Leiomyoma of the uterus, also called fibroids, are common and the leading cause of hysterectomy. When they are submucous in location, they have the chance to prolapse. Prolapsed myoma can undergo necrosis due to reduced blood supply from the pedicle, and may cause sepsis if they become infected.1 Symptomatically, their presentation is commonly prolonged vaginal bleeding with or without pelvic pain.1 Here, we report a case with a large impacted friable prolapsed myoma to highlight the challenges in the management, factors predicting the success of vaginal myomectomy, and possible interventions to enhance the safety and feasibility in such circumstances.
Case report
A 36-year-old nulliparous widow was admitted with a history of heavy menstrual bleeding and symptoms of anemia. She gave a history of uterine fibroids and heavy prolonged menstrual flow lasting six months. She had a blood transfusion in another hospital four months before this admission for the same reasons. She was otherwise healthy. At presentation, she was pale and tachycardic with normal blood pressure. On abdominal examination, the uterus was palpable corresponding to 16 weeks pregnancy. On vaginal examination, there was a large friable myoma tightly impacted vaginally with inability to visualize or palpate the cervix. Her hemoglobin was 80 g/L and platelets 260 × 106/L with a normal coagulation profile. Pelvic ultrasound showed three intramural fibroids, 3–5 cm in diameter with a vaginal mass details which were difficult to delineate. Magnetic resonance imaging (MRI) showed a large prolapsed vaginal leiomyoma measuring 10 × 11 cm [Figure 1]. The pedicle of the myoma arose from the fundus of the uterine cavity. The cervix was stretched out but appeared grossly normal. Informed consent was obtained for vaginal myomectomy for the prolapsed fibroid and possible hysteroscopic myomectomy for the submucous fibroid. She agreed to a possible hysterectomy only if it was a necessary lifesaving emergency intervention. Her preoperative anemia was corrected.
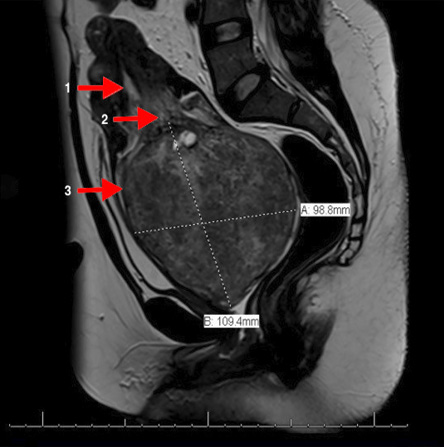
Figure 1: A sagittal view of MRI pelvis showing the (1) endometrial cavity, (2) the pedicle of the prolapsed fibroid, and the (3) prolapsed fibroid in the vagina.
The surgical procedure was performed under general anesthesia. The introitus and vagina were found to be narrow with the large friable fibroid impacted. The hysteroscopic approach was attempted to bypass the fibroid to its pedicle for devascularization. The attempt was unsuccessful as there was no space to pass a 5 mm scope between the myoma and the vaginal wall. Another attempt to devascularize the myoma by encircling the pedicle with a pre-made loop was unsuccessful as the commercially available loop was smaller in diameter than the fibroid. Then the surgeon improvised using a ligating loop, Surgitie™ (Covidien, Norwalk, Connecticut, USA), but was not able to pass it around the fibroid. Then the loop was threaded in two small pieces of pediatric suction catheter to aid insertion around the fibroid, but the attempts were unsuccessful. The Kiwi OmniCup Vacuum Delivery System™ (Clinical Innovations Inc, Murray, Utah, USA) was applied to the fibroid to twist the fibroid around its pedicle, but the fibroid was so impacted it did not rotate.
The decision was taken to proceed with what was avoided initially to morcellate the fibroid with an intact pedicle. As the friable fibroid was manually morcellated in rapid sequence, it started bleeding. Laparotomy or laparoscopy was not a good option as the fibroid was completely vaginal. Ultimately, the fibroid was excised completely as a piecemeal then the pedicle was ligated when it was reached at the end. Hemostasis was secured.
Estimated blood loss was 1L. She had an uneventful recovery. Histopathology report confirmed a degenerated leiomyoma weighing 488 g.
