|
Abstract
Gastrointestinal ganglioneuromatosis is a rare and benign proliferation of both ganglion and Schwann cells, which may present in a variety of clinicopathological characteristics including polypoid, localized and diffuse forms. It is characterized by the presence of a large number of dysplastic ganglion cells or hyperganglionosis. The affected patients are usually children and a number of them have intestinal neuronal dysplasia type B, which may overlap with ganglioneuromatosis. We report a very rare case of gastric ganglioneuromatosis with hyperganglionosis in a 34 year old male, who presented as a case of gastric outlet obstruction and marked gastric dilatation which was diagnosed both clinically and radiologically as a case of gastric obstruction due to gastric malignancy. Based on these findings and because of the patient’s deteriorating clinical situation; the patient underwent distal gastrectomy and the final diagnosis was made following the histopathological examination of the resected specimen. The clinicopathological features and diagnostic criteria of this rare disorder are described together with a literature review of other similar cases affecting different parts of the gastrointestinal tract.
Keywords: Ganglioneuromatosis; Intestinal neuronal dysplasia; Stomach.
Introduction
Gastrointestinal ganglioneuromatosis is a rare condition characterized by the presence of a significant proliferation of ganglion cells, Schwann cells and nerve fibers in the wall of the stomach or intestine. The disease may affect any part of the gastrointestinal tract but the ileum, gallbladder, colon and appendix are more frequently affected. The disease is very rare in adults and the stomach is an exceptionally rare site. In this report, we describe the clinicopathological features of a unique case of gastric ganglioneuromatosis and neuronal dysplasia in an adult patient who presented with distal gastric stenosis, which led to an initial erroneous diagnosis of gastric malignancy with subsequent distal gastrectomy. The final diagnosis was then reached following histopathological assessment of the partial gastrectomy specimen at King Khalid University Hospital.
Case report
A dehydrated 34 years old Yemeni male presented to the surgical unit at a private hospital in the Riyadh region with upper abdominal pain, nausea, vomiting and a severe sensation of "bloating" and discomfort. The symptoms were present for the last few days but increased in the few hours prior to admission. The patient gave a past medical history of previous laparotomy in Yemen for a bleeding gastric ulcer. The biochemical and hematological profiles of the patient were within normal limits, but he continued to complain of severe abdominal pain and bouts of nausea and vomiting, which persisted despite initial emergency treatment measures. Ultrasound and Barium studies of the upper GI revealed a markedly dilated stomach with thickening of the anterior gastric wall and prominent mucosal folds, (Fig. 1). A diagnosis of gastric outlet obstruction possibly due to adenocarcinoma or lymphoma was made.
However, because of the patient’s deteriorating clinical situation, no confirmatory biopsies could be done and the patient underwent exploratory laparotomy with subsequent partial gastrectomy at the same private hospital. Initial histopathological examination of the resection specimen failed to show evidence of a neoplastic process and the case was referred to King Khalid University Hospital, for review of the histopathological slides and material.

Figure 1: Barium meal studies showing a markedly dilated stomach with prominent mucosal folds.
Histopathological examination of sections from the partial gastrectomy specimen showed large collections of ganglion cells lying in between the hypertrophied muscularis propria. The described ganglion cells were large, had dense eosinophilic cytoplasm with enlarged nuclei and prominent nucleoli. Their numbers varied between 5-15 ganglion cells per one medium to high power microscopic field, and were surrounded by hypertrophied nerve bundles with areas of edema and fibrosis, (Figs. 2A,B).
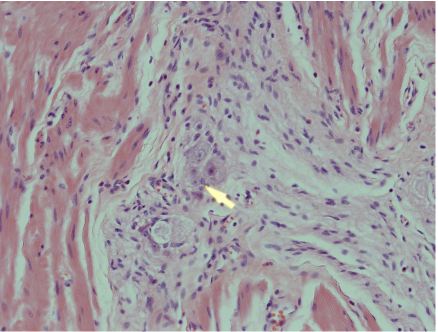
Figure 2A: Gastric ganglioneuromatosis - hyperplastic and enlarged nerve fibers and Schwann cells in intramural myenteric plexus. Hematoxylin and Eosin stain ×200.
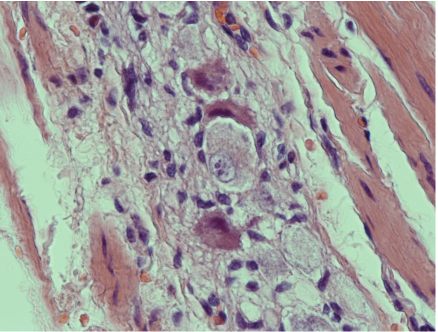
Figures 2B: Gastric ganglioneuromatosis and hypergangliosis due to intestinal neuronal dysplasia type II. Note the presence of abnormal neurons within hyperplastic nerve bundles. Hemotoxylin and Eosin stain × 400.
These findings were confirmed by immunohistochemical stains which included S-100 protein and neurone specific enolase. A final diagnosis of gastric hyperganglionosis (also referred to as neuronal dysplasia type B) and diffuse ganglioneuromatosis was made. This diagnosis was based on the abnormal presence of numerous giant ganglion cells associated with many bundles of hypertrophied nerve fibers and Schwann cells. These changes are usually associated with hypertrophied muscularis propria which may lead (as in this unusual case) to pseudo-obstruction of the gastric outlet mimicking pyloric stenosis secondary to a neoplastic process.
