A 54-year-old female with medical history significant for breast cancer status post right lumpectomy, chemotherapy, and radiation currently in remission, presented with a complaint of progressive dyspnea with exertion over a four-month timeframe. Transthoracic echocardiography (TTE) revealed a left atrial mass raising suspicion of metastasis. The mass was somewhat tubular and thread-like in appearance.
Question
What is the likely diagnosis?
a. Metastatic breast cancer.
b. Atrial myxoma.
c. Papillary fibroelastoma.
d. Cardiac sarcoma.
e. Atrial thrombus.
Answer
b. Atrial myxoma.
Discussion
Subsequent transesophageal echocardiography (TEE) confirmed a highly mobile mass attached to the mid portion of the interatrial septum. Cardiac computed tomography (CCT) was more suggestive of a neoplastic process than a thrombus. Tissue characteristics revealed by cardiac magnetic resonance imaging (cMRI) were most consistent with those of an atrial myxoma [Figure 1]. The patient underwent surgical removal of the left atrial mass with repair of the resulting atrial septal defect. Histological studies confirmed myxoma [Figure 2].
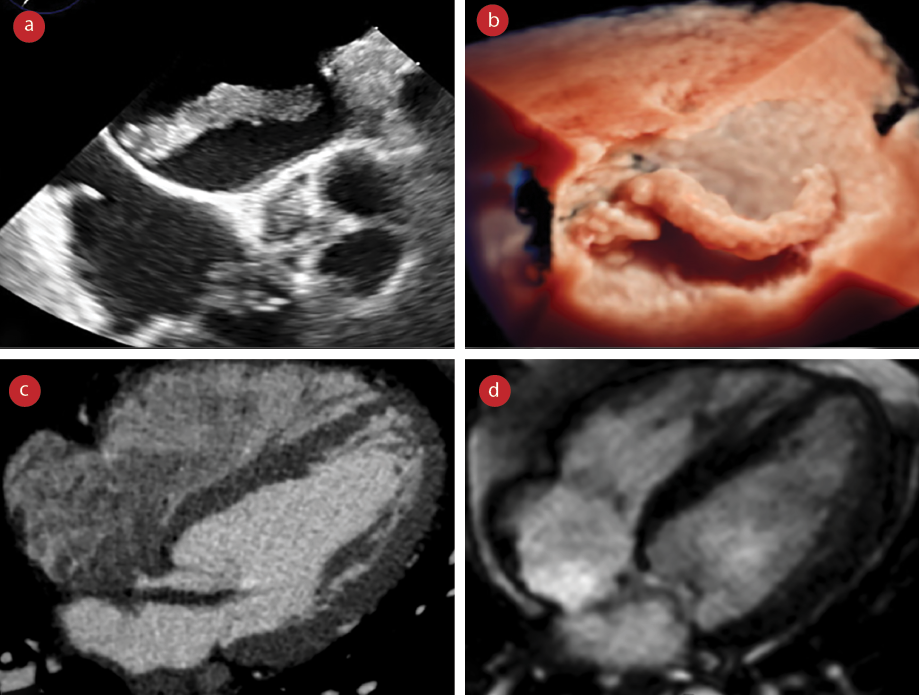 Figure 1: A mobile tubular-like mass which is measuring 7 × 34 mm originating from the left atrial side of fossa ovalis and projecting to the mitral valve. (a) TEE image, (b) 3D-TEE image, (c) CCT image, and
Figure 1: A mobile tubular-like mass which is measuring 7 × 34 mm originating from the left atrial side of fossa ovalis and projecting to the mitral valve. (a) TEE image, (b) 3D-TEE image, (c) CCT image, and
(d) cMRI image.
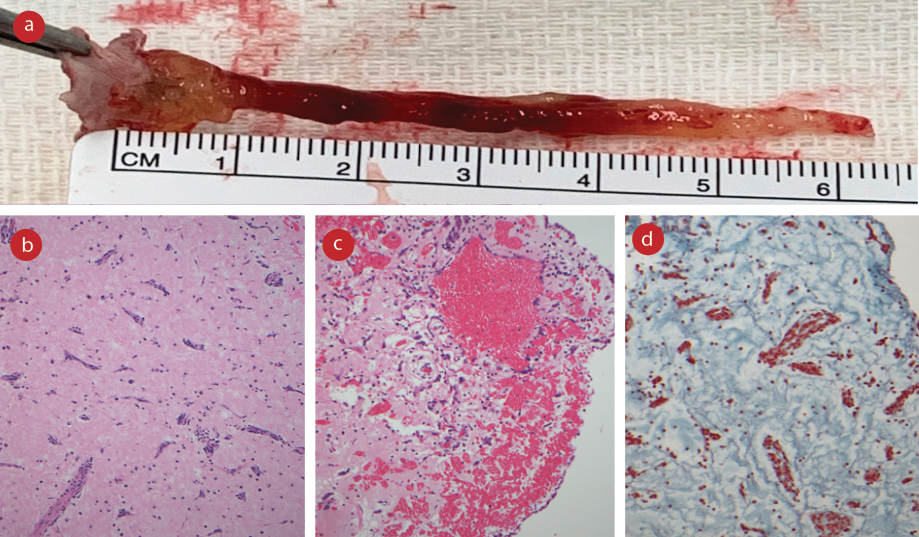 Figure 2: (a) Left atrial mass attached to the fossa ovalis which was removed in one piece by right atriotomy. The mass was ≈ 6 cm in length and gelatinous in texture. (b) Hematoxylin and eosin stain showing myxoma cells, magnification = 100 ×. (c) Subsurface hemorrhage on the removed mass, magnification = 100 ×.