Discussion
Leiomyoma is a common uterine pathology, and it is the leading cause of hysterectomy in premenopausal women.1,2 Leiomyoma can be subserous, intramural, or submucous. Of all the myomas, 5% are submucous, of which 1.3%–2.5% are pedunculated and have the chance of prolapse.3 The degree of prolapse outside the uterine cavity is variable. It might be partially prolapsed in the cervix, completely in the vagina, or outside the vagina and the introitus.3,4 Most prolapsed myomas are small but variable in size, between 1–6 cm in diameter.5 There are case reports in the literature of large prolapse myomas of more than 10 cm in diameter.4–6 The standard management of prolapsed submucous myoma is vaginal myomectomy, which is a minimally invasive procedure, or hysterectomy.5–9 An emergency hysterectomy might be required for continuous severe bleeding, technical difficulty in removing the fibroid, or associated sepsis.4,6
The process of removing a pedunculated myoma requires three steps: devascularization, detachment, and removal.6 In our experience, the mobility of the myoma within the vagina is a crucial factor in the success of surgical management. That mobility is determined by the size of the myoma, the length and thickness of its pedicle, and the vaginal laxity. The ability of the surgeon to reach the pedicle cephalad to the myoma is required for devascularization.5 Applying a ligature or a clamp around the pedicle will devascularize the myoma.10 However, there are rare cases, like ours, where those methods are not successful when applied and result in hysterectomy.11 Our patient never had a vaginal delivery and was not sexually active. These factors contributed to reduced vaginal laxity and hence impaction of the myoma. When myoma impaction is recognized preoperatively, uterine artery embolization is an option to devascularize the myoma and then decrease the intraoperative blood loss during morcellation.4 Another technique to decrease intraoperative blood loss is temporary occlusion of the uterine arteries which can be achieved vaginally or laparoscopically.12,13 The vaginal approach was initially described in 2004 as a non-incisional approach alternative to myomectomy where the uterine arteries are occluded under doppler-ultrasound guidance under general or regional anesthesia then the occluding band is removed after variable time intervals ranging from minutes to hours.12,14 The laparoscopic uterine artery occlusion was described intraoperatively before laparoscopic myomectomy or hysterectomy to decrease blood loss.15 The occlusion of the uterine vessels in myomectomies are either temporary where the occluding suture or clip is removed at the end of the procedure,16 or permanent where the vessel is transected electrosurgically or the occluding vessel and suture are not removed.15,16 There are controversies about the use of permanent occlusion of the uterine arteries in women wanting to preserve fertility due to uncertainty of the consequences of the of ischemic changes on the uterus.15–17 The vaginal approach was not applicable to our case as it was an impacted prolapsed myoma with no access to the uterine arteries through the vaginal fornices. In our practice, we do not perform permanent uterine artery occlusion (laparoscopically or otherwise) on women wanting to preserve fertility in compliance with international guidelines.17 The temporary occlusion requires the use of laparoscopic removable vascular clamps or clips that were not available in our hospital at that time. Intra-myoma injection of diluted vasopressin is another method to decrease intraoperative blood loss.18 However, in our case and from previous experience, vasoconstriction within the myoma is not effective when the myoma is degenerative and friable.
In general, the degree of myoma impaction vaginally is difficult to assess preoperatively. Gonadotropin (GnRH) agonist has historically been considered the most effective presurgical therapy for symptomatic leiomyoma by decreasing their size and vascularization.19 However, usually, their use is not applicable for such large prolapsed myomas for two reasons. An average of two to three months is required for an optimal effect of those medications on the size and the vascularity of the myoma.19 A time interval that is not affordable in the majority of these cases as they usually present to the emergency department with heavy vaginal bleeding requiring an early—if not urgent—intervention.3 The second reason is that most of these prolapsed myomas have undergone a significant degeneration renders the GnRH analogs ineffective.