Following surgery, the patient made an uneventful recovery and is currently undergoing further investigations to exclude MEN IIb syndrome (medullary carcinoma of the thyroid, pheochromocytoma, oral mucosal neuromas and skeletal deformities) as well as other conditions which may be associated with intestinal neuronal dysplasia, like aortic stenosis and congenital diaphragmatic hernia.
Discussion
Intestinal neuronal dysplasia is a developmental abnormality which involves the gastroenteric nervous system and usually occurs in two forms: type A - characterized by decreased gastrointestinal sympathetic innervation also known as hypoganglionosis,1 and type B - characterized by increased numbers of ganglion cells and is also known as hyperganglionosis.2,3 Neuronal dysplasia can be diffuse,4,5 and involve both the small and large intestine, or it may remain confined to a single intestinal segment.6 The disease may also involve the oesphagus,7 and gallbladder.8,9 Intestinal ganglioneuromatosis is a rare and benign neoplastic condition characterized by a variety of pathological findings, which include a polypoid form and a diffuse form characterized by hyperplasia of the myenteric plexus which can be associated (as in our case) with neuronal dysplasia type B or hyperganglionosis, and in these cases the changes may be accompanied by multiple endocrine Neoplasia IIB and a mutation in the RET oncogene.10
Histologically, intestinal neuronal dysplasia type B usually show increased numbers of ganglion cells (7 to15 ganglion cells per plexus) with thickened and hypertrophied axons. There is also usually an increase in acetylcholinesterase activity in the mucosal and submucosal nerves.2,3,10
Intestinal ganglioneuromatosis is mainly a disease of young children which overlap with intestinal neuronal dysplasia type B or hyperganglionosis. Some investigators do, however, believe that the two conditions must be clearly differentiated from each other.11
This case report describes the clinicopathological features of an unreported site for ganglioneuromatosis and hyperganglionosis (neuronal dysplasia type II) in an adult patient, which is an unusual age group for this condition. Furthermore, gastric obstruction is an undescribed presentation, which may create (as in this case) a false clinical impression of malignancy. We must emphasize, however, that if malignancy is suspected, a staging computed tomography study together with endoscopy and biopsies should ideally be performed prior to any surgical intervention. In our case, surgery was done because of the described severe gastric obstruction which was most probably caused by a combination of muscular mural hypertrophy and hyperplasia of the myenteric plexus leading to stricture formation.4,6,10
Conclusion
In adult patients presenting with obstructive gastrointestinal symptoms, the rare possibility of ganglioneuromatosis and intestinal neuronal dysplasia should be considered and investigated in order to avoid unnecessary and extensive surgical intervention which may occur because of the assumption of a malignant diagnosis.
Acknowledgements
The authors would like to express their gratitude to Ms. Vivian Darusin for her excellent secretarial skills in typing of this manuscript. The authors reported no conflict of interest and no funding was received for this work.
References
1. Schärli AF, Sossai R. Hypoganglionosis. Semin Pediatr Surg 1998 Aug;7(3):187-191.
2. Kobayashi H, Hirakawa H, Puri P. What are the diagnostic criteria for intestinal neuronal dysplasia? Pediatr Surg Int 1995;10:459 .
3. Meier-Ruge W, Gambazzi F, Käufeler RE, Schmid P, Schmidt CP. The neuropathological diagnosis of neuronal intestinal dysplasia (NID B). Eur J Pediatr Surg 1994 Oct;4(5):267-273.
4. Charagundla SR, Levine MS, Torigian DA, Campbell MS, Furth EE, Rombeau J. Diffuse intestinal ganglioneuromatosis mimicking Crohn’s disease. AJR Am J Roentgenol 2004 May;182(5):1166-1168.
5. Hirata K, Kitahara K, Momosaka Y, Kouho H, Nagata N, Hashimoto H, et al. Diffuse ganglioneuromatosis with plexiform neurofibromas limited to the gastrointestinal tract involving a large segment of small intestine. J Gastroenterol 1996 Apr;31(2):263-267.
6. Lorenceau-Savale C, Savoye G, Pouzoulet J, Le Pessot F, Savoye-Collet C, Leblanc-Louvry I, et al. Ganglioneuromatosis: an unusual cause of ileal stricture mimicking Crohn’s disease. Dig Dis Sci 2007 Aug;52(8):1806-1809.
7. Siderits R, Hanna I, Baig Z, Godyn JJ. Sporadic ganglioneuromatosis of esophagogastric junction in a patient with gastro-esophageal reflux disorder and intestinal metaplasia. World J Gastroenterol 2006 Dec;12(48):7874-7877.
8. Sakuma T, Hirota M, Ohashi H, Kakudo K and Kawano K. Extensive ganglioneuromatosis of gallbladder. International Journal of Surgical Pathology 2008; Electronic publication ahead of print.
9. Chetty R, Clark SP. Cholecystitis, cholelithiasis, and ganglioneuromatosis of the gall bladder: an unusual presentation of MEN type 2b. J Clin Pathol 1993 Nov;46(11):1061-1063.
10. Fenoglio-Freiser CM, Noffsinger AE, Stemmermann GN, Lantz PE, Isaacson P. Gastrointestinal pathology: An Atlas and Text; Third Edition. Philadelphia, PA: Lippincott Williams and Wilkins, 2008: 555-559.
11. Meier-Ruge WA, Ammann K, Bruder E, Holschneider AM, Schärli AF, Schmittenbecher PP, et al. Updated results on intestinal neuronal dysplasia (IND B). Eur J Pediatr Surg 2004 Dec;14(6):384-391.
|