Inflammatory bowel disease (IBD) encompasses a group of chronic inflammatory conditions affecting the gastrointestinal (GI) tract. The two main forms are Crohn’s disease (CD) and ulcerative colitis (UC). IBD has become a worldwide health issue with a rising incidence. A 2021 study on the epidemiology of IBD in the Arab world estimated the annual incidence rate of UC as ~ 2.33/100 000 and that of CD as ~ 1.46/100 000 in the general population.1
While the exact cause of IBD remains unclear, it is widely attributed to a complex interplay between the host genetics, the gut microbiome, and the immune system, which triggers a strong inflammatory response within the lamina propria, manifested as excessive production of mucus, alpha-defensins, and antimicrobial peptides.2
Presentation may vary depending on the IBD type (CD or UC), genetic background, site of involvement, and lifestyle factors. The most common symptoms include bloody diarrhea, tenesmus, nausea, vomiting, abdominal pain, and weight loss.2 Additionally, patients with IBD are at higher risk for serious infections, mainly due to impaired innate immune response, immunosuppressive medications, and malnutrition.3,4
Hepatitis B virus (HBV) is a blood-borne hepatotropic virus that is preventable by vaccination, which led the World Health Organization (WHO) to urge its eradication through active treatment and vaccination. Patients with IBD are more prone to developing and reactivating HBV infection.5 In 1990, HBV vaccination was included among scheduled immunization schedule in Oman.6 The humoral immune response to HBV vaccine is > 90% in healthy individuals, but much lower in patients with IBD. Recommendations to improve the vaccine immunogenicity in individuals with impaired immunity include booster doses and different vaccine schedules.7
Multiple studies have shown that patients with IBD are at a risk for contracting HBV because of their impaired immunity, failed HBV vaccination, and frequent exposure to blood transfusions as well as surgical and endoscopic procedures.8 Thus, long-term immunity against HBV is a significant clinical concern for these patients, as their already impaired immunity, compounded by immunosuppressive therapies and nosocomial infections, reduces the effectiveness of HBV vaccination.
Reduced vaccine response in IBD arises from impaired immunity, which fails to generate adequate antibody titers.7 Several reports recommend HBV vaccine booster doses to achieve protective antibody levels, especially for older individuals. Patients with IBD require routine HBV serological screening, especially before immunosuppression therapy. Vaccination timing is crucial, and should ideally coincide with IBD diagnosis or disease remission to maximize effectiveness.7
This study quantified the long-term immunogenicity of the scheduled HBV vaccine in patients with IBD in Oman compared to healthy controls.
Methods
This retrospective hospital-based case-control study was conducted from 1 January to 31 May 2024, among patients with IBD at Sultan Qaboos University Hospital (SQUH), Muscat. Ethical approval was obtained from the Medical Research Ethics Committee at the College of Medicine and Health Sciences, Sultan Qaboos University (Ref. MREC #30523 dated 1 January 2024).
The study population consisted of two groups: a case group and a control group, both comprising Omani nationals. All patients < 32 years of age who were diagnosed with IBD at SQUH were included. This age limit was chosen to include only individuals born after 1981, coinciding with the implementation of compulsory HBV vaccination in Oman.
An age- and sex-matched control group was concurrently recruited from among healthy Omani organ and blood donors at SQUH. Inclusion criteria for the case group included a documented history and diagnosis of IBD, as well as recent HBV screening within the preceding five years. The control group was required to have documented HBV screening and confirmed prior HBV vaccination. Exclusion criteria for both groups were undocumented vaccination history of complete three-dose HBV series and/or evidence of acquired or inherited immunosuppression.
A sample size of 126 was estimated following Cossio-Gil et al,9 using the formula n = NZ2 p (1-p) / {d2 (N-1) + Z2p (1-p)}, where n = sample size, N = total number of IBD patients at SQUH, d = permissible error of 10%, Z = standard normal deviation = 1.96 at 95% confidence level (95% CI) and p = proportion of IBD patients with immunogenicity against HBV.
