An 11-year-old boy was diagnosed with inflammatory bowel disease (IBD), moderate pancolitis, in January 2021, when he presented with bloody diarrhea with failure to thrive. He received oral prednisolone as induction therapy and continued with mesalazine as maintenance therapy. However, due to frequent disease flare-ups and ongoing disease activity, his therapy was escalated to infliximab infusion (5 mg/kg/dose) at eight-week intervals, which resulted in the resolution of his gastrointestinal symptoms.
Six months after starting infliximab, he developed lower back pain, bilateral thigh pain, and intermittent difficulty bearing weight. He reported no fever, joint swelling, or skin rash, and he remained asymptomatic from a gastrointestinal perspective.
On examination, he appeared small for age with a weight below the 3rd centile and height at the 5th centile. There was tenderness over the lower back, bilateral sacroiliac joints, and groin area with normal hip joint movement. He was unable to bend his back or bear weight on his legs fully.
His blood tests revealed the following results: hemoglobin levels of 10.0 g/dl (reference range: 11.4–14), platelet count of 800 × 109 (150–450 × 109), and white cell count of 12 × 109 (4–12 × 109). The neutrophil count was 7.0× 109 (3.5–8), and the lymphocyte count was 3.0 × 109 (3–9). The albumin levels were 43 g/L (38–54) with normal transaminases but the C-reactive protein was 51 (< 5) with an ESR of 57 (< 9).
He underwent a whole-body magnetic resonance imaging (MRI) [Figure 1]. Informed consent was obtained from the patient’s parent.
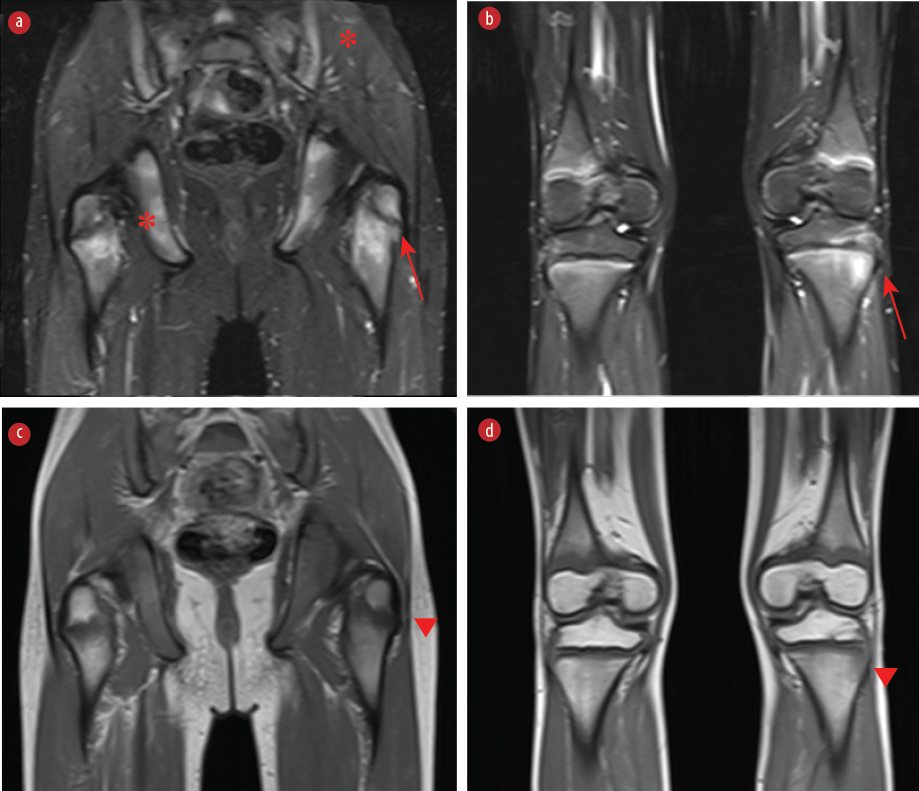 Figure 1: Coronal MRI images of the pelvis/proximal femur, distal femur and proximal tibia. (a, b) Edema is seen in the periphyseal regions of the femur and tibia on short-tau inversion recovery images (red arrows). (a) Asymmetric involvement of the pelvic bones and sacroiliac joints (*) is also present. (c, d) Corresponding low-signal changes are noted on T1-weighted images (arrowheads).
Figure 1: Coronal MRI images of the pelvis/proximal femur, distal femur and proximal tibia. (a, b) Edema is seen in the periphyseal regions of the femur and tibia on short-tau inversion recovery images (red arrows). (a) Asymmetric involvement of the pelvic bones and sacroiliac joints (*) is also present. (c, d) Corresponding low-signal changes are noted on T1-weighted images (arrowheads).
Questions
- What is the most likely diagnosis?
- What are the possible differential diagnoses?
- How would you manage this boy?
Answers
- Chronic recurrent multifocal osteomyelitis (CRMO)
- Infectious osteomyelitis, neoplasms (e.g., leukemia, Ewing sarcoma), Langerhans cell histiocytosis, or other autoimmune/autoinflammatory disorders.
- Effective control of IBD often leads to an improvement in CRMO symptoms. Treatment options may include oral corticosteroids, methotrexate, sulfasalazine, and tumor necrosis factor-α antagonists.
