Cancer is one of the most important preventable causes of mortality and morbidity worldwide. Based on new data, alarming trends in cancer incidence rates have been reported in both developed and developing countries in recent years and, especially in developing countries, is predicted to increase by 45% in 2025.1 Moreover, it is estimated that the global economic and healthcare burden of cancer will increase as much as 70% within the next two decades.2
Despite being potentially among the most preventable and treatable chronic diseases, cancer is the second leading cause of death globally and is expected to account for 13.1 million deaths per year by 2030. Approximately 70% of these cancer-related deaths are predicted to occur in developing countries.3
Due to the growing healthcare burden of cancer in developing countries, it is important to assess the incidence of cancer patterns. As in most developing countries, there has been considerable population growth in Turkey. Life expectancy has increased, and the socioeconomic and demographic situation has also changed.1,3–5
In Turkey, the lack of population-based national cancer prevention and screening programs, and low cancer awareness remains an important problem. Definitive information about the patient including location and time characteristic of cancer is required to provide more accurate and efficient cancer control planning and program implementation. The number of researchers investigating the recent changes and incidence of common cancers in Turkey is limited. Both incidence and time-trend analysis are important in determining the cancer pattern. Therefore, this study aimed to evaluate the trends in age-standardized incidence rates of cancer incidence by gender and age, and common types of cancers in the Sivas province, Turkey, between 2004 and 2014.
Methods
The study population composed of all patients diagnosed with cancer in Sivas, a Middle Anatolian province, from 2004 to 2014. This retrospective study was carried out on data derived from the Sivas Public Health Department Cancer Unit and Cumhuriyet University Hospital Cancer Record Unit. After data entry, all duplicates were removed. Then, information related to characteristics, including age, gender, and cancer type were reorganized. To estimate the incidence rate, those with secondary tumors and whose residence in Sivas was less than six months were excluded.
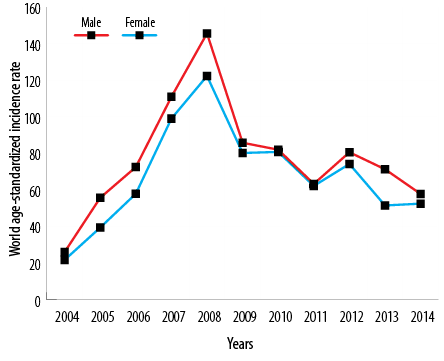
Figure 1: Trend of world age-standardized incidence rate of all cancer cases by gender from 2004 to 2014 in Sivas, Turkey.
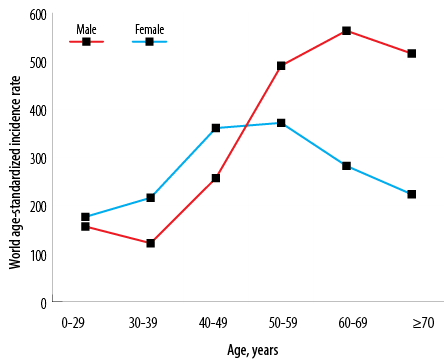
Figure 2: World age-standardized incidence rate of all cancer cases by gender and age groups in Sivas, Turkey, from 2004 to 2014.
Cancer cases were divided into the following 19 types: lung, laryngeal, central nervous system and brain, skin, bone, testis, prostate, gynecological (cervix, endometrium, and ovary), stomach, colorectal, leukemia, lymphoma, breast, liver, bladder, thyroid, and urinary. World age-standardized incidence rates (ASR-W), which were obtained using the world standard population, were calculated for each of the six age groups (0–29, 30–39, 40–49, 50–59, 60–69 and ≥ 70) by gender.6
Data analysis was performed using SPSS Statistics (IBM Corp. Released 2013. IBM SPSS Statistics for Windows, Version 22.0. Armonk, NY: IBM Corp) based on age-standardized incidence rates in both genders. Age-standardized incidence rates were also directly calculated according to the world standard population. Descriptive statistics and linear regression analysis were performed to determine the trends in age-standardized incidence rates of cancer incidence. The significance level was considered as p < 0.050.
