
Chronic Adreno-Cortical Insufficency Associated with a Unilateral Adrenal Mass
ABSTRACT
Adreno-cortical insufficiency in the context of an adrenal mass can be a challenging clinical problem. The two main possibilities are either a benign mass or a malignant pathology.1
We describe here a patient who was investigated for chronic adreno-cortical insufficiency and was found to have a left adrenal mass that was later confirmed histopathologically to be tuberculous in nature.
Submitted: 29 August 2007
Reviewed: 5 October 2007
Accepted: 1 November 2007
From the departments of 1Department of Family Medicine & Public Health; 2Department of Medicine; 3Department of Child Health, College of Medicine & Health Sciences, Sultan Qaboos University, Muscat, Oman.
Address Correspondence and reprint request to: Abdullah Balkhair MD, FRCPC, Department of Medicine, College of Medicine & Health Sciences, Sultan Qaboos University, PO Box 35, Al-Khod 123, Muscat, Sultanate of Oman
Email: balkhair2000@hotmail.com
CASE REPORT
A 42 years old female presented with a two year history of tiredness, easy fatigability, and generalized body aches. She described increased skin pigmentation particularly in the peri-orbital regions, neck, upper chest and palmar creases. She was on no medications. Her family history was positive for pulmonary tuberculosis affecting her mother.
On physical examination, she looked healthy, but tired. Her blood pressure was 130/78 mmHg with no postural drop. Her palmar creases and buccal mucosa were hyperpigmented.
The initial serum cortisol concentration was less than 243 nmol/l. Her peak cortisol response to the Synacthen test was 311 nmol/l (expected >550 nmol/l) (Alliance Pharmaceuticals, Wiltshire). The baseline concentration of adrenocorticotrophic hormone was 42.7 pmol/l (normal range < 10.7 pmol/l). The patient had a tuberculin skin test that was positive at 12 mm after 48 hours. A chest x-ray was normal. CT scan of the chest revealed a patchy fibrotic lesion in RUL with small plaque of calcification in the right apical and the right tracheo-bronchial region. These lesions were thought to be consistent with old tuberculous lesions. MRI scan of the abdomen showed an enlarged left suprarenal gland with specs of calcifications .The outer limb of the left suprarenal was bulbous (Figures 1,2). T1 images showed only rim enhancement. These findings were suggestive of a granulomatous pathology although, given the appearance, a neoplastic process was not possible to exclude. The right suprarenal was normal .The patient was then subjected to a CT guided Tru-cut biopsy of the Left suprarenal gland. The histopathology revealed caseating granulomas. Stain for Acid Fast Bacilli was negative. However, the cultures later confirmed the growth of mycobacterium tuberculosis.
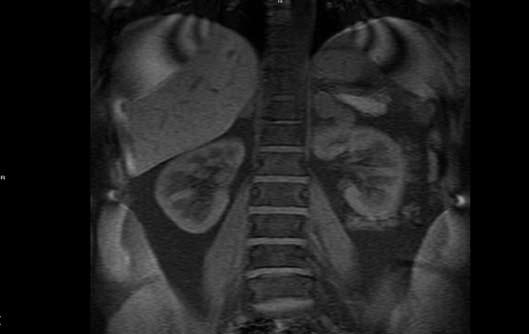
Figure 1. Gadolinium enhanced MR scan of the abdomen demonstrating
the enlarged left adrenal gland on the frontal view. Note the rim enhancement.
The patient was treated with a standard anti-tuberculous regimen and was also started on steroid replacement therapy with hydrocortisone and fludrocortisone. The patient improved considerably with regards to her constitutional symptoms and was back to her baseline activities. A year later, a follow up MRI scan of the adrenals showed reduction in the size of the adrenal mass and increased calcification. The patient remained asymptomatic during the follow-up period.
