An eight-year-old girl presented with a history of fever, nonbilious vomiting, and abdominal pain lasting three days. She was referred from a peripheral hospital for suspected acute appendicitis and admitted to the pediatric emergency department. She had difficulty breathing and pain in the left side of the chest referred to the back. On examination, her vitals were stable with oxygen saturation of 92% in room air. Abdominal examination revealed diffuse tenderness without guarding or rebound tenderness. Chest auscultation showed reduced breath sounds on left-sided posterior lung fields. She was subjected to an erect chest X-ray [Figure 1] and abdominal ultrasound.
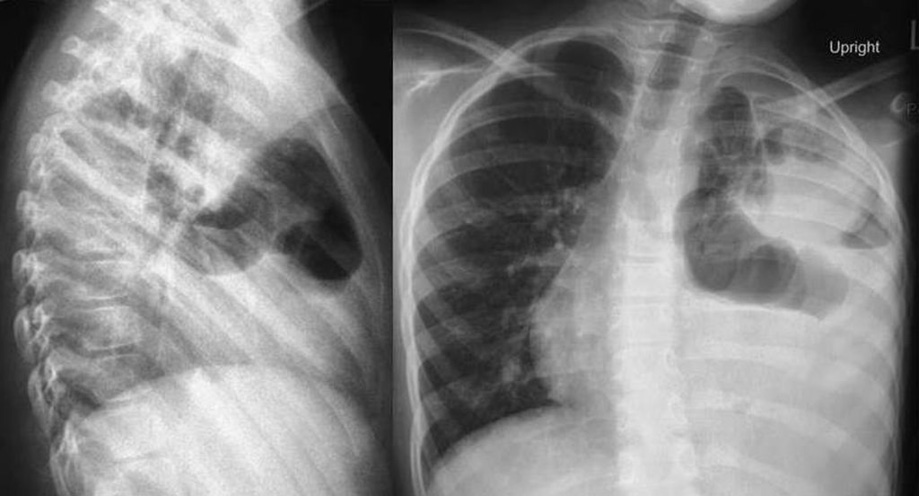
Figure 1: Erect chest X-ray of an eight-year-old girl (posterioranterior and lateral views) showing loops of intestine in the left hemithorax along with a mediastinal shift to the right.
Question
- What is the diagnosis?
a. Pneumonia with pneumatocele.
b. Cavitary pulmonary tuberculosis.
c. Pulmonary hydatid cyst.
d. Lung abscess.
e. Congenital diaphragmatic hernia.
Answer
e. Congenital diaphragmatic hernia.
Discussion
Congenital diaphragmatic hernia (CDH) is a developmental defect of the diaphragm most commonly presenting with severe respiratory compromise in the neonatal period. The condition is observed in one in 2500 live births due to failure of the fusion of pleuroperitoneal folds at six to eight weeks gestation leading to herniation of abdominal contents into the hemithorax.1 A posterolateral Bochdalek hernia is the most common form of CDH, which is more common on the left side (75–80%). Forty percent of cases have additional anomalies most commonly involving the ribs, vertebra, and heart.1 CDH may be a feature of genetic conditions such as Fryns syndrome, Simpson-Golabi-Behmel syndrome, and Cornelia de Lange syndrome. Up to 60% of CDH cases are diagnosed by antenatal ultrasound, and the rest are suspected postnatally based on clinical presentation with symptoms usually appearing a few hours after birth and confirmed radiologically. However, late presentation of CDH due to delayed herniation of the abdominal contents through the defect may occur beyond the neonatal period in as many as 25% of cases.2,3
Late-presenting CDH is associated with a wide range of non-specific clinical symptoms.2–4 Dyspnea and vomiting were the most frequent symptoms reported in patients with either chronic or acute manifestations. Right-sided hernias are associated with respiratory symptoms that occur more often in younger age-groups whereas left-sided defects tend to have gastrointestinal symptoms among older patients. In a review of 362 cases of late-presenting CDH, 80% had left posterolateral hernia with associated anomalies in 8%.2 Chronic symptoms were more common with a right-sided hernia. Complications resulting from diaphragmatic hernia were noted in 12.4% and a further 3% of children had iatrogenic complications due to misdiagnosis. Preoperative and postoperative mortality were 4% and 2%, respectively. Postoperative complications were observed in 3.6% of children requiring further surgical intervention.2
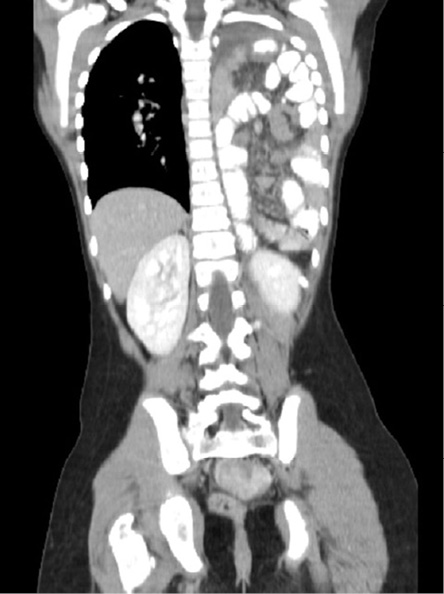
Figure 2: Computed tomography of the abdomen (coronal view) showing left posterolateral diaphragmatic hernia of Bochdalek type.
