Calcifying fibrous tumor (CFT) is a rare benign tumor of mesenchymal origin which has been documented in different anatomical sites, including the gastrointestinal tract and a variety of superficial and deep soft tissues, such as the pleura.1 CFTs of the GI tract usually remain asymptomatic and are incidentally discovered, or may present with symptoms, such as abdominal pain, dyspepsia, nausea, or vomiting.2 Complications can arise in the presence of gastric ulcers, bowel obstruction, volvulus, or intussusception.2
Treatment is usually by surgical resection or endoscopic submucosal dissection.3 CFT of the GI tract has no tendency for local recurrence, unlike soft tissue CFT.4 There are no reported cases of malignant transformation of CFT.2
Case Report
A 33-year-old man with no significant medical history presented to our emergency department with pain in the right iliac fossa associated with nausea and vomiting for one day, after consuming food from outside. He did not report diarrhea or respiratory or urinary symptoms.
On examination, the patient was alert, conscious, and vitally stable with clear chest and right iliac fossa tenderness. His complete blood count result was unremarkable, while C-reactive protein was elevated at 54 mg/L. Abdominal X-ray revealed a dilated small intestine. Bowel gases prevented ultrasound visualization of the appendix. Therefore, computed tomography (CT) scan of the abdomen using intravenous contrast was performed. The scan, conducted during the portal venous phase, revealed distended small bowel loops and a dilated appendix. This raised suspicion of appendicitis, accompanied by irritation or obstruction of the small bowel as a secondary effect. He was referred to general surgery with an impression of appendicitis, the other differential diagnosis being gastroenteritis.
A nasogastric tube was inserted to relieve the obstruction but still there was increasing abdominal distension and guarding. The surgical team opted for diagnostic laparoscopy. During the laparoscopic probing, the appendix appeared normal, but a mesenteric mass was identified and laparotomy was decided upon. During laparotomy, a band was revealed. It was constricting the small bowel and was connected to both the omentum and a mesenteric jejunal mass. This mass did not obstruct the lumen of the jejunal loop but was firmly attached to the mesentery [Figure 1]. The mass was excised completely, and the band was released and ligated.
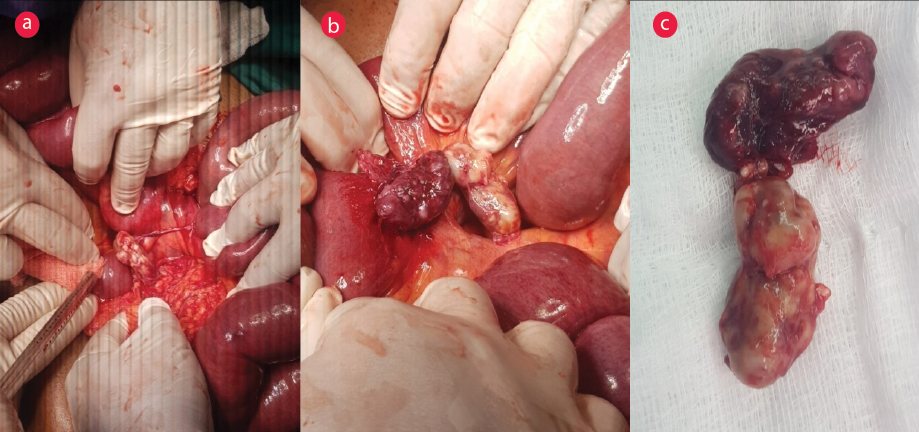 Figure 1: (a) and (b): Intraoperative views of the mesenteric calcifying fibrous tumor and dilated small bowel loops. (c)The excised tumor.
Figure 1: (a) and (b): Intraoperative views of the mesenteric calcifying fibrous tumor and dilated small bowel loops. (c)The excised tumor.
With hindsight from the surgery, the original CT images were once again examined. The mass could be detected in the small bowel mesentery, with the appearance of a small bowel loop (which was why it was not identified earlier, especially as no bowel contrast was used). The marginal foci of calcifications were also identified [Figure 2].