DISCUSSION
Tuberculosis is one of the leading causes of adrenal insufficiency worldwide, but the presence of TB may be difficult to diagnose.2
In a large retrospective study of autopsy results in Hong Kong, Lam and Lo found active TB in 6.5% of cases. However, in more than 70% of these patients, TB was diagnosed only at autopsy. Adrenal insufficiency was found in 6% of the patients with active TB.2
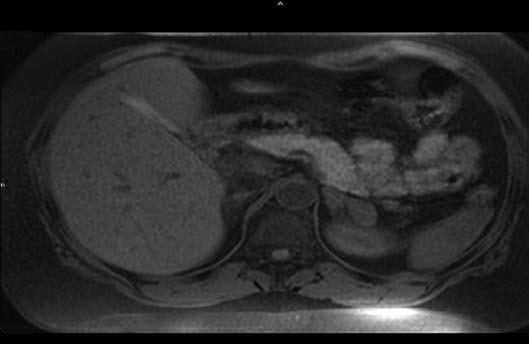
Figure 2. Gadolinium enhanced MR scan of the abdomen.
Note the enlarged left adrenal gland on the coronal view.
It may also be difficult to identify TB as the cause of adrenal insufficiency, as illustrated by Serter and associates.3 The manifestations can be both acute and chronic.3,7,9 Numerous efforts were made to try to establish features on CT scan of the adrenal glands to distinguish between adrenal tuberculosis and other benign and malignant adrenal pathology.4,5,6 Ultimately, tissue diagnosis remains the mainstay of diagnosis8. Our patient presented with insidious vague symptoms that prompted investigation of adreno-cortical function. Her hormonal profile confirmed that she had primary adreno-cortical insufficiency. The patient made a remarkable symptomatic improvement when she was started on steroid replacement therapy. The finding of a left adrenal mass was an interesting finding. The mass had features that suggested the diagnosis of tuberculous adrenal involvement, namely preservation of gland’s contour, rim enhancement and obvious speckled calcifications. In addition, given the epidemiology of tuberculosis in this part of the world and other evidence of tuberculosis on CT scan of chest and a positive tuberculin skin test, the likelihood of tuberculosis was quite high. However, the unilateral nature of the mass was worrisome. The decision to subject the patient to CT guided biopsy was indeed prudent before committing her to a prolonged treatment regimen with anti-tuberculous medications. Findings on histopathology and later on culture were in keeping with the clinical suspicion. This was augmented by the findings on repeat scan of the shriveling of the previously enlarged left adrenal gland and increasing calcification.
Tuberculosis (TB) is one of the leading causes of adrenal insufficiency worldwide, but the presence of TB may be difficult to diagnose.2 The manifestations can be both acute and chronic.3,4,5 Numerous efforts were made to try to distinguish between adrenal tuberculosis and other benign and malignant adrenal pathologies using CT scan.1,6,7 Ultimately, tissue biopsy remains the mainstay of diagnosis.8
Adrenal tuberculosis is being increasingly recognized as a cause for chronic and acute adrenocortical insufficiency. Our case illustrates a rather unusual and rare manifestation of chronic tuberculous adreno-cortical insufficiency.
REFERENCES
1.
Yang ZG, Guo YK, Li Y, Min PQ, Yu JQ, Ma ES. Differentiation between tuberculosis
and primary tumors in the adrenal gland: evaluation with contrast-enhanced CT. Eur
Radiol 2006;:1-6.
2.
Haddara WM, Van Uum SH. TB and adrenal insufficiency. CMAJ 2004; 171:710.
3.
Serter R, Koc G, Demirbas B, Culha C, Ongoren AU, Usten H et al. Acute adrenal crisis
together with unilateral adrenal mass caused by isolated tuberculosis of adrenal
gland. Endocr Pract 2003; 9:157.
4.
Kon YC, Sokoloff M, Straus FH 2nd, Weiss RE. Addisonian crisis and tuberculous epididymo-orchitis.
Endocr Pract. 2002; 8:365-369.
5.
Ueda H, Ohara H, Sakakibara T, Tonami H, Onishi S, Otake R et al. Tuberculosis of
the contralateral adrenal gland: a case report. Hinyokika Kiyo 1985; 31:449-456.
6.
Wang YX, Chen CR, He GX, Tang AR. CT findings of adrenal glands in patients with
tuberculous Addison’s disease. J Belge Radiol 1998; 81:226-228.
7.
Yilmaz T, Sever A, Gur S, Killi RM, Elmas N. CT findings of abdominal tuberculosis
in 12 patients. Comput Med Imaging Graph 2002; 26:321-325.
8.
Yee AC, Gopinath N, Ho CS, Tao LC. Fine-needle aspiration biopsy of adrenal tuberculosis.
Can Assoc Radiol J 1986; 37:287-289.