Intestinal malrotations are one of the most interesting yet challenging cases for clinicians. They can be broadly defined as any deviation in the position of the intestines from their normal anatomical location.1 This can include the small bowel, the large bowel, or both, and can be associated with abnormal fixation or non-fixation of the bowel, which predisposes to obstruction.1
Classically, small bowel malrotations have been extensively studied and classified, while isolated hindgut malrotations are rare. Even rarer are hindgut malrotations associated with an internal hernia and an enteric duplication cyst, which is the case we present here.
Case Report
An eight-year-old boy was admitted with severe acute abdominal pain that was spastic and intermittent in nature, associated with multiple episodes of bilious vomiting. The child was malnourished, but his physical and blood investigations were unremarkable. He gave a history of similar intermittent episodes in the past, which had been managed conservatively in multiple other hospitals.
Ultrasonography of the abdomen revealed that the small bowel loops were predominantly on the left side of the abdomen, and the large bowel loops were on the right side. Additionally, on the left side of the abdomen, a cyst with internal echoes having a gut signature was seen in relation to the bowel, indicating an intestinal duplication cyst.
The contrast-enhanced computed tomography (CECT) abdomen findings were as follows: The D3 segment of the duodenum was seen to cross to the left side with the duodeno-jejunal junction in its expected location. The superior mesenteric arter-superior mesenteric vein (SMA-SMV) relationship was maintained with the SMV lying on the right side of SMA. The small bowel loops were predominantly on the left side of the abdomen, and the entire colonic loops were positioned on the right side of the abdomen [Figure 1]. The ileocecal junction (ICJ), cecum, and appendix were noted in the right lumbar region [Figure 2]. The inferior mesenteric artery was seen coursing to the right side of the midline, rather than its normal left-sided course [Figure 3]. A tubular cystic lesion was observed in relation to the small bowel loops on the left side of the abdomen [Figure 4]. Intrabdominal solid organs were essentially normal, with a normal situs.
 Figure 1: Coronal sections of the contrast-enhanced computed tomography scan of the abdomen, showing the abnormal positioning of the small bowel loops on the left side (red arrow), and the large bowel loops on the right side (blue arrow), suggesting the possibility of hindgut malrotation.
Figure 1: Coronal sections of the contrast-enhanced computed tomography scan of the abdomen, showing the abnormal positioning of the small bowel loops on the left side (red arrow), and the large bowel loops on the right side (blue arrow), suggesting the possibility of hindgut malrotation.
 Figure 2: Coronal sections of contrast-enhanced computed tomography abdomen showing the position of the ileocecal junction (red arrow), cecum and appendix (blue arrow) in the right lumbar region.
Figure 2: Coronal sections of contrast-enhanced computed tomography abdomen showing the position of the ileocecal junction (red arrow), cecum and appendix (blue arrow) in the right lumbar region.
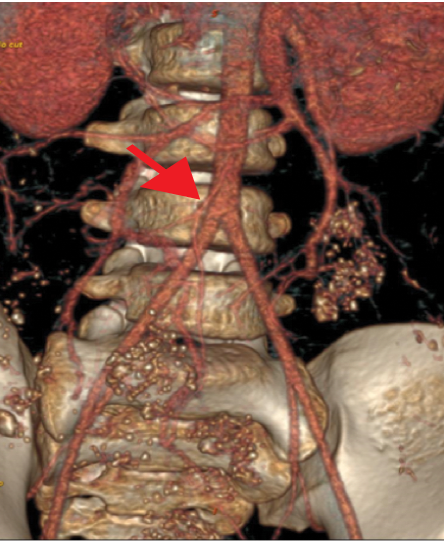 Figure 3: 3D volume-rendered contrast-enhanced computed tomography arterial phase images showing the abnormal right-sided course of the inferior mesenteric artery (red arrow).
Figure 3: 3D volume-rendered contrast-enhanced computed tomography arterial phase images showing the abnormal right-sided course of the inferior mesenteric artery (red arrow).
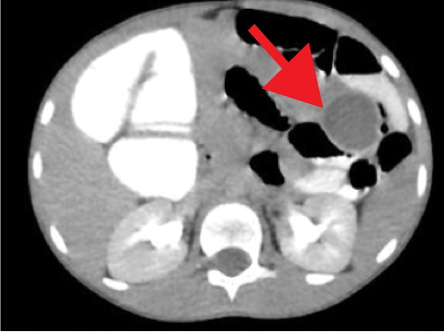 Figure 4: Axial sections of contrast-enhanced computed tomography abdomen showing a well-defined fluid filled cyst (red arrow) on the left side of the abdomen in relation to the small bowel loops.
Figure 4: Axial sections of contrast-enhanced computed tomography abdomen showing a well-defined fluid filled cyst (red arrow) on the left side of the abdomen in relation to the small bowel loops.
A diagnosis of isolated hindgut malrotation associated with an enteric duplication cyst was suggested. Surgical findings confirmed the diagnosis, with the colonic loops lying on the right side of the abdomen and small bowel loops on the left side. A tubular duplication cyst was observed along the distal jejunum and proximal ileum. An additional and interesting finding was that the ascending colon had mesentery, and there was a defect in the ascending colon mesentery, through which the terminal ileum, ICJ , cecum, and appendix were herniating [Figure 5]. The ascending colon was also noted to be twisted along its vascular axis. The twisted portion of the ascending colon was resected and the remaining ends were re-anastomosed. The position of the ICJ junction and terminal ileum was corrected. A part of the small bowel loop, specifically the distal jejunal-proximal ileal loops containing the duplication cyst, was excised [Figure 6].