In most cases of large prolapsed fibroids, hysterectomy is a common planned intervention especially if it is a large myoma, and the patient has completed her family and is willing to lose her uterus.5,6 Hysterectomy can also be performed as an emergency lifesaving measure if associated with severe hemorrhage or sepsis (with or without uterine inversion), or if myomectomy failed.20–22 Our patient wanted to preserve her uterus, and hysterectomy was not acceptable to her unless it was required as an emergency procedure. Intraoperatively, the ligature around the pedicle is achieved by passing a tie or a pre-made loop manually around the fibroid up to the most reachable part of the pedicle.10 Hysteroscopic devascularization is also an option if the scope can be passed beyond the myoma traveling cephalad, and if the cervix provides enough seal for cavity distention medium.23 Another standard method for devascularization and detachment of a prolapsed submucous myoma is devascularization by torsion.7,8 That is achieved by manually rotating the myoma axially around its pedicle.7,8 Challenges to this technique are a slippery myoma to hold by hand, friable to grasp by an instrument, and resistant to rotation due to a thick pedicle or impaction.4,6 In our case, the myoma was as big as a term fetal head, we attempted a Kiwi cup application, which maintained a good suction seal to rotate, but the myoma was so impacted and twisting failed. At this point, a hysterectomy might be safer. However, morcellation of the myoma with intact pedicle was attempted as our patient wanted to avoid hysterectomy. Infiltrating the myoma with vasopressin might help to decrease the blood loss.11 When morcellation without prior devascularization is attempted, time is of the essence to minimize blood loss. This should only be attempted by an experienced gynecologic surgeon.
To our knowledge, unlike other types of myomectomies, there is no data on the use of blood salvage in vaginal myomectomy as a means to minimize intraoperative blood loss by retransfusion of the lost blood back to the patient. Most surgeons avoid the use of blood salvage in vaginal procedures due to concerns of urogenital contamination.
In such large myomas, histopathological evaluation is important to exclude sarcomas that may mimic a benign leiomyoma in clinical behavior and macroscopic features.24,25
Conclusion
Vaginal myomectomy is a standard minimally invasive procedure for prolapsed myoma. The literature on vaginal myomectomy puts a strong emphasis on the size of the myoma as a predictor of the success of vaginal myomectomies. Although there is no specific threshold myoma size, the gynecologic surgeons know that as the size of the myoma increases so does the anticipated surgical difficulties. In our opinion, the other two factors that are frequently ignored; the mobility of the myoma in the vagina and the ability of the surgeon to pass a finger around the prolapsed myoma are good predictors of a successful vaginal approach. So the success of vaginal myomectomy depends not only on the size of the myoma but also on the vaginal laxity. When prolapsed uterine myoma is impacted, it is likely to require combined pre- and intraoperative preparations available to the surgeon’s armamentarium to make the procedure safe and feasible.
Disclosure
The authors declared no conflicts of interest.
references
- Cramer SF, Patel A. The frequency of uterine leiomyomas. Am J Clin Pathol 1990 Oct;94(4):435-438.
- 2. Baird DD, Dunson DB, Hill MC, Cousins D, Schectman JM. High cumulative incidence of uterine leiomyoma in black and white women: ultrasound evidence. Am J Obstet Gynecol 2003 Jan;188(1):100-107.
- 3. Ben-Baruch G, Schiff E, Menashe Y, Menczer J. Immediate and late outcome of vaginal myomectomy for prolapsed pedunculated submucous myoma. Obstet Gynecol 1988 Dec;72(6):858-861.
- 4. Serradilla LN, Gomez-Rios MA, Nicolas C, Ramon y Cajal L. Embolization before surgery of a large pedunculated submucosal myoma prolapsed into the vagina. Acta obstetricia et gynecologica Scandinavica. United States; 2011. p. 554-555.
- 5. Brito LG, Magnani PS, de Azevedo Trapp AE, Sabino-de-Freitas MM. Giant prolapsed submucous leiomyoma: a surgical challenge for gynecologists. Clin Exp Obstet Gynecol 2011;38(3):299-300.
- 6. Golan A, Zachalka N, Lurie S, Sagiv R, Glezerman M. Vaginal removal of prolapsed pedunculated submucous myoma: a short, simple, and definitive procedure with minimal morbidity. Arch Gynecol Obstet 2005 Jan;271(1):11-13.
- 7. Brooks GG, Stage AH. The surgical management of prolapsed pedunculated submucous leiomyomas. Surg Gynecol Obstet 1975 Sep;141(3):397-398.