Table 1: World age-standardized incidence rate for all cancer cases by gender in Sivas, Turkey, from 2004 to 2014.
|
2004 |
26.0 |
21.7 |
1.2 |
|
2005 |
55.7 |
39.4 |
1.4 |
|
2006 |
72.5 |
57.9 |
1.3 |
|
2007 |
110.9 |
99.0 |
1.1 |
|
2008 |
145.6 |
122.3 |
1.2 |
|
2009 |
85.8 |
80.2 |
1.1 |
|
2010 |
82.0 |
80.8 |
1.0 |
|
2011 |
63.3 |
62.2 |
1.0 |
|
2012 |
80.6 |
74.2 |
1.0 |
|
2013 |
71.3 |
51.5 |
1.4 |
|
2014 |
57.8 |
52.5 |
1.1 |
Table 2: World age-standardized incidence rate for all cancer cases by gender and age in Sivas, Turkey.
|
0–29 |
156.4 |
176.3 |
0.9 |
|
30–39 |
121.7 |
216.0 |
0.6 |
|
40–49 |
256.8 |
360.8 |
0.7 |
|
50–59 |
490.4 |
371.6 |
1.3 |
|
60–69 |
563.0 |
282.2 |
2.0 |
Results
A total of 13 377 patients were diagnosed with cancer, 7606 (56.9%) males and 5771 (43.1%) females with a mean age of 57.1±16.6 (59.5±6.0 years for males and 54.0±8.3 years for females). The total number of cancer cases was 407 in 2004, and that number increased to 969 cases in 2014.
Table 1 and Figure 1 provide the ASR-W for all cancer cases over the 11-year study period for both genders. According to the ASR-W, the gender ratio (male-to-female) for all cancer cases was 1.2. The ASR-W of common cancer in males and females increased more than two-fold. The highest ASR-W for both genders was observed in 2008 (ASR-W = 145.6 for males and 122.3 for females). The overall ASR-W was higher among males than females, and this difference was statistically significant (p < 0.050).
The ASR-W for all cancer types by age groups for both genders is demonstrated in Table 2 and Figure 2. ASR-W was higher among females aged 49 years or younger [Table 2]. While this was not statistically significant (p > 0.050), this rate was significantly higher in male aged 50 years or over (p < 0.050).
The ASR-W was 205.2 in male and 168.0 in female for the time period studied [Table 3]. Prostate cancer (ASR-W = 35.8) was the most common cancer type for males followed by lung (ASR-W = 33.9), colorectal (ASR-W = 19.0), urinary (ASR-W = 18.4), and stomach (ASR-W = 17.3). Thyroid (ASR-W = 37.5) was the most common type of cancer for females followed by breast (ASR-W = 27.7), colorectal (ASR-W = 11.7), lymphoma (ASR-W = 10.4), and stomach (ASR-W = 10.0).
Our study showed that ASR-W of the most commonly diagnosed cancers differs by gender and age. In males, the ASR-W increased with increasing age and reached a peak among those aged 60–69 years. Among females, we saw a sharp decrease in the ASR-W of thyroid and lymphoma cancers in those aged 30–39 years. This rate was sharply increased for thyroid and breast cancer in the 40–49 age group.
Table 3: World age-standardized incidence rate for different cancer types by gender in Sivas, Turkey, from 2004 to 2014.
|
Lung |
33.9 |
9.8 |
|
Laryngeal |
16.0 |
6.1 |
|
CNS and brain |
9.8 |
9.2 |
|
Skin |
11.4 |
9.8 |
|
Bone |
1.3 |
0.7 |
|
Testis |
3.4 |
- |
|
Prostate |
35.8 |
- |
|
Endometrium |
- |
5.5 |
|
Cervix |
- |
5.5 |
|
Ovary |
- |
3.5 |
|
Stomach |
17.3 |
10.0 |
|
Colorectal |
19.0 |
11.7 |
|
Leukemia |
13.9 |
7.3 |
|
Lymphoma |
10.9 |
10.4 |
|
Breast |
0.0 |
27.7 |
|
Bladder |
3.6 |
4.4 |
|
Liver |
2.3 |
1.1 |
|
Thyroid |
8.2 |
37.5 |
|
Urinary |
18.4 |
7.6 |
CNS: central nervous system.
Discussion
We investigate the incidence and trend of common cancers in the Sivas province by gender from 2004 to 2014. Over the 11-year study period, cancer cases exhibit some interesting incidence and trends. First, all cancer cases that showed a sharp increase in 2008 among both females and males tended to decrease after 2008. Secondly, data analysis showed an interesting pattern regarding a few cancer types in our study. Prostate and thyroid cancers were the most common cancers in males and females, respectively. The second most common cancers were lung cancer in males and breast cancer in females, while stomach, colorectal, urinary (only in male), and lymphoma (only in females) were the only cancers that were ranked in the top five most incident cancers for the study period.
Our study findings show that the proportion of common cancer cases in males was higher than in females (56.9% vs. 43.1%). These findings were similar to the results from Europe, where the incidence of various cancers was higher in males than females (57% vs. 43%).7
An increased peak in cancer cases was observed in both sexes in 2008, which can be attributed to the improvement in the cancer registry system in the country and the increase in access to health services in the same year.8 The improvement in the registry system in Sivas province also accounts for the sharp increases in the incidence rates of cancer during the study period, especially in 2008. Conclusively, cancer was most frequently diagnosed in both genders in 2008.