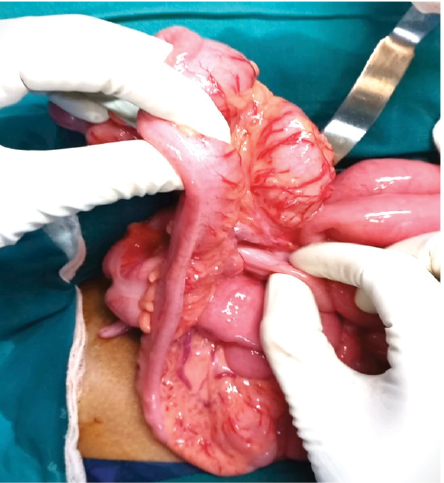 Figure 5: Intraoperative image showing the herniation of the ileocecal junction, cecum, and appendix through the mesenteric defect of the ascending colon.
Figure 5: Intraoperative image showing the herniation of the ileocecal junction, cecum, and appendix through the mesenteric defect of the ascending colon.
 Figure 6: Resected surgical specimen of small bowel and the associated intestinal duplication cyst (along the mesenteric border). Arrows show the duplication cyst.
Figure 6: Resected surgical specimen of small bowel and the associated intestinal duplication cyst (along the mesenteric border). Arrows show the duplication cyst.
Histopathology examination confirmed the diagnosis of an enteric duplication cyst, which also contained ectopic gastric mucosa. Following the procedure, the child showed complete symptomatic relief. He is now on a normal diet and is gaining weight. Written consent was obtained from the patient’s mother.
Discussion
Malrotation limited to the colon is much rarer than that of the small bowel alone or that of both the small and large bowel together.2 It is suspected when an abnormal position of the colon is seen in conjunction with a normal position of the small bowel. The presence of associated complications with an abnormal course of the inferior mesenteric artery helps confirm the diagnosis.3,4 Colonic volvulus is the most common complication of such malrotations.5,6
Internal hernias are defined as the herniation of viscera through an orifice in the peritoneum or mesentery.7 Although the most common clinical manifestation is small bowel obstruction, they can remain clinically silent or cause intermittent obstruction in cases where they are self-reducing.7,8 Radiological features such as an abnormal location or crowding of small bowel loops, evidence of intestinal obstruction, features of apparent fixation, and mesenteric vessel abnormalities guide us to the diagnosis of an internal hernia.7 Preoperatively, a radiological diagnosis of an internal hernia could not be made in our case. It is presumed that the herniations were transient and self-resolving, and that none were present during the scan. The clinical history intermittent self-resolving abdominal pain of the child also supports this postulation.
Enteric duplication cysts are rare congenital malformations of the intestinal tract closely attached to the gut wall, lined with intestinal epithelium.9 Complications include recurrent abdominal pain, intussusception, obstruction, and bleeding.10 Ultrasound typically shows a cyst in relation to the gut, with a double-wall gut signature.9 CT and magnetic resonance imaging can depict the location and extension of the cyst, complications, associated anomalies, and anatomical relationships.10
Conclusion
Isolated hindgut malrotations are rare entities. Whenever an abnormal position of a bowel is encountered, its vascular course and other related pathologies predisposing to bowel obstruction should be thoroughly checked. A mesenteric fluid-filled structure in relation to the bowel should raise the possibility of an enteric duplication cyst.
Disclosure
The authors declared no conflicts of interest.
references
- 1. Pickhardt PJ, Bhalla S. Intestinal malrotation in adolescents and adults: spectrum of clinical and imaging features. AJR Am J Roentgenol 2002 Dec;179(6):1429-1435.
- 2. Balthazar EJ. Intestinal malrotation in adults. Roentgenographic assessment with emphasis on isolated complete and partial nonrotations. AJR Am J Roentgenol 1976 Feb;126(2):358-367.
- 3. Applegate KE, Anderson JM, Klatte EC. Intestinal malrotation in children: a problem-solving approach to the upper gastrointestinal series. Radiographics 2006;26(5):1485-1500.
- 4. Jansen JO, Driver CP, Duncan JL. Unusual hindgut malrotation and associated mesenteric vascular abnormality presenting as large bowel obstruction in an adult. Surgeon 2007 Apr;5(2):109-110, quiz 110, 121.
- 5. Black RE, Cox JA. Volvulus of the transverse colon in children–Report of a case and review of the literature. Z Kinderchir 1984 Feb;39(1):69-71.
- 6. Anderson JR, Lee D, Taylor TV, Ross AH. Volvulus of the transverse colon. Br J Surg 1981 Mar;68(3):179-181.
- 7. Martin LC, Merkle EM, Thompson WM. Review of internal hernias: radiographic and clinical findings. AJR Am J Roentgenol 2006 Mar;186(3):703-717.
- 8. Doishita S, Takeshita T, Uchima Y, Kawasaki M, Shimono T, Yamashita A, et al. Internal hernias in the era of multidetector CT: correlation of imaging and surgical findings. Radiographics 2016;36(1):88-106.
- 9. Sangüesa Nebot C, Llorens Salvador R, Carazo Palacios E, Picó Aliaga S, Ibañez Pradas V. Enteric duplication cysts in children: varied presentations, varied imaging findings. Insights Imaging 2018 Dec;9(6):1097-1106.
- 10. Lee NK, Kim S, Jeon TY, Kim HS, Kim DH, Seo HI, et al. Complications of congenital and developmental abnormalities of the gastrointestinal tract in adolescents and adults: evaluation with multimodality imaging. Radiographics 2010 Oct;30(6):1489-1507.