Radiological findings in late presentation of CDH are highly variable and pose a significant diagnostic problem. The radiographic appearance may mimic congenital lung malformations, lung cysts, necrotizing pneumonia, pneumatoceles, severe acute asthma, and pneumothorax.3 Normal chest X-rays only add to the diagnostic dilemma in this condition. The normal radiographic appearance might be explained by the anatomical location of the spleen, which may act as a plug covering the defect.5 A loop of intestine in the hemithorax is often misinterpreted as pneumothorax leading to needle aspiration or chest drain insertion.6 It has been suggested that nasogastric tube placement could double as an early diagnostic or therapeutic intervention when the diagnosis is suspected and gastrointestical contrast studies are useful in diagnostic work-up. The possibility of ‘acquired’ CDH in the setting of extreme aerophagia or mild abdominal trauma should be considered.7
Ultrasound is a useful diagnostic tool for visualizing diaphragmatic continuity and herniated organs, and may reveal associated intra-abdominal defects. Computed tomography (CT) scan is most effective in showing the herniated intestines and associated complications such as strangulation. Multislice CT scan with coronal and sagittal reformatted images is the most effective and useful imaging technique [Figure 2]. With high sensitivity for soft tissue, magnetic resonance imaging may be performed in selected conditions wherein the diagnosis remains doubtful.8
Conclusion
The late-presenting CDH presents a considerable diagnostic challenge to clinicians. Radiologic findings in these cases may be particularly difficult to interpret and may result in diagnostic delay, misguided therapy, and even fatal outcomes.
references
- 1. Keller RL, Guevara-Gallardo S, Farmer DL. Surgical disorders of the chest and airways. In: Gleason CA, Devaskar SU, editors. Avery’s diseases of the newborn. 9th ed Elsevier Saunders; 2012. p. 672-697.
- 2. Bagłaj M. Late-presenting congenital diaphragmatic hernia in children: a clinical spectrum. Pediatr Surg Int
2004 Sep;20(9):658-669.
- 3. Berman L, Stringer D, Ein SH, Shandling B. The late-presenting pediatric Bochdalek hernia: a 20-year review. J Pediatr Surg 1988 Aug;23(8):735-739.
- 4. Singer JI. Herniation of abdominal contents simulating status asthmaticus. Pediatr Emerg Care 1987 Dec;3(4):
250-252.
- 5. Glasson MJ, Barter W, Cohen DH, Bowdler JD. Congenital left posterolateral diaphragmatic hernia with previously normal chest x-ray. Pediatr Radiol 1975 Sep;3(4):201-205.
- 6. Coren ME, Rosenthal M, Bush A. Congenital diaphragmatic hernia misdiagnosed as tension pneumothorax. Pediatr Pulmonol 1997 Aug;24(2):119-121.
- 7. Fein JA, Loiselle J, Eberlein S, Wiley JF, Bell LM. Diaphragmatic hernia masquerading as pneumothorax in two toddlers. Ann Emerg Med 1993 Jul;22(7):1221-1224.
- 8. Eren S, Ciriş F. Diaphragmatic hernia: diagnostic approaches with review of the literature. Eur J Radiol 2005 Jun;54(3):448-459.