|
Introduction
Asymmetry is common and most unusual error of human reproduction. Sometimes, some painless lesions lead to facial asymmetry, in which case they become painful for life. The asymmetric overgrowth traditionally termed hemihypertrophy is more accurately referred to as hemihyperplasia, since the pathologic growth process involves an abnormal proliferation of cells (hyperplasia), rather than an increase in size of existing cells (hypertrophy).1 In patients affected by hemifacial hyperplasia, asymmetry is more marked than in normal individuals. Most of the time, this disorder is congenital but few cases have been recorded where the condition developed after birth.2 Facial asymmetry caused by this condition becomes more evident as age increases, and its features are completely expressed at the time puberty.3 It can affect the entire half of the body or may involve only the face. When it affects the entire half of the body, it is called complex hemihyperplasia. When one or both limbs are involved it is called simple hemihyperplasia and when it affects face, head and associated structures, it is called hemifacial hyperplasia.2
Many theories have been proposed on the cause of hemifacial hyperplasia, including hormonal imbalances, diseases involving the neural system, vascular conditions (such as hemangiomas and arteriovenous malformations), abnormalities (such as lymphangioma, incomplete twinning, abnormal intrauterine environment, somatic mutations, and central nervous system lesions), mechanical influences, and congenital syphilis.4 Thus, many authors consider the development of prenatal teeth to be a good indication of future malformation. This report describes a rare case of hemifacial hyperplasia on the left side of the face of a 50- year-old female who presented with unilateral facial enlargement since birth.
Case Report
A 50-year-old female presented at the outpatient department of Oral Medicine and Radiology, with complaints of ulcers on the left cheek and posterior part of mouth for the past 7 days (Figs. 1 and 2). The patient’s history revealed that she developed the ulcers for the first time when she scratched that area due to a tingling sensation. Ulcers were smaller in size which increased gradually to reach the present size. Family history was noncontributory.

Figure 1: Female patient presented with unilateral facial enlargement.

Figure 2: Showing ulcers on palate and left buccal mucosa.
Extra-oral examination revealed gross facial asymmetry with diffuse swelling on the left side of the face which was present since birth. On inspection, the swelling extended supero-inferiorly from the infra-orbital ridge to the lower border of mandible and antero-posteriorly from the midline to the left pre auricular region, with smooth overlying surface. The color of the overlying skin was same as that of the surrounding skin. On palpation, the swelling was soft and nontender, temperature was not raised and it was not associated with any discharge. There was a deviation of the chin towards the normal side and the lower lip was larger on the affected side with drooping of the corner of the mouth on the same side.
On intra-oral examination, a solitary oval ulcer was seen on the left buccal mucosa and palate roughly measuring 0.5 × 0.5 cm in diameter with well-defined erythematous margins. The base of the ulcer was filled with necrotic slough. On palpation, it was nontender and was not associated with any discharge. The left buccal mucosa was thickened and pendulous. The tongue was considerably enlarged (Fig. 3), with enlargement of upper and lower left alveolus, left upper premolar was larger compared to its counterpart. Based on history and clinical examination, a provisional diagnosis of traumatic ulcer on palate and left buccal mucosa as well as hemifacial hyperplasia on the left side of the face was made. The differential diagnosis of condylar hyperplasia was considered (which is an uncommon malformation of the mandible caused by excessive growth of condyle), it is difficult to differentiate between hemifacial hyperplasia and condylar hyperplasia clinically, but it can be easily distinguished radiographically owing to the involvement of soft tissue and other bones in hemifacial hyperplasia.
Figure 3: Enlargement of tongue on affected side.
Panoramic radiography displayed hyperplasia (increase in size) of maxilla and mandible including condylar process, ramus, and body on the left side. The size of the mandibular canal on the left side was also increased (Fig 4). To better define the facial deformity, CT scan was performed which showed the left maxilla, mandible and sphenoid to be enlarged including the palatal and zygomatic bones (Figs. 5 and 6). An increased size of maxillary sinus was also realized on the affected side. CT also demonstrated an enlargement of the subcutaneous fat and masseter muscle on the affected side (Fig. 7), these extensive clinical and radiographic abnormalities were considered to justify a diagnosis of hemifacial hyperplasia.

Figure 4: OPG showing enlarged maxilla and mandible on left side.

Figure 5: CT scan showing enlarged soft tissue on left side.