Demographic and clinical data were collected from the electronic medical records of SQUH. The following variables were collected: age, sex, type of IBD (CD or UC), medication data (immunosuppressants, biologics, antibiotics), anthropomorphic measurements (height, weight, body mass index (BMI)), and laboratory results (HBV and HIV screening tests, serum iron, ferritin, hemoglobin, serum albumin, glycated hemoglobin). The optimal immune response of both groups against the HBV vaccine was defined as an anti-HBs concentration ≥ 10 mIU/mL.10
The collected data were analyzed using IBM SPSS Statistics for Windows (IBM Corp. Released 2017. IBM SPSS Statistics for Windows, Version 25.0. Armonk, NY: IBM Corp.). Descriptive statistics were generated, and chi-square test was used to examine the association between the variables and the level of anti-HBs antibodies. A p-value of < 0.05 was considered significant.
Results
The patient group comprised 126 individuals with IBD who underwent HBV serological screening and met our inclusion criteria. Their mean age was 22.3 ± 6.2 years, with near-equal sex distribution. The control group included 126 healthy Omani blood/organ donors with a male majority (73.0%) and a mean age of 27.7 years [Table 1].
Within the IBD group, 29 (23.0%) patients were seropositive for anti-HBs, indicating current immunity. Only two (1.6%) patients tested positive for anti-HBc, suggestive of prior HBV exposure without current immunity. Importantly, none of the IBD patients exhibited positivity for HBsAg, signifying an absence of ongoing viral
replication [Table 1].
In contrast, 109 (86.5%) controls were seropositive for anti-HBs, indicative of protective immunity. Five (4.0%) patients tested positive for HBsAg, signifying ongoing viral replication [Table 1]. These HBsAg-positive patients were three (60.0%) males and two (40.0%) females.
Most patients with IBD (82.5%) had CD, while 22 (17.5%) had UC. Comorbidities were present in 65.1% patients, mainly iron deficiency anemia (80; 63.5%), hypoalbuminemia (8; 6.3%), and type 2 diabetes (2; 1.6%) [Figure 1]. Regarding the BMI distribution, 64 (50.8%) patients were normal weight, 36 (28.6%) were underweight, 14 (11.1%) were overweight, and 12 (9.5%) were obese [Table 1].
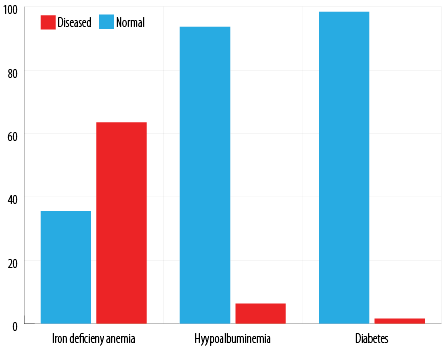 Figure 1: Comorbidities among Omani patients with inflammatory bowel disease (n = 126).
Figure 1: Comorbidities among Omani patients with inflammatory bowel disease (n = 126).
Table 1: Baseline characteristics of Omani patients with IBD (n = 126) versus control group (n =126).
|
Age, years
|
|
< 10
|
5 (4.0)
|
0 (0.0)
|
|
10–20
|
38 (30.2)
|
3 (2.4)
|
|
20–32
|
83 (65.9)
|
123 (97.6)
|
|
Sex
|
|
Male
|
64 (50.8)
|
92 (73.0)
|
|
Female
|
62 (49.2)
|
34 (27.0)
|
|
HBV screening
|
|
HBsAg, %
|
0 (0.0)
|
5 (4.0)
|
|
Anti HBsAb, %
|
29 (23.0)
|
109 (86.5)
|
|
Anti HBcAb, %
|
2 (1.6)
|
0 (0.0)
|
|
IBD type
|
|
Crohn’s disease
|
104 (82.5)
|
NA
|
|
Ulcerative colitis
|
22 (17.5)
|
NA
|
|
Body mass index
|
|
Normal weight
|
64 (50.8)
|
NA
|
|
Underweight
|
36 (28.6)
|
NA
|
|
Overweight
|
14 (11.1)
|
NA
|
|
Obese
|
12 (9.5)
|
NA
|
|
Patients with comorbidities
|
|
Single comorbidity
|
75 (59.5)
|
NA
|
|
Two or more comorbidities††
|
7 (5.6)
|
NA
|
|
Total
|
82 (65.1)
|
NA
|
|
Comorbidity type
|
|
Iron deficiency anemia
|
80 (63.5)*
|
NA
|
|
Hypoalbuminemia
|
8 (6.3)*
|
NA
|
IBD: inflammatory bowel disease; HBV: hepatitis B virus; HBsAg: hepatitis B surface antigen; anti-HBs: hepatitis B surface antibody; anti-HBc: hepatitis B core antibody; ††Five with iron deficiency anemia and hypo albuminemia, two with iron deficiency anemia and type 2 diabetes, and one with all three comorbidities. NA: not applicable.