According to the World Health Organization, estimations of cancer incidence rates will almost double by 2030, and most rises (75%) are predicted to occur in non-developed countries.9 As indicated by the Ministry of Health Department of Cancer Control database in Turkey, cancer incidence rates increased from 133.78 per 105 in 2002 to 173.85 per 105 in 2005. Also, the age-adjusted cancer rates for males and females in 2012 were reported as 277.7 per 105 and 188.2 per 105, respectively.10 Similar to these reports, a serious increase in the cancer incidence rate was observed in this study. The value of ASR-W in our study was 205.2 per 105 for males and 168.0 per 105 for females, which was lower than the value of ASR-W in Turkey and in central and eastern Europe (260.0 in males and 193.5 in females per 105), but higher than the value of ASR-W in Western Asia (192.8 in males and 150.2 in females), yet similar to the world value.11 The increased ASR-W in males and females between 2004 and 2014 may be explained as the result of changes in environmental factors (e.g., electromagnetic waves, radiation, chemicals, compounds in cosmetics, insecticides and pesticides, food additives, pharmaceutical drugs) and changes in lifestyle, including increasing consumption of fatty foods and fast foods, tobacco smoking, sedentary lifestyle as well as rapidly growing elderly population.12,13 All of these lifestyle changes have been repeatedly shown to increase the incidence of cancer.14–17
Unlike previous reports in which the most common type of cancer in Turkey was lung cancer in males (60.4 per 105) and breast cancer in females (46.8 per 105),18,19 we found prostate and thyroid cancer ranked first both in males and females, respectively. This difference might be due to the different time, geographical population shifts, or the improvement in the cancer registry system.8
Our study indicated that thyroid cancer was the first most common cancer in females. This high incidence of thyroid cancer in females (ASR-W = 37.5) compared to males (ASR-W = 8.2) requires further investigations to determine whether these findings were the result of the greater use of diagnostic imaging, leading to more frequent detection of smaller, asymptomatic tumors,20 since radiation exposure of the thyroid gland (especially during childhood and adolescence) is recognized as a risk factor for the development of thyroid cancer.21 In recent years, various studies have shown that there has been a significant increase in the incidence of thyroid cancer. A recent study from Cyprus reported a higher rate for thyroid cancer in females and showed that the incidence has doubled in just one decade.22 A similar pattern of increase has also been reported in western European countries.23
Similar to the incidence rate in developed countries, prostate cancer is the first most common cancer among males in our study while being the second most common cancer worldwide and in Turkey.24 This evidence suggests an increase in the incidence of prostate cancer in developing countries in the future.25 Although the main cause of this cancer (and similarly of other types of cancer) is yet unknown,26 there are various effective factors associated with the development and progression of prostate cancer. For example, occupational or environmental risk factors, smoking, nutrition, lifestyle, and demographic factors, including older age, socioeconomic situation, and genetic susceptibility are the most responsible risk factors in prostate cancer.27,28 However, the effects of western lifestyle and behavior, as well as genetic predisposition, on the incidence of prostate cancer and their relationship with macroeconomic determinants should be cautiously interpreted.
Conclusion
The cancer incidence rate among males has remained higher than females from 2004 to 2014 in the Sivas province, Turkey, and an increasing trend of incidences of various cancers was observed in both genders. Compared to previous studies, the differences in the most common type of cancer in both genders and cancer incidence rates in this study can be due to the changes in the environment, lifestyle, and the aging population. It is necessary to raise public awareness about the risk factors and develop appropriate and effective screening programs to provide more reliable data for prevention and control programs in Sivas province.
Disclosure
The authors declared no conflicts of interest. No funding was received for this study.
references
- 1. Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin 2005 Mar-Apr;55(2):74-108.
- 2. Stewart BW, Wild CP. World Cancer Report. Lyon, France: IARC; 2014.
- 3. Colditz GA, Sellers TA, Trapido E. Epidemiology - identifying the causes and preventability of cancer? Nat Rev Cancer 2006 Jan;6(1):75-83.
- 4. Yüceşahin MM. KC, S. Demographic and human capital heterogeneity in selected provinces in Turkey: A scenario analysis using multi-dimensional population projection model. Econ Sociol 2015;8(3):215-244.
- 5. Jemal A, Center MM, DeSantis C, Ward EM. Global patterns of cancer incidence and mortality rates and trends. Cancer Epidemiol Biomarkers Prev 2010 Aug;19(8):1893-1907.