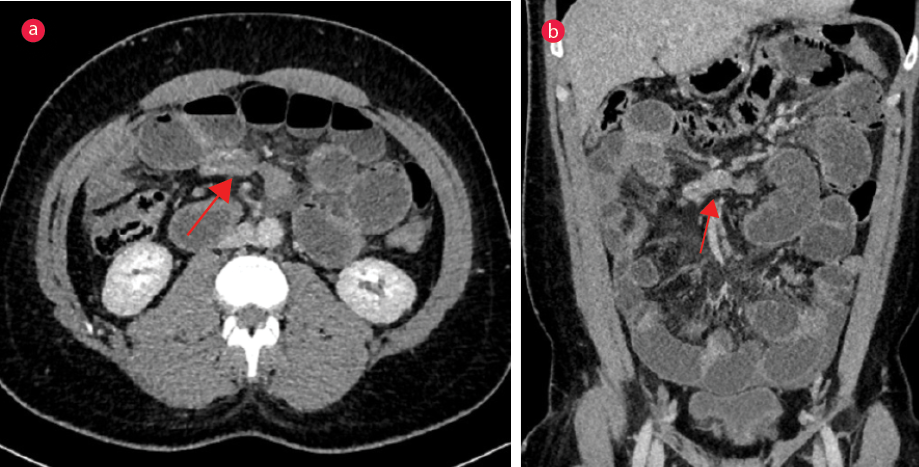 Figure 2:(a) Axial CT image showing the mesenteric calcifying fibrous tumor (arrow). (b) Coronal CT image showing dilated fluid-filled small bowel loops.
Figure 2:(a) Axial CT image showing the mesenteric calcifying fibrous tumor (arrow). (b) Coronal CT image showing dilated fluid-filled small bowel loops.
Sections from the excised mass [Figure 3] showed a paucicellular fibroblastic proliferation with bland spindle cells embedded in dense collagenous stroma with scattered calcifications and foci of lymphoplasmacytic infiltrate. There was no evidence of malignancy. The final diagnosis was a calcifying mesenteric tumor.
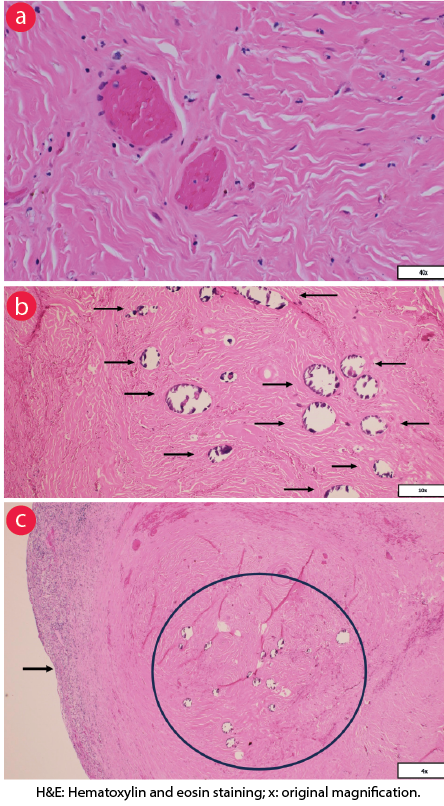 Figure 3: Histopathology sections of the excised mesenteric mass in different magnifications show a well-circumscribed hypocellular lesion composed of scattered bland cells embedded in highly collagenized stroma with dystrophic calcification. There are scattered chronic inflammatory cells. No indication of atypia or malignancy. (a) The microscopic field shows collagenized fibrotic stroma and two adjacent blood vessels (hematoxylin and eosin(H&E) staining, magnification = 40×). (b) Scattered spheres of dystrophic classification (Black arrows) embedded within a sclerosed fibrotic stroma, with only the rim of the calcified materials remaining in the slide due to detachment during tissue processing (H&E staining, magnification = 10×). (C) A circumscribed mass composed of fibrotic sclerosed stroma with embedded multiple dystrophic calcification spheres (black circle). At the periphery, a rim of inflammatory cells is noted (black arrow) (H&E staining, magnification = 4×).