Most patients with IBD received immunosuppressive therapy (82.5%), including hydrocortisone (57.1%), prednisolone (38.1%), and the biologic agent infliximab (35.7%). Two IBD medications had a statistically significant association with low anti-HBs levels: prednisolone (p = 0.016) and esomeprazole (p < 0.001) [Table 2].
Table 2: Relation between medication and immunogenicity in Omani IBD patients (n = 126).
|
Corticosteroids
|
Prednisolone
|
48 (38.1)
|
0.016*
|
|
Hydrocortisone
|
72 (57.1)
|
0.975
|
|
Methylprednisolone
|
42 (33.3)
|
0.767
|
|
Dexamethasone
|
22 (17.5)
|
1.000
|
|
Antibiotics
|
Amoxicillin
|
16 (12.7)
|
0.705
|
|
Clarithromycin
|
14 (11.1)
|
1.000
|
|
Erythromycin
|
15 (11.9)
|
0.519
|
|
Cloxacillin
|
9 (7.1)
|
1.000
|
|
Biologic agents
|
Infliximab
|
45 (35.7)
|
1.000
|
|
Adalimumab
|
12 (9.5)
|
0.180
|
|
Proton pump inhibitor
|
Esomeprazole
|
41 (32.5)
|
< 0.001*
|
IBD: inflammatory bowel disease. *Significant.
There were no significant relationships between IBD patients’ sex, age, type of IBD, co-morbidities, or BMI with anti-HBs levels [Table 3].
Table 3: Association between baseline variables and immunity to scheduled hepatitis B vaccine among Omani IBD patients (n = 126).
|
Sex
|
Male
|
64
|
18 (28.1)
|
46 (71.9)
|
1.916
|
0.166
|
|
Female
|
62
|
11 (17.7)
|
51 (82.3)
|
|
Age(years)
|
< 10
|
5
|
3 (60.0)
|
2 (40.0)
|
9.796
|
0.106
|
|
10–20
|
38
|
3 (7.9)
|
35 (92.1)
|
|
20–32
|
83
|
23 (27.7)
|
60 (72.3)
|
|
Type of IBD
|
Crohn’s disease
|
104
|
25 (24.0)
|
79 (76.0)
|
0.099
|
0.753
|
|
Ulcerative colitis
|
22
|
4 (18.2)
|
18 (81.8)
|
|
Comorbidities
|
No
|
44
|
12 (27.3)
|
32 (72.7)
|
0.691
|
0.406
|
|
Yes
|
82
|
17 (20.7)
|
65 (79.3)
|
|
Underweight
|
36
|
7 (19.4)
|
29 (80.6)
|
|
Normal
|
64
|
15 (23.4)
|
49 (76.6)
|
|
Overweight
|
14
|
6 (42.9)
|
8 (57.1)
|
IBD: inflammatory bowel disease.
