Ovarian hyperstimulation syndrome (OHSS) is a complication of assisted reproduction technology (ART). It results from an exaggerated ovulation process in response to exogenous gonadotropins. This exaggeration manifests in excessive production of corpora lutea, causing a massive fluid shift from intravascular to the third space compartment, leading to intravascular hypovolemia, overt with clinical fluid overload, resulting in severe cardiac, renal, and liver impairment, which can be fatal.1 Spontaneous ovarian hyper-stimulation syndrome (sOHSS), although rare, has been reported in association with multiple pregnancy, hypothyroidism and polycystic ovarian syndrome (PCOS). The pathogenesis is not fully understood, but two main theories have been suggested: hypersecretion of glycoprotein hormone and genetic mutation of the follicle-stimulating hormone (FSH) receptor.2 Clinical manifestations include enlarged ovaries with multiple follicular cysts, manifesting in abdominal discomfort, and pain with increased vascular permeability, leading to fluid accumulation in dependent areas, resulting in ascites, pedal and pulmonary edema and pleural effusion.3 The diagnosis is dependent on clinical assessment aided by imaging. The history of exogenous gonadotropin administration is crucial to make a conclusive diagnosis of OHSS.3 This paper reports a peculiar case of sOHSS in a young non-pregnant woman, which was managed by multidisciplinary teams in two tertiary institutes in Muscat (the Royal Hospital and Khoula Hospital) who focused on the imaging findings at each follow-up.
Case Report
A 28-year-old non-pregnant obese woman with no history of ART presented with a six-month history of headaches, visual disturbances, galactorrhea, and secondary amenorrhea. Her medical background included obesity and PCOS. Clinical examination revealed a soft, non-distended abdomen. Neurological examination revealed right lower quadrant hemianopia.
Test for human chorionic gonadotropin (hCG) yielded a negative result (< 5.3 IU/L) as expected for non-pregnant women. Hormonal tests showed normal levels of thyroid hormones and FSH, elevated prolactin (405 IU/L) and estradiol (1095 pg/mL), and low luteinizing hormone (0.5 IU/L). Other routine test results were unremarkable.
Abdominal imaging with ultrasound and magnetic resonance imaging (MRI) of the pelvis revealed both ovaries as hugely enlarged (right 48 mL; left 28 mL) and containing multiple different-sized follicular cysts. The MRI also showed hypertrophied central stroma bilaterally with features suggestive of OHSS [Figure 1]. Concordant brain MRI [Figure 1] revealed a 1.3 × 1.1 × 1.0 cm lesion occupying the pituitary gland fossa with progressive enhancement on dynamic contrast study. A diagnosis of pituitary macroadenoma was made.
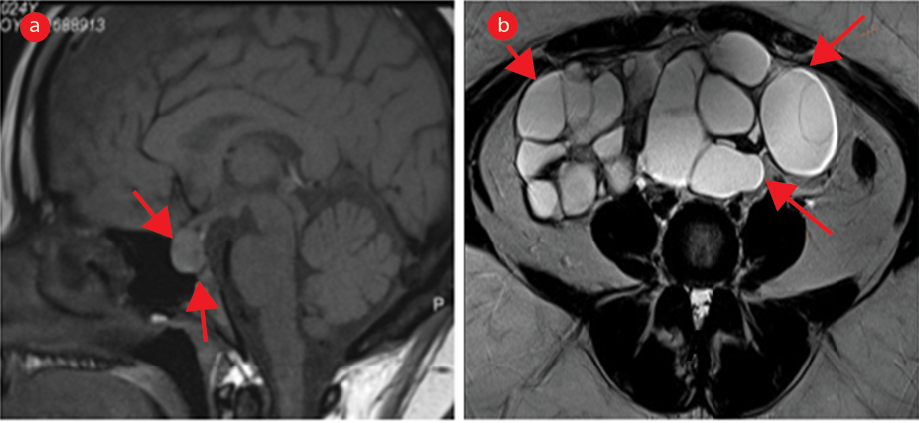 Figure 1: MRI of the brain and pelvis at presentation. (a) Initial MRI sagittal pituitary T1-weighted-image shows a 1.3 cm lesion indicative of pituitary macroadenoma (arrows). (b) Serial pelvis MRI on axial plane T2-weighted-image shows greatly enlarged ovaries with stromal hypertrophy (arrows).
Figure 1: MRI of the brain and pelvis at presentation. (a) Initial MRI sagittal pituitary T1-weighted-image shows a 1.3 cm lesion indicative of pituitary macroadenoma (arrows). (b) Serial pelvis MRI on axial plane T2-weighted-image shows greatly enlarged ovaries with stromal hypertrophy (arrows).