Figure 3: Histopathology sections of the excised mesenteric mass in different magnifications show a well-circumscribed hypocellular lesion composed of scattered bland cells embedded in highly collagenized stroma with dystrophic calcification. There are scattered chronic inflammatory cells. No indication of atypia or malignancy. (a) The microscopic field shows collagenized fibrotic stroma and two adjacent blood vessels (hematoxylin and eosin(H&E) staining, magnification = 40×). (b) Scattered spheres of dystrophic classification (Black arrows) embedded within a sclerosed fibrotic stroma, with only the rim of the calcified materials remaining in the slide due to detachment during tissue processing (H&E staining, magnification = 10×). (C) A circumscribed mass composed of fibrotic sclerosed stroma with embedded multiple dystrophic calcification spheres (black circle). At the periphery, a rim of inflammatory cells is noted (black arrow) (H&E staining, magnification = 4×).
Postoperatively the patient remained stable with a clean dressing and soft abdomen; he tolerated an oral diet and passed motion, and was discharged uneventfully. Consent for publication was taken from the patient.
Discussion
CFT was first reported in 1988 in two pediatric cases, which featured soft tissue fibrous tumor with psammoma bodies.5 At first it was described as ‘pseudotumor of possible inflammatory or traumatic etiology,’ which was later changed to the current name CFT as was noted cases of local recurrence.6 Chorti et al.’s1 international review of 104 papers comprising 157 CFT cases estimated the frequency of abdominal CFT as rare, with just one case yearly with a trimodal age distribution—one peak at 0–4 years of age, another peak in the mid-20s, and a third peak in the mid-30s (as in our patient)—with indications that the third peak may be associated with late sclerosing stage of this myofibroblastic tumor.
What was unique in our case was the association of mesenteric CFT with a mesenteric band that constricted the small intestine, leading to its obstruction. Congenital bands are a rare cause of intestinal obstruction in children, and extremely rare in adults. A patient may present with obstruction despite no history of trauma or surgery.7 Our patient too had no previous trauma or surgery, and no hernia was revealed in examination or imaging.
Microscopically, these lesions are characteristically hypocellular with abundant hyalinized collagen and are composed of bland cells with ovoid vesicular nuclei and eosinophilic cytoplasm. Lymphoplasmacytic infiltrates are a consistent finding, while psammomatous or dystrophic calcifications are common,8 also found in our patient’s histopathology result.
Conclusion
CFT of the GI tract is rare and can present with different symptoms depending on its size and location. It can be associated with other pathologies such as congenital bands—as in the present case—which should be suspected in a patient presenting with small bowel obstruction without previous history of trauma or surgery and with no detectable hernias. Management is by surgical resection, which is usually curative.
Disclosure
The authors declare no conflicts of interest.
References
- 1. Chorti A, Papavramidis TS, Michalopoulos A. Calcifying fibrous tumor: review of 157 patients reported in international literature.Medicine (Baltimore)2016 May;95(20):e3690.
- 2. Turbiville D, Zhang X. Calcifying fibrous tumor of the gastrointestinal tract: a clinicopathologic review and update.World J Gastroenterol2020 Oct;26(37):5597-5605.
- 3. Ogasawara N, Izawa S, Mizuno M, Tanabe A, Ozeki T, Noda H, et al. Gastric calcifying fibrous tumor removed by endoscopic submucosal dissection.World J GastrointestEndosc2013 Sep;5(9):457-460.
- 4. George SA, Abdeen S. Gastric calcifying fibrous tumor resembling gastrointestinal stromal tumor: a case report.Iran J Pathol2015;10(4):306-309.
- 5. Rosenthal NS, Abdul-Karim FW. Childhood fibrous tumor with psammoma bodies. Clinicopathologic features in two cases.Arch Pathol Lab Med1988 Aug;112(8):798-800.
- 6. Nascimento AF, Ruiz R, Hornick JL, Fletcher CD. Calcifying fibrous ‘pseudotumor’: clinicopathologic study of 15 cases and analysis of its relationship to inflammatory myofibroblastic tumor.Int J Surg Pathol2002 Jul;10(3):189-196.
- 7. Dimitrios C, George AA, Dimosthenis Z, Nikolaos X. Intestinal obstruction due to an anomalous congenital band.Saudi J Gastroenterol2008 Jan;14(1):36-37.
- 8. Pezhouh MK, Rezaei MK, Shabihkhani M, Ghosh A, Belchis D, Montgomery EA, et al. Clinicopathologic study of calcifying fibrous tumor of the gastrointestinal tract: a case series.Hum Pathol2017Apr;62:199-205.