Discussion
This study evaluated the long-term immunogenicity of scheduled HBV vaccine in Omani patients with IBD and compared it with healthy controls. It is reported that HBV evokes an adequate immune response in 86.5% of healthy individuals, but inadequately in immunosuppressed individuals.11 Consistent with this, our patients had a significantly weaker immune response to the HBV vaccine than controls.11
Two mechanisms have been proposed to explain this impaired response. First, pre-existing immune deficiencies may lead to a suboptimal initial response. These deficiencies may have arisen from genetic polymorphisms affecting monocyte receptors, macrophage function, and cytokine secretion, or chronic disease-related impairment of immune competence.9,12 Second, some individuals who initially mount a robust initial immune response may experience waning immunity due to malnutrition or the use of immunosuppressants, with effects varying by drug type, dosage, and timing.8,11,13
Our findings also align with reports of lower immune response to HBV vaccination (24–36%) in pediatric IBD patients.14,15 In contrast, a study in Italy reported 61.6% anti-HBs positivity among 99 IBD patients, 38.6% higher than ours.16 It is suggested that routine administration of a booster HBV vaccine dose to all Italian children aged 12 years may have enhanced their immune response.17
In a study in Turkey, IBD patients had a lower immune response to HBV vaccination compared to controls.18 A meta-analysis by Kochhar et al,19 of 14 studies comprising 2375 IBD patients, similarly reported significantly reduced immune response to HBV vaccine in IBD patient populations (p = 0.001).
Similarly, a 2022 meta-analysis of 21 studies involving 2602 patients with IBD found HBV vaccine response rate to be significantly lower among patients receiving immunosuppressive therapy than those who did not. The authors recommended administering the vaccine during disease remission when patients receive minimal or no immunosuppressive thereapy.20
Immunosuppressive drugs for IBD may have varying impact HBV vaccine effectiveness. For example, a prospective observational study in Kuwait reported that patients with UC treated with infliximab had lower immune response to HBV vaccine compared to those treated with 5-ASA.11
Previous studies have consistently linked infliximab and adalimumab with impaired responses to both HBV and COVID-19 vaccines.21,22 However, our findings did not reveal a significant association between anti-TNF and the blunted immune response. This discrepancy seems to be attributable to differences in epidemiological characteristics. In fact, our IBD cohorts may have been unique in parameters such as younger mean age (22.3 years), ethnicity, disease severity, duration of therapy, concomitant medications, or individual responses, though this lacks empirical evidence. The observed lack of significant association could also be attributed to sample size limitations.
Our study found a significant association (p = 0.016) between prednisolone use and lower anti-HBs levels in patients with IBD. This aligns with the previously reported lack of effectiveness of the HBV vaccine in eliciting an immune response in children with nephrotic syndrome undergoing steroid therapy.23 A standard corticosteroid taper spans roughly 12 weeks, contrasting with the typical 5-day hydrocortisone and methylprednisolone course administered during hospitalizations. This raises the possibility that the duration of steroid exposure rather than its type contributes to the observed impairment of immunogenicity. However, further investigation is warranted to determine the mechanisms linking prednisolone use and vaccine response in this patient population.
A significant association (p < 0.001) between esomeprazole use and suboptimal immune response to the HBV vaccine was observed in our cohort. Recently, many authors suggested that chronic use of proton pump inhibitors (PPIs) such as esomeprazole might influence the gut microbiome, potentially altering the immune system and increasing vulnerability to autoimmune diseases.24–26 Such alterations were recently suggested in connection with vaccine response.27–29
On the same line, PPIs have been proven to have a direct impact on the immune system. Growing evidence suggests that PPIs exert multifaceted effects on the immune system. Preclinical in-vivo studies have demonstrated that, unlike H2 receptor antagonists, PPIs exhibit pleiotropic effects, targeting a range of immune defense molecules, including tumor necrosis factor-alpha, interleukin-1 beta, interleukin-6, and nuclear factor kappa B.30 Further supporting these findings, recent clinical research indicates that pantoprazole modulates the immune response by downregulating the expression of interferon-gamma and interleukin-2. This modulation appears to be mediated through the regulation of key signaling molecules.31 Further studies are needed to clarify the mechanisms by which esomeprazole might affect vaccine response in IBD patients.
Our analysis did not reveal significant associations between demographic factors in patients with IBD and their response to the HBV vaccine. This agrees with the results of a recent meta-analysis that involved 2602 patients with IBD, where the response rate to HBV vaccine was not affected by sex, IBD subtype, or disease severity.9 However, unlike the findings of Cossio-Gil et al,9 our data did not show an association between younger age and higher anti-HBs (HbsAb) levels. This disparity is likely explained by our significantly younger cohort (mean age 22.3 vs. 44.5 years). Further research across a wider age range is warranted to better determine the influence of age.