Initial management with a dopamine agonist resulted in minimal improvement only. Therefore, she underwent transsphenoidal resection of the pituitary macroadenoma. Four months after the pituitary surgery, there was clinical improvement in the patient’s symptoms. However, a follow-up MRI of the brain [Figure 2] revealed a residual lesion measuring 1 × 0.7 × 0.6 cm. MRI of the pelvis [Figure 2] showed that the ovarian hyperstimulation features were resolved.
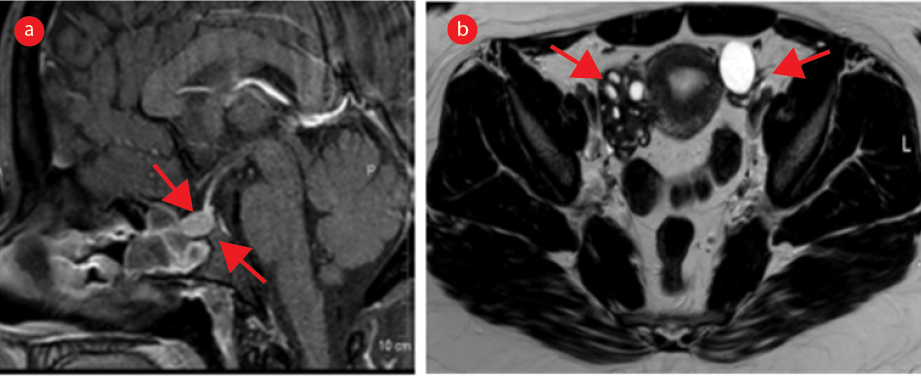 Figure 2: MRI of the brain and pelvis four months after pituitary macroadenoma resection. (a) Sagittal pituitary T1-weighted MRI shows a residual lesion measuring nearly 1.0 cm (arrows). (b) Serial pelvic axial T2-weighted MRI shows both the ovaries with normal appearance and size (arrows).
Figure 2: MRI of the brain and pelvis four months after pituitary macroadenoma resection. (a) Sagittal pituitary T1-weighted MRI shows a residual lesion measuring nearly 1.0 cm (arrows). (b) Serial pelvic axial T2-weighted MRI shows both the ovaries with normal appearance and size (arrows).
Four years later, our patient’s symptoms recurred. The new laboratory findings were similar to the baseline findings, including negative results for hCG and thyroid screening, extremely elevated prolactin (21 364 IU/L), normal FSH (6.2 IU/L), and suppressed luteinizing hormone (0.5 IU/L). MRI of the brain [Figure 3] showed an interval increase in the size of the pituitary macroadenoma measuring 1.4 × 1.2 × 1.2 cm. Pelvis MRI [Figure 3] showed recurrence of bilateral ovarian hyper-stimulation features. Due to persistent symptoms, the patient underwent a repeat surgery for the pituitary adenoma.
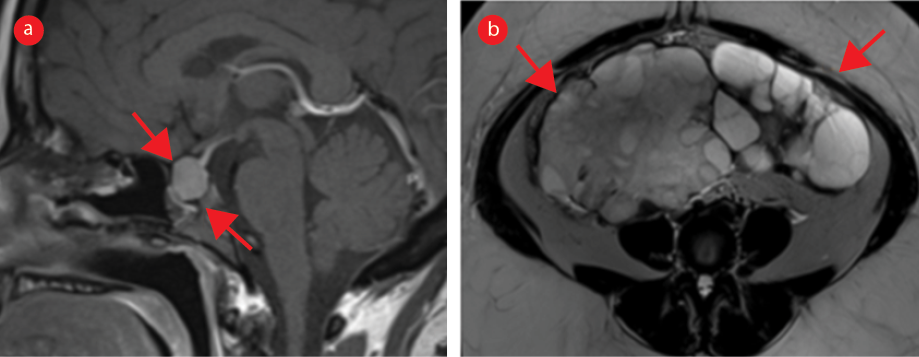 Figure 3: MRI four years after pituitary macroadenoma resection. (a) Brain MRI shows pituitary macroadenoma measuring approximately 1.4 cm (c.f. Figures 1a and 2a). (b) Serial pelvic MRI on axial plane T2-weighted image shows marked enlargement of both the ovaries (arrows) with multiple follicles and prominent stroma (c.f. Figures 1b and 2b).