Figure 2: (a) Left atrial mass attached to the fossa ovalis which was removed in one piece by right atriotomy. The mass was ≈ 6 cm in length and gelatinous in texture. (b) Hematoxylin and eosin stain showing myxoma cells, magnification = 100 ×. (c) Subsurface hemorrhage on the removed mass, magnification = 100 ×.
(d) Movat stain showing myxoid stroma, magnification = 100 ×.
This case illustrates the shape and characteristics of a left atrial myxoma. Its usual appearance is as a lobulated hyper-echoic mass. In this case, the mass was more tubular and thread-like. Myxomas are usually solitary. However, multiple atrial, biatrial, atrioventricular, and biventricular tumors have been reported.1,2 The usual size is 0.4–6.5 cm. Symptoms may result from valvular obstruction or emboli but may also be non-specific or absent. A left atrial myxoma has to be differentiated from other cardiac masses such as thrombus.3 Scheffel et al,4 concluded that atrial myxomas and thrombi can be differentiated by their distinguishing features of size, origin, shape, mobility, and prolapse. On echocardiography, myxomas are typically globular, smooth-surfaced, or have irregular friable surface with a multi-lobular appearance. On CCT, they are appreciated as intracavitary lesions, with decreased attenuation compared to surrounding tissues and may have calcified attenuating areas with contrast. MRI can be used to differentiate atrial myxoma from other intracardiac masses (thrombus, fibroelastoma, and malignant tumors) based on tissue characteristics. These characteristics include a variable degree of late gadolinium enhancement uptake, isointense T1, and hyperintense T2. However, T1 and T2 can heterogenous due to varying amounts of myxoid, hemorrhagic, ossific, and necrotic tissues.5 Furthermore, atrial myxomas may be part of the relatively rare Carney complex (< 10%), an autosomal dominant condition that can result from a mutation in the PRKAR1A gene.6
Carney complex may also be associated with extracardiac myxomas, endocrinopathy, and spotty skin pigmentation. Cardiac myxomas occurring in the context of the Carney complex are more likely to occur in atypical (non-left atrium) locations; be multiple; and occur earlier in life. There has been an association with breast cancer, but our patient did not carry a diagnosis of Carney complex.7,8
Our case highlights that a thorough non-invasive work-up must be conducted when dealing with cardiac tumors to differentiate primary cardiac tumors from metastatic tumors, as the treatments differ significantly. Multimodality imaging comprising TEE, CCT, and cMRI is extremely valuable in establishing the diagnosis. A histological study is confirmatory.
Disclosure
The authors declared no conflicts of interest. The patient gave verbal consent.
references
- 1. Zaher MF, Bajaj S, Habib M, Doss E, Habib M, Bikkina M, et al. A giant left atrial myxoma. Case Rep Med 2014;2014:819052.
- 2. Johansson L. Histogenesis of cardiac myxomas. An immunohistochemical study of 19 cases, including one with glandular structures, and review of the literature. Arch Pathol Lab Med 1989 Jul;113(7):735-741.
- 3. Makhija N, Irpachi K, Chowdhury UK, Kiran U. Unusual attachment of left atrial myxoma: role of transesophageal echocardiography. J Perioper Echocardiogr 2016;4(1):30-33.
- 4. Scheffel H, Baumueller S, Stolzmann P, Leschka S, Plass A, Alkadhi H, et al. Atrial myxomas and thrombi: comparison of imaging features on CT. AJR Am J Roentgenol 2009 Mar;192(3):639-645.
- 5. Gulati G, Sharma S, Kothari SS, Juneja R, Saxena A, Talwar KK. Comparison of echo and MRI in the imaging evaluation of intracardiac masses. Cardiovasc Intervent Radiol 2004;27(5):459-469.
- 6. Maleszewski JJ, Larsen BT, Kip NS, Castonguay MC, Edwards WD, Carney JA, et al. PRKAR1A in the development of cardiac myxoma: a study of 110 cases including isolated and syndromic tumors. Am J Surg Pathol 2014 Aug;38(8):1079-1087.
- 7. Alizadehasl A, Rahbar Z. Relationship between breast cancer and cardiac myxoma. Int J Hematol Oncol Stem Cell Res 2021 Apr;15(2):75-76.
- 8. Vaduva P, Espiard S, Jouinot A, Vantyghem MC, Assié G, Catherine CB, et al. Is Carney complex a breast cancer predisposing syndrome? prospective study of 50 women. Endocrine Abstracts 2020;70 OC7.1.