CD was the most prevalent form of IBD in this cohort (82.5%). While 18.2% of patients with UC showed adequate HbsAb levels, 24.0% of patients with CD achieved an adequate response to the HBV vaccine, but this difference lacked statistical significance. This data supports the findings of Altunöz et al,18 who reported comparable immunogenicity to the HBV vaccine in patients with both UC and CD. Traditionally, CD is more associated with the need for immunosuppression than UC.32 Nevertheless, the overrepresentation of CD patients and a selection bias towards younger ages in our study might have influenced the observed prevalence of this specific IBD subtype.
Our study did not find significant associations between comorbidities such as iron deficiency anemia, hypoalbuminemia, and type 2 diabetes and suboptimal immune response to the HBV vaccine. This finding contrasts with that of Cossio-Gil et al,9 in Spain, who reported a significant association between certain comorbidities (primarily hypertension) and low immune response to HBV vaccination in patients with IBD. Additionally, the association between obesity and poor HBV vaccine response seen in the Spanish cohort was not observed in ours, possibly because our patients were younger and most had a normal BMI.
While previous research has indicated a decline in vaccine response to HBV with age, as evidenced by lower HBsAb levels in older populations, our participants exhibited stable HBsAb levels across all age groups. This finding underscores the potential impact of drug therapy on vaccine response, suggesting that drug-related factors may outweigh the effects of aging in influencing immune responses to HBV vaccination.33,34
None of the IBD patients in this study tested positive for HB surface antigen (HBsAg), indicating no current HBV infection. In contrast, the control group exhibited a 4.0% HBsAg positivity rate. This unexpected finding warrants further investigation. Potential explanations could include the higher mean age of the control group (27.7 years) versus (22.3 years) for IBD group in addition to limitations in screening protocols. A previous study by Al-Busafi et al,35 identified a higher prevalence of HBsAg among males residing in the Muscat governorate, potentially due to risk factors like barber shaving and intra-familial contact.Future research should explore these possibilities in a larger cohort to gain a clearer understanding of the observed distribution of HBsAg positivity.
Several limitations inherent to the study design warrant cautious interpretation of the findings. The single-center retrospective design limits generalizability to other populations and restricts control of potential confounders such as vaccine type and dosage. In addition, incomplete data in the healthcare tracking system required participant exclusion, which may have introduced selection bias and reduced cohort representativeness.
Conclusion
This study demonstrates a significantly lower immune response to the HBV vaccine in Omani patients with IBD compared with healthy controls. This finding suggests impaired immune regulation in IBD that may hinder vaccine responsiveness. Treatment with immunosuppressive medications such as prednisolone and proton pump inhibitors also appears to be associated with a suboptimal HBV vaccine response in this population. Although we found no statistically significant associations between vaccine response and age, sex, IBD subtype, comorbidities, or BMI, further studies in larger and more diverse cohorts are needed to clarify these potential influences.
Disclosure
The authors declare no conflicts of interest. No funding was received for this study.
references
- 1. Mosli M, Alawadhi S, Hasan F, Abou Rached A, Sanai F, Danese S. Incidence, prevalence, and clinical epidemiology of inflammatory bowel disease in the Arab world: a systematic review and meta-analysis. Inflamm Intest Dis 2021 Sep;6(3):123-131.
- 2. Calvez V, Puca P, Vincenzo FD, Del Gaudio A, Bartocci B, Murgiano M, et al. Novel insights into the pathogenesis of inflammatory bowel diseases. Biomedicines 2025 Jan;13(2):305.
- 3. Ardabili AR, Esser DV, Wintjens D, Cilissen M, Deben D, Mujagic Z, et al. The risk of mild, moderate, and severe infections in ibd patients – a prospective, multicentre observational cohort study (PRIQ). J Crohns Colitis 2025 Jul:jjaf112.
- 4. Mårild K, Söderling J, Axelrad J, Halfvarson J, Forss A, Olén O, et al; SWIBREG Study Group. Histologic activity in inflammatory bowel disease and risk of serious infections: a nationwide study. Clin Gastroenterol Hepatol 2024 Apr;22(4):831-846.