Figure 6: CT scan shows great discrepancy in both right and left condyle.
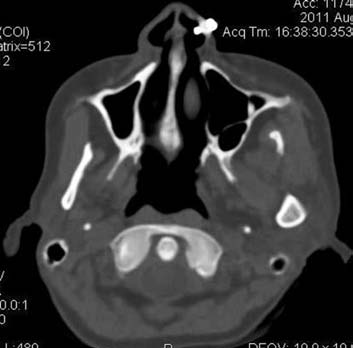
Figure 7: Showing increased size of maxillary sinus on affected side.
For treatment, discarding the irritation or triggering agent was advised, and the ointment Dologel was prescribed for ulcers and replacement of missing teeth was also advised, but no therapy was instituted for the facial deformity, to which the patient expressed reluctance, but she was recalled after 2 weeks and periodic clinical and radiographic assessment was recommended.
Discussion
Hemifacial hyperplasia represents a developmental anomaly characterized by unilateral enlargement of the face involving single or multiple tissues including the underlining bone on the affected side.5 Congenital hemifacial hyperplasia also known as hemifacial hypertrophy was initially described by Merckel in 1822 and Wagner in 1839, who coined it as a sporadic congenital condition.6 Its true incidence is unknown and to our knowledge, very few references are available in the literature, and though it is often called hemifacial hypertrophy, it may be more accurately termed "hemifacial hyperplasia" to reflect the underlying pathology.
Etiology is unknown although various factors have been mentioned. There is little evidence suggesting that heredity plays a role, but the condition has been ascribed to vascular and lymphatic malformations, as well as endocrine and neurocutaneous lesions.3 Pathogenesis is thought to be due to basic fibroblast growth factor and its receptor, which stimulates osteoblast DNA synthesis of the affected side in a more pronounced manner than the normal site.7 Embryologic hypothesis has been proposed by Pollock et al. which implicates the role of neural crest cells for unilateral overgrowth.8
Clinically, it represents as unilateral overgrowth of the orofacial soft tissues, bones, and teeth. The right side of the face is affected most often than the left side and hemifacial hyperplasia is more common in women than in men.9 In an earlier report, we described the condition in a female patient but on the left side. It may be associated with other conditions such as acromegaly and pituitary gigantism, or with hypertrophy of other parts of the body. The asymmetry is always evident at birth and the enlarged side generally grows at a faster rate than the normal side. Growth continues until skeletal maturation and leads to the asymmetry that remains for life. A similar history was given by our current patient, in which growth continued till she attained maturity.
Skeletal deformities have also been noted in hemifacial hypertrophy which includes macrodactyly, polydactyly, syndactyly, scoliosis, tilting of the pelvis, and clubfoot.8 The present case showed only syndactyly. For oro-facial structures, bony hyperplasia is seen in maxilla, mandible, condylar hyperplasia, hyperplasia of frontal bone and sometimes involvement of maxillary sinus, which was also present in our case. Soft tissue involvement leads to the enlargement of muscles on the affected side. Involvement of tongue leads to unilateral enlargement with thickened and hypertrophic fungiform papillae.10 Our patient had the characteristic enlargement of facial muscles and tongue only on the affected side.
Central nervous system involvement may include cerebral enlargement, epilepsy, strabismus, and mental retardation in 15% to 20% of patients, and in some cases dilatation of the pupils on the affected side.4 Genitourinary system disorders such as hypospadias, cryptorchidism and medullary sponge kidney are also noted occasionally.11
Imaging features have been noted for hemifacial hypertrophy which include an increase in the size of condyle, ramus and mandibular canal, along with hyperplasia of the maxillary and mandibular bone as well. It is suggested in the literature that the size of teeth also increases (i.e., size of crown and root) on the affected side, but this was not evident in our patient whose mandibular teeth (from 34 to 38) were missing, but changes were observed in maxillary tooth (i.e., in maxillary premolar), but the rest of the teeth were missing. The rest of the features are consistent with those expressed in our patient. Other uncommon features are thought to include early eruption and idiopathic root resorption, which have been described but were not apparent in our patient.
Treatment procedures are usually planned when physiologic growth ceases. They encompass reconstructive procedures such as ostectomy or orthognathic surgeries.3 Other options include facelifts and orthognathic surgical procedures in conjunction with orthodontic therapy. Overall, prognosis for this disorder is good and none of the cases have as yet shown malignancy.
Conclusion
Sometimes painless lesion becomes painful for life if it leads to gross facial asymmetry. Hemifacial hyperplasia is one such lesion, it is a developmental disorder in which one side of face appear larger than other. Not only soft tissue underlying bone also shows growth discrepancy and appears larger than its normal counterpart. Orthognathic surgery and ostectomies are treatment of choice.
Acknowledgements
The authors reported no conflict of interest and no funding was received for this work.
References
1. Mutafoglu K, Cecen E, Cakmakci H. Isolated hemihyperplasia in an infant: an overlooked sign for wilms tumor development. Iran J Pediatr 2010 Mar;20(1):113-117.
2. Islam MN, Bhattacharyya I, Ojha J, Bober K, Cohen DM, Green JG. Comparison between true and partial hemifacial hypertrophy. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2007 Oct;104(4):501-509.
3. Khanna JN, Andrade NN. Hemifacial hypertrophy. Report of two cases. Int J Oral Maxillofac Surg 1989 Oct;18(5):294-297.
4. Miranda RT, Barros LM, Santos LA, Bonan PR, Martelli H Jr. Clinical and imaging features in a patient with hemifacial hyperplasia. J Oral Sci 2010 Sep;52(3):509-512.
5. Sugiyama M, Tanaka E, Ogawa I, Ishibashi R, Naito K, Ishikawa T. Magnetic resonance imaging in hemifacial hyperplasia. Dentomaxillofac Radiol 2001 Jul;30(4):235-238.
6) Lawoyin J, Daramola J, Lawoyin D. Congenital hemifacial hypertrophy oral surg oral med oral pathol 1989; 68:27-30.
7. Yoshimoto H, Yano H, Kobayashi K, Hirano A, Motomura K, Ohtsuru A, et al. Increased proliferative activity of osteoblasts in congenital hemifacial hypertrophy. Plast Reconstr Surg 1998 Oct;102(5):1605-1610.
8) Pollock R, Newman M, Burdi A, Condit D. Congenital hemifacial hyperplasia: an embryologic hypothesis a case report. Cleft palate 1985; 22:173-183.
9. Neville B, Damm D, Allen C, Bouquot J. Developmental defects of oral and maxillofacial region. In Neville et al oral and maxillofacial pathology. 2nd Edition.Philadelphia, 2002. P.37-38.
10. Azevedo RA, Souza VF, Sarmento VA, Santos JN. Hemifacial hyperplasia: a case report. Quintessence Int 2005 Jun;36(6):483-486.
11. Nayak R, Baliga MS. Crossed hemifacial hyperplasia: a diagnostic dilemma. J Indian Soc Pedod Prev Dent 2007 Mar;25(1):39-42.
|