Discussion
CRMO, also known as chronic nonbacterial osteomyelitis, is one of the extraintestinal manifestation of IBD. It is a rare autoinflammatory bone disorder characterized by recurrent, sterile bone inflammation, primarily affecting the clavicles, pelvis, spine, and long bones.1-3
It typically affects children and adolescents, presenting with a relapsing course of insidious bone pain, localized swelling, and tenderness over the affected areas. The exact etiology remains unclear, but it is believed to involve immune dysregulation. It is proposed that cytokines released from the inflamed gut, such as interleukin-1, interleukin-6, and tumor necrosis factor-α, may drive bone inflammation.4
CRMO is a diagnosis of exclusion, made after ruling out infectious osteomyelitis, neoplasms like leukemia and Langerhans cell histiocytosis, and other autoimmune/autoinflammatory disorders. Bristol and Jansson diagnostic criteria are commonly used in pediatric patients.3
These differential diagnoses were ruled out in our patient based on clinical features and the absence of systemic symptoms suggestive of malignancy or infection, negative blood cultures, and MRI findings (e.g., multifocal, symmetric lesions with no abscess or sequestrum). Whole-body MRI revealed bilateral asymmetric subchondral bone marrow oedema in the sacroiliac joints. The femurs showed peri-physeal edema on the left near the greater trochanter and edematous changes in the peri-physeal metaphysis of the femur on both sides, and similar changes in the proximal tibia bilaterally, in keeping with a diagnosis of CRMO.
Laboratory tests, bone imaging, and bone biopsy are typically required for diagnosis. Radiological findings commonly include one or more osteolytic lesions with sclerotic borders, periosteal reactions, and bone edema. Histopathological findings typically show an inflammatory infiltrate with macrophages, lymphocytes, and plasma cells, along with bone remodeling, fibrosis, and osteoclast-like giant cells, all in the absence of infection. Our patient’s parents declined the biopsy and histology examination. While laboratory findings are often normal, elevated inflammatory markers have been observed in some patients.4
There is no standardized treatment for CRMO due to the lack of randomized trials. NSAIDs are considered first-line but are relatively contraindicated in patients with colitis. Alternative options include oral corticosteroids, methotrexate, sulfasalazine, and TNF-α antagonists. Limited studies have shown that bisphosphonates may provide substantial disease control.3,4
Our patient was initially managed with an escalated dose of infliximab at 7.5 mg/kg, six weekly and then four weekly. However, over time, he lost response to the treatment and subsequently developed anti-infliximab antibodies. He was then managed with monthly pamidronate infusions, which proved ineffective. Ultimately, he was started on adalimumab, resulting in the resolution of bone pain and sustained gastrointestinal remission—clinically, biochemically, and histologically.
Paradoxical CRMO refers to the unexpected onset or worsening of CRMO symptoms during treatment with anti-TNFα agents, which are typically used to manage inflammatory conditions, including CRMO itself. It is typically characterized by symptom emergence or worseningafter starting anti-TNFα therapy, with improvement after discontinuation.5, 6
In our patient, paradoxical CRMO is unlikely. The patient’s symptoms did not improve after stopping the anti-TNFα agent. Despite the temporal relationship between infliximab initiation and CRMO symptoms, the absence of clinical improvement after withdrawal—along with low trough levels and the presence of anti-drug antibodies—supports a non-paradoxical CRMO diagnosis.
CRMO should be considered in the differential diagnosis of IBD patients presenting with unexplained bone pain, difficulty walking, or abnormal uptake on bone imaging.
Disclosure
The authors declare no conflicts of interest.
references
- 1. Sergi CM, Miller E, Demellawy DE, Shen F, Zhang M. Chronic recurrent multifocal osteomyelitis. A narrative and pictorial review. Front Immunol 2022 Aug;13:959575.
- 2. Bousvaros A, Marcon M, Treem W, Waters P, Issenman R, Couper R, et al. Chronic recurrent multifocal osteomyelitis associated with chronic inflammatory bowel disease in children. Dig Dis Sci 1999 Dec;44(12):2500-2507.
- 3. Roderick MR, Shah R, Rogers V, Finn A, Ramanan AV. Chronic recurrent multifocal osteomyelitis (CRMO) - advancing the diagnosis. Pediatr Rheumatol Online J 2016 Aug;14(1):47.
- 4. Tzaneti A, Athanasopoulou E, Fessatou S, Fotis L. Chronic nonbacterial osteomyelitis in inflammatory bowel disease. Life (Basel) 2023 Dec;13(12):2347.
- 5. Cordesse A, Ecochard-Dugelay E, Melki I, Caseris M, Belarbi N, Hugot JP, et al. Chronic recurrent multifocal osteomyelitis in pediatric Crohn disease, a paradoxical effect to antitumor necrosis factor alpha. JPGN Rep 2020 Aug;1(2):e007.
- 6. Cachen L, Nocturne G, Collins M, Meyer A, Gleizes A, Hacein-Bey-Abina S, et al. Articular manifestations in patients with inflammatory bowel diseases treated with anti-TNF. RMD Open 2022 Jan;8(1):e001697.