- 6. Ahmad OB, Boschi-Pinto C, Lopez AD, Murray CJ, Lozano R, Inoue M. Age standardization of rates: a new WHO standard. Geneva: World Health Organization; 2001.
- 7. World Health Statistics. 2014. Genova, Switzerland: World Health Organization; 2014.
- 8. Health Ministry of Turkey. Turkey oncology services reconstruction program 2010-2023. [cited 2017 Jun 10]. Available from: https://www.kanser.org/saglik/userfiles/file/11Mayis2011/turkiye_onkoloji_hizmetleri_kitapcik.pdf (in Turkish).
- 9. World Health Organization. Cancer. [cited 2017 Jun 10]. Available from: http://www.who.int/topics/cancer/en/.
- 10. Health Ministry of Turkey Cancer control programme. [cited 2017 Jun 10]. Available from: https://www.iccp-portal.org/system/files/plans/Turkiye_Kanser_Kontrol_Program_English.pdf.
- 11. International Agency for Research on Cancer. [cited 2017 Jun 10]. Available from: http://www. http://gco.iarc.fr/Pages/pie_pop_sel.aspx.
- 12. Belpomme D, Irigaray P, Sasco AJ, Newby JA, Howard V, Clapp R, et al. The growing incidence of cancer: role of lifestyle and screening detection (Review). (Review). Int J Oncol 2007 May;30(5):1037-1049.
- 13. Keyghobadi N, Rafiemanesh H, Mohammadian-Hafshejani A, Enayatrad M, Salehiniya H. Epidemiology and trend of cancers in the province of Kerman: southeast of Iran. Asian Pac J Cancer Prev 2015;16(4):1409-1413.
- 14. Curry SJ, Byers T, Hewitt M, eds. Fulfilling the potential of cancer prevention and early detection. Washington, DC: National Academy Press; 2003.
- 15. Province MA, Hadley EC, Hornbrook MC, Lipsitz LA, Miller JP, Mulrow CD, et al. The effects of exercise on falls in elderly patients. A preplanned meta-analysis of the FICSIT Trials. Frailty and Injuries: Cooperative Studies of Intervention Techniques. JAMA 1995 May;273(17):1341-1347.
- 16. Campbell KL, McTiernan A. Exercise and biomarkers for cancer prevention studies. J Nutr 2007 Jan;137(1)(Suppl):161S-169S.
- 17. Friedenreich CM, Courneya KS, Bryant HE. Case-control study of anthropometric measures and breast cancer risk. Int J Cancer 2002 May;99(3):445-452.
- 18. Özmen V. Breast cancer in Turkey: clinical and histopathological characteristics (analysis of 13.240 patients). J Breast Health 2014 Apr;10(2):98-105.
- 19. Fidaner C, Eser SY, Parkin DM. Incidence in Izmir in 1993-1994: first results from Izmir Cancer Registry. Eur J Cancer 2001 Jan;37(1):83-92.
- 20. Siegel R, Naishadham D, Jemal A. Cancer statistics, 2012. CA Cancer J Clin 2012 Jan-Feb;62(1):10-29.
- 21. Schneider AB, Ron E, Lubin J, Stovall M, Gierlowski TC. Dose-response relationships for radiation-induced thyroid cancer and thyroid nodules: evidence for the prolonged effects of radiation on the thyroid. J Clin Endocrinol Metab 1993 Aug;77(2):362-369.
- 22. Farazi PA. Cancer trends and risk factors in Cyprus. Ecancermedicalscience 2014 Jan;8:389.
- 23. La Vecchia C, Malvezzi M, Bosetti C, Garavello W, Bertuccio P, Levi F, et al. Thyroid cancer mortality and incidence: a global overview. Int J Cancer 2015 May;136(9):2187-2195.
- 24. Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide burden of cancer in 2008: GLOBOCAN 2008. Int J Cancer 2010 Dec;127(12):2893-2917.
- 25. Baade PD, Youlden DR, Cramb SM, Dunn J, Gardiner RA. Epidemiology of prostate cancer in the Asia-Pacific region. Prostate Int 2013;1(2):47-58.
- 26. Hsing AW, Chokkalingam AP. Prostate cancer epidemiology. Front Biosci 2006 May;11:1388-1413.
- 27. Baade PD, Youlden DR, Krnjacki LJ. International epidemiology of prostate cancer: geographical distribution and secular trends. Mol Nutr Food Res 2009 Feb;53(2):171-184.
- 28. Zhang L, Yang BX, Zhang HT, Wang JG, Wang HL, Zhao XJ. Prostate cancer: an emerging threat to the health of aging men in Asia. Asian J Androl 2011 Jul;13(4):574-578.