- 5. López-Serrano P, Pérez-Calle JL, Sánchez-Tembleque MD. Hepatitis B and inflammatory bowel disease: role of antiviral prophylaxis. World J Gastroenterol 2013 Mar;19(9):1342-1348.
- 6. Al Awaidy ST, Bawikar SP, Al Busaidy SS, Al Mahrouqi S, Al Baqlani S, Al Obaidani I, et al. Progress toward elimination of hepatitis B virus transmission in Oman: impact of hepatitis B vaccination. Am J Trop Med Hyg 2013 Oct;89(4):811-815.
- 7. Gisbert JP, Villagrasa JR, Rodríguez-Nogueiras A, Chaparro M. Efficacy of hepatitis B vaccination and revaccination and factors impacting on response in patients with inflammatory bowel disease. Am J Gastroenterol 2012 Oct;107(10):1460-1466.
- 8. Carrera E, Manzano R, Garrido E. Efficacy of the vaccination in inflammatory bowel disease. World J Gastroenterol 2013 Mar;19(9):1349-1353.
- 9. Cossio-Gil Y, Martínez-Gómez X, Campins-Martí M, Rodrigo-Pendás JÁ, Borruel-Sainz N, Rodríguez-Frías F, et al. Immunogenicity of hepatitis B vaccine in patients with inflammatory bowel disease and the benefits of revaccination. J Gastroenterol Hepatol 2015 Jan;30(1):92-98.
- 10. Elbahrawy A, Atalla H, Alboraie M, Alwassief A, Madian A, El Fayoumie M, et al. Recent advances in protective vaccines against hepatitis viruses: a narrative review. Viruses 2023 Jan;15(1):214.
- 11. Shehab M, Alrashed F, Alyaseen M, Safar Z, Adekunle T, Alfadhli A, et al. Immunogenicity of hepatitis B vaccination in patients with ulcerative colitis on infliximab is attenuated compared to those on 5-aminosalicylic acid therapies: a prospective observational study. Vaccines (Basel) 2024 Mar;12(4):364.
- 12. Watts A, Bennett W, Molleston J, Gupta S, Croffie J, Waseem S, et al. P-222 YI hepatitis B immunity in inflammatory bowel disease. Inflamm Bowel Dis 2016;22:S76.
- 13. Pratt PK Jr, Nunes D, Long MT, Farraye FA. Improved antibody response to three additional hepatitis b vaccine doses following primary vaccination failure in patients with inflammatory bowel disease. Dig Dis Sci 2019 Jul;64(7):2031-2038.
- 14. Aljaberi N, Ghulam E, Smitherman EA, Favier L, Dykes DM, Danziger-Isakov LA, et al. Maintaining hepatitis B protection in immunocompromised pediatric rheumatology and inflammatory bowel disease patients. J Rheumatol 2021 Aug;48(8):1314-1321.
- 15. Watts A, Bennett WE, Molleston JP, Gupta SK, Croffie JM, Waseem S, et al. Incidence of low seroimmunity to hepatitis B virus in children with inflammatory bowel disease. J Pediatr Gastroenterol Nutr 2017 Nov;65(5):551-554.
- 16. Chang JY, Jung SA, Moon CM, Kim SE, Jung HK, Shim KN. Response to hepatitis B vaccination in patients with inflammatory bowel disease: a prospective observational study in Korea. Intest Res 2018 Oct;16(4):599-608.
- 17. Stroffolini T, Stroffolini G. Vaccination campaign against hepatitis B virus in Italy: a history of successful achievements. Vaccines (Basel) 2023 Sep;11(10):1531.
- 18. Altunöz ME, Senateş E, Yeşil A, Çalhan T, Ovünç AO. Patients with inflammatory bowel disease have a lower response rate to HBV vaccination compared to controls. Dig Dis Sci 2012 Apr;57(4):1039-1044.
- 19. Kochhar GS, Mohan BP, Khan SR, Chandan S, Kassab LL, Ponnada S, et al. Hepatitis-B vaccine response in inflammatory bowel disease patients: a systematic review and meta-analysis. Inflamm Bowel Dis 2021 Oct;27(10):1610-1619.