- 8. Plotti G, Plotti F, Di Giovanni A, Battaglia F, Nagar G. Feasibility and safety of vaginal myomectomy: a prospective pilot study. J Minim Invasive Gynecol 2008 Mar-Apr;15(2):166-171.
- 9. Caglar GS, Tasci Y, Kayikcioglu F. Management of prolapsed pedunculated myomas. Int J Gynaecol Obstet 2005 May;89(2):146-147.
- 10. Ujihira T, Ota T, Nagano H, Ogishima D. Endoloop ligation technique for prolapsed pedunculated submucous uterine myoma: utility and reliability. Arch Gynecol Obstet 2013 Apr;287(4):697-701.
- 11. Zielina P, Schreier R. [Acute hysterectomy for huge submucous leiomyoma prolaps]. Ceska Gynekol 2009 Oct;74(5):389-392.
- 12. Dickner SK, Cooper JM, Diaz D. A nonincisional, Doppler-guided transvaginal approach to uterine artery identification and control of uterine perfusion. J Am Assoc Gynecol Laparosc 2004 Feb;11(1):55-58.
- 13. Vilos GA, Vilos EC, Abu-Rafea B, Hollett-Caines J, Romano W. Transvaginal Doppler-guided uterine artery occlusion for the treatment of symptomatic fibroids: summary results from two pilot studies. J Obstet Gynaecol Can 2010 Feb;32(2):149-154.
- 14. Patel A, Malik M, Britten J, Cox J, Catherino WH. Alternative therapies in management of leiomyomas. Fertil Steril 2014 Sep;102(3):649-655.
- 15. Yang W, Cheng Z, Yu J, Yang H, Liu Z, Ren Q, et al. Multicentre study to evaluate the clinical effects of laparoscopic uterine artery occlusion in combination with myomectomy to treat symptomatic uterine leiomyomas. Eur J Obstet Gynecol Reprod Biol 2016 Sep;204:9-15.
- 16. Dubuisson J, Ramyead L, Streuli I. The role of preventive uterine artery occlusion during laparoscopic myomectomy: a review of the literature. Arch Gynecol Obstet 2015 Apr;291(4):737-743.
- 17. Society of Obstetricians and Gynaecologists of Canada. SOGC clinical practice guidelines. Uterine fibroid embolization (UFE). Number 150, October 2004. Int J Gynaecol Obstet 2005 Jun;89(3):305-318.
- 18. Faivre E, Surroca MM, Deffieux X, Pages F, Gervaise A, Fernandez H. Vaginal myomectomy: literature review. J Minim Invasive Gynecol 2010 Mar-Apr;17(2):154-160.
- 19. Lewis TD, Malik M, Britten J, San Pablo AM, Catherino WH. A Comprehensive review of the pharmacologic management of uterine leiomyoma. Biomed Res Int 2018 Jan;2018:2414609.
- 20. da Silva BB, da Silva-Sampaio JP, Lopes-Costa PV. Huge prolapsed pedunculated necrotizing submucosal leiomyoma. J Minim Invasive Gynecol 2018 Nov - Dec;25(7):1128-1129.
- 21. Pieh-Holder KL, Bell H, Hall T, DeVente JE. Postpartum prolapsed leiomyoma with uterine inversion managed by vaginal hysterectomy. Case Rep Obstet Gynecol 2014;2014:435101.
- 22. Newton BW, Harmanli O. Perplexing presentation of uterine prolapse and a prolapsed pedunculated leiomyoma. Am J Obstet Gynecol 2016 Dec;215(6):799.e1-799.e2.
- 23. Cravello L, Stolla V, Bretelle F, Roger V, Blanc B. Hysteroscopic resection of endometrial polyps: a study of 195 cases. Eur J Obstet Gynecol Reprod Biol 2000 Dec;93(2):131-134.
- 24. Chien JC, Hsieh SC, Lee RC, Chen CY, Cheng CJ, Chan WP. Endometrial stromal sarcoma mimicking submucosal myoma protruding to the vagina: MRI findings. Eur J Gynaecol Oncol 2005;26(6):657-660.
- 25. McCluggage WG, Alderdice JM, Walsh MY. Polypoid uterine lesions mimicking endometrial stromal sarcoma. J Clin Pathol 1999 Jul;52(7):543-546.