Figure 3: MRI four years after pituitary macroadenoma resection. (a) Brain MRI shows pituitary macroadenoma measuring approximately 1.4 cm (c.f. Figures 1a and 2a). (b) Serial pelvic MRI on axial plane T2-weighted image shows marked enlargement of both the ovaries (arrows) with multiple follicles and prominent stroma (c.f. Figures 1b and 2b).
Written consent was taken from the patient.
Discussion
Presentations of sOHSS are typically associated with high hCG levels, a characteristic feature of pregnancy. The combination of sOHSS and elevated hCG leads to abnormally high neovascularization, causing fluid shift to the extravascular compartments.1,2 Our patient, however, was not pregnant since the onset of her symptoms, and had consistently low hCG levels (< 1) during her three presentations over four years. Instead, she had an FSH-secreting pituitary macroadenoma, which was considered the cause of sOHSS in her case. However, her FSH levels were within the normal range at each analysis. The clinical manifestations of sOHSS include abdominal pain and distension and ascites, which were absent in our patient.1,3 Rather, she presented with headaches, nausea, amenorrhoea, and visual disturbances, with a background of a history of PCOS.
Radiological investigations using ultrasound, computed tomography, and MRI usually yield similar findings in sOHSS cases. These typically include symmetrically enlarged ovaries, usually > 20 mL in volume, and multiple non-uniform cysts, creating a ‘spoke-wheel’ appearance, in addition to associated free fluid in the abdomen. Our patient had symmetrical enlargement of her ovaries, with multilobulated cysts of varying sizes, with the characteristic spoke-wheel appearance.4,5
A few similar cases of FSH-secreting macroadenomas causing sOHSS in non-pregnant women with normal thyroid function have been reported.6–8 Their authors have suggested surgical resection of the macroadenoma as the standard treatment of choice. Other reported suggestions include radiotherapy and medical therapy with dopamine agonists and somatostatin analogues, though these are case-dependent.1,2,8 Though the patient initially underwent medical treatment with a dopamine agonist (cabergoline), she did not respond well, which led to surgical excision of the pituitary macroadenoma.
Conclusion
We reported a rare association of sOHSS secondary to FSH-secreting pituitary macroadenoma in a young non-pregnant woman with no history of ART or thyroid disease. Of particular interest are three serial pelvic and pituitary MRI scans taken at baseline, four months after the first surgical resection of the pituitary macroadenoma and four years later, when recurrence of the pituitary macroadenoma and sOHSS was identified.
Disclosure
The authors declare no conflicts of interest.
References
- 1. Namavar Jahromi B, Parsanezhad ME, Shomali Z, Bakhshai P, Alborzi M, Moin Vaziri N, et al. Ovarian hyperstimulation syndrome: a narrative review of its pathophysiology, risk factors, prevention, classification, and management. Iran J Med Sci 2018 May;43(3):248-260.
- 2. Delbaere A, Smits G, Olatunbosun O, Pierson R, Vassart G, Costagliola S. New insights into the pathophysiology of ovarian hyperstimulation syndrome. What makes the difference between spontaneous and iatrogenic syndrome? Hum Reprod 2004 Mar;19(3):486-489.
- 3. Kumar P, Sait SF, Sharma A, Kumar M. Ovarian hyperstimulation syndrome. J Hum Reprod Sci 2011 May;4(2):70-75.
- 4. Mittal K, Koticha R, Dey AK, Anandpara K, Agrawal R, Sarvothaman MP, et al. Radiological illustration of spontaneous ovarian hyperstimulation syndrome. Pol J Radiol 2015 Apr 28;80:217-227.
- 5. Bhutani R, Arora A, Kapoor V, Pant CS. Assisted reproductive technology – boon or bane? ERC 2023 [cited 2023 June]. Available from: https://epos.myesr.org/poster/esr/ecr2013/C-2509/imaging%20findings%20or%20procedure.
- 6. Cooper O, Geller JL, Melmed S. Ovarian hyperstimulation syndrome caused by an FSH-secreting pituitary adenoma. Nat Clin Pract Endocrinol Metab 2008 Apr;4(4):234-238.
- 7. Caretto A, Lanzi R, Piani C, Molgora M, Mortini P, Losa M. Ovarian hyperstimulation syndrome due to follicle-stimulating hormone-secreting pituitary adenomas. Pituitary 2017 Oct;20(5):553-560.
- 8. Hasegawa H, Nesvick CL, Erickson D, Cohen SC, Yolcu YU, Khan Z, et al. Gonadotroph pituitary adenoma causing treatable infertility and ovarian hyperstimulation syndrome in female patients: neurosurgical, endocrinologic, gynecologic, and reproductive outcomes. World Neurosurg 2021 Jun;150:e162-e175.