- 20. Singh AK, Jena A, Mahajan G, Mohindra R, Suri V, Sharma V. Meta-analysis: hepatitis B vaccination in inflammatory bowel disease. Aliment Pharmacol Ther 2022 Apr;55(8):908-920.
- 21. Kennedy NA, Lin S, Goodhand JR, Chanchlani N, Hamilton B, Bewshea C, et al; Contributors to the CLARITY IBD study. Infliximab is associated with attenuated immunogenicity to BNT162b2 and ChAdOx1 nCoV-19 SARS-CoV-2 vaccines in patients with IBD. Gut 2021 Oct;70(10):1884-1893.
- 22. Pratt PK, David N, Weber HC, Little FF, Kourkoumpetis T, Patts GJ, et al. Antibody response to hepatitis B virus vaccine is impaired in patients with inflammatory bowel disease on infliximab therapy. Inflamm Bowel Dis 2018;24 2(2):380-386.
- 23. Yıldız N, Sever L, Kasapçopur Ö, Çullu F, Arısoy N, Çalışkan S. Hepatitis B virus vaccination in children with steroid sensitive nephrotic syndrome: immunogenicity and safety? Vaccine 2013 Jul;31(33):3309-3312.
- 24. Lin SH, Chang YS, Lin TM, Hu LF, Hou TY, Hsu HC, et al. Proton pump inhibitors increase the risk of autoimmune diseases: a nationwide cohort study. Front Immunol 2021 Sep;12:736036.
- 25. Waszczuk E, Waszczuk KM, Mulak A, Paradowski L. Inadequate seroprotection against hepatitis B virus and one detected case of hepatitis C virus infection among patients with inflammatory bowel disease. Eur J Gastroenterol Hepatol 2016 Jun;28(6):628-632.
- 26. Wilhelm SM, Rjater RG, Kale-Pradhan PB. Perils and pitfalls of long-term effects of proton pump inhibitors. Expert Rev Clin Pharmacol 2013 Jul;6(4):443-451.
- 27. Airola C, Andaloro S, Gasbarrini A, Ponziani FR. Vaccine responses in patients with liver cirrhosis: from the immune system to the gut microbiota. Vaccines (Basel) 2024 Mar;12(4):349.
- 28. Decker V, Qureshi K, Roberts L, Powell N, Marchesi JR, Mullish BH, et al. The emerging role of the gut microbiota in vaccination responses. Gut Microbes 2025 Dec;17(1):2549585.
- 29. Liu Y, Zhou J, Yang Y, Chen X, Chen L, Wu Y. Intestinal microbiota and its effect on vaccine-induced immune amplification and tolerance. Vaccines (Basel) 2024 Aug;12(8):868.
- 30. Balza E, Piccioli P, Carta S, Lavieri R, Gattorno M, Semino C, et al. Proton pump inhibitors protect mice from acute systemic inflammation and induce long-term cross-tolerance. Cell Death Dis 2016 Jul;7(7):e2304.
- 31. Liu W, Jakobs J, Rink L. Proton-pump inhibitors suppress T cell response by shifting intracellular zinc distribution. Int J Mol Sci 2023 Jan;24(2):1191. doi:10.3390/IJMS24021191.
- 32. Siegel CA, Yang F, Eslava S, Cai Z. Treatment pathways leading to biologic therapies for ulcerative colitis and crohn’s disease in the United States. Clin Transl Gastroenterol 2020 Feb;11(2):e00128.
- 33. Cekic C, Aslan F, Kirci A, Gümüs ZZ, Arabul M, Yüksel ES, et al. Evaluation of factors associated with response to hepatitis B vaccination in patients with inflammatory bowel disease. Medicine (Baltimore) 2015 Jun;94(22):e940.
- 34. Jiang HY, Wang SY, Deng M, Li YC, Ling ZX, Shao L, et al. Immune response to hepatitis B vaccination among people with inflammatory bowel diseases: a systematic review and meta-analysis. Vaccine 2017;35(20):2633-2641.
- 35. Al-Busafi SA, Al-Harthi R, Al-Naamani K, Al-Zuhaibi H, Priest P. Risk factors for hepatitis B virus transmission in Oman. Oman Med J 2021 Jul;36(4):e287.