovations. Lancet 2021 Feb;397(10276):839-852.
- 24. Leone Roberti Maggiore U, Chiappa V, Ceccaroni M, Roviglione G, Savelli L, Ferrero S, et al. Epidemiology of infertility in women with endometriosis. Best Pract Res Clin Obstet Gynaecol 2024 Feb;92:102454.
- 25. Magdum M, Chowdhury MA, Begum N, Riya S. Types of infertility and its risk factors among infertile women: a prospective study in Dhaka city. JBM 2022;10:158-168.
- 26. Pokhrel S, Ghimire A, Chhetry M, Lamichane S, Shreewastav RK. Selected risk factors and pattern of semen abnormality in male partners of infertile couples in eastern nepal: a descriptive cross-sectional study. JNMA J Nepal Med Assoc 2020 Sep;58(229):668-671.
- 27. Chung E, Atmoko W, Saleh R, Shah R, Agarwal A. Sixth edition of the World Health Organization laboratory manual of semen analysis: updates and essential take away for busy clinicians. Arab Journal of Urology 2024;22(2):71-74.
- 28. Roomaney R, Salie M, Jenkins D, Eder C, Mutumba-Nakalembe MJ, Volks C, et al. A scoping review of the psychosocial aspects of infertility in African countries. Reprod Health 2024 Aug;21(1):123.