| |
Introduction
Pain relief during maternal labor is one of the main goals of maternity care. It is emphasized that request for pain relief be considered as a sufficient medical indication for the use of labor pain relief methods.1 Also, one of the most pressing concerns for pregnant women is the pain of labor,2,3 and it is this fear of pain which is the main of cause of cesarean section.4 Pain during the first stage of labor is generated largely from the uterus and cervix. Early on in labor, the pain of uterine contractions is transmitted predominantly through the T11 and T12 nerves.1 According to the gate control theory, pain intensity is influenced by numerous factors such as anxiety, environmental factors, culture, support from caregivers, focus of attention and previous experiences.5,6 Women’s expectations may limit the ability to predict the pain intensity before the beginning of labor.1 For some women, the pain of labor is accepted as a natural phenomenon, while others believe that little or no pain should be tolerated.7
During labor pain, there are increased levels of epinephrine and norepinephrine. Catecholamines are released from the adrenal medulla and are related to nausea, vomiting, increased blood pressure,2,7 and reduced uterine blood flow.2 Labor pain is managed by non-pharmacologic as well as pharmacologic methods and the effect of each method has long been confirmed.8 Analgesic drugs can be administered in three forms: topical, enteral, and parenteral.7 Opioids are the most common drugs for pain relief and are mostly prescribed in injectable form. These drugs inhibit neuronal transmission by neural system depression and thus relieve pain. All opioids are largely transmitted cross the placenta and may decrease the beat-to-beat variability of the fetal heart rate.9
Fentanyl, a Phenyl piperidine derivative, is a short-acting and potent synthetic narcotic.1,7 It is administered in subcutaneous, oral and patch forms, although these forms are not completely evaluated in labor.9,10 Due to its short half-life, fentanyl is considered a good option for labor pain relief. The usual dose in labor is around 25-50 µg IV, and its peak effect becomes apparent 3-5 min after drug infusion, which is repeated at 30-60 minutes intervals. All opioids cause side effects such as respiratory depression, nausea, vomiting, euphoria or sedation.10 Because fentanyl has no active metabolites, intravenous infusion of the drug can provide good analgesic effect when used as an alternative labor analgesic when epidural analgesia is contraindicated.11 For instance, regional block is contraindicated in some pregnant women, such as those with spinal abnormalities, infection or coagulopathy.12 Fentanyl should not be given when there is non-reassuring fetal heart rate pattern, maternal respiratory rate of 8 breaths per minute or less, or when maternal oxygen saturation is less than 95%.9
Meanwhile, meperidine is the most common opioid used worldwide for pain relief during the first stage of labor.1 Several comparative studies have shown that analgesic effects of intravenous fentanyl are better than meperidine (or pethidine).10 Also, some researchers have reported a significantly higher level of satisfaction in fentanyl groups than women receiving pethidine (p<0.01).5 In 2005, Fathi et al. reported that spinal analgesia with fentanyl decreased the length of the first stage of labor (p<0.01).12 But few studies have been conducted focusing on the efficacy of intravenous fentanyl administration on the duration of the active phase of labor and pain intensity; therefore, this study aims to determine the effect of fentanyl on pain as well as its effect on the duration of the active phase of labor.
Methods
This clinical trial was conducted on 70 multiparous parturients undergoing labor from May to July 2006 at the maternity unit of the Tamin Ejtemai Hospital, Torbat Heydariyeh City, Iran. First, based on results from a pilot study on 10 parturients (and mean duration of the active phase), effect size was obtained at 0.4 hours with power 80% and confidence level of 95%, the sample size was then calculated to be 70 parturients.
Inclusion criteria were as follows: multiparous pregnant women (gravida 2-7); term singleton pregnancy; cephalic presentation; low risk pregnancy with no history of drug tolerance (addiction), medical or mental diseases. While the exclusion criteria included the following: Respiratory rate ≤8 or maternal bradycardia (pulse rate less than 60) and severe congenital anomalies in neonate after birth. Written consent was obtained from each participant and the eligible subjects were selected by convenience sampling at the onset of the active phase of labor (cervical dilatation 4-5 cm); samples were then randomly assigned. A coin was tossed to determine the subjects comprising the control and case groups (35 women per group).
In the case group, 50 micrograms fentanyl was prescribed in two doses with an interval of 1 hour after being diluted in 4 cc normal saline (total volume 5 cc - 25 µg /5 ml during 10 minutes infusion and repeated second dose an hour later 25 µg /5 ml) at zero and 60 minutes. On the contrary, the control group received no analgesic drug. Then, an assessor recorded verbal pain score scale (verbal pain score 0-10, where 0 = no pain and 10 = maximum pain) and pain was then categorized into 3 groups based on the scores: mild pain (1-3), moderate pain (4-7) and severe pain (8-10). Pain intensity was estimated four times (before and 1,2,3 hours after the intervention).
The usual observations during this research consisted of monitoring, non-invasive blood pressure, heart rate, fetal heart rate and maternal respiratory rate. Vital signs were recorded pre-administration and 5, 15, 30, 45, 60 minutes post-administration. Other data were collected such as age, parity, duration of labor, maternal side effects drowsiness, dizziness, nausea/vomiting, respiratory depression, hypotension (BP <90 mmHg or less than <20% of baseline), bradycardia (HR<60 beats min-1), and pruritus. Also, neonatal outcomes were recorded such as the outcome of birth (assessed using 1 and 5 minutes Apgar scores) and resuscitation efforts (if any). Fentanyl was last administered prior to birth and any confounding factors that would influence resuscitation, such as SGA and meconium aspiration were also recorded. An anesthesiologist and resuscitation equipment were available at all times.
Analysis was performed using an independent t-test, repeated measure ANOVA and chi-square tests via the SPSS 11.5 software.
Results
In this study, there was no statistically significant difference mean age (in the case group 28±1 years and in control group 26±1 years; p=0.215) between the two groups. There were no significant differences in gravidity, parity, fetal heart rate, contraction duration or HR between the two groups.
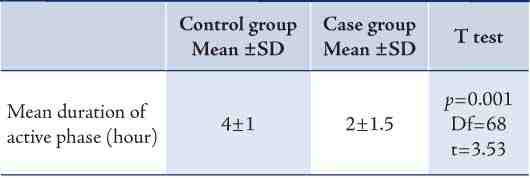
As shown in Table 1, the duration of the active phase was calculated 2±1.5 hours in the case group and 4±1 hours in the control group; a finding that was statistically significant (p=0.001). Mean pain scores decreased in the fentanyl group and there was a significant difference between the two groups (p=0.002), as detailed in Table 2. While, 63% of fentanyl recipients reported higher levels of satisfaction with analgesia and only 8% reported little satisfaction. During the first hour of fentanyl administration, no severe pain was apparent within the case group, but 89% of parturient in the control group reported severe pain. (Table 3)
Table 1: Mean duration of active phase of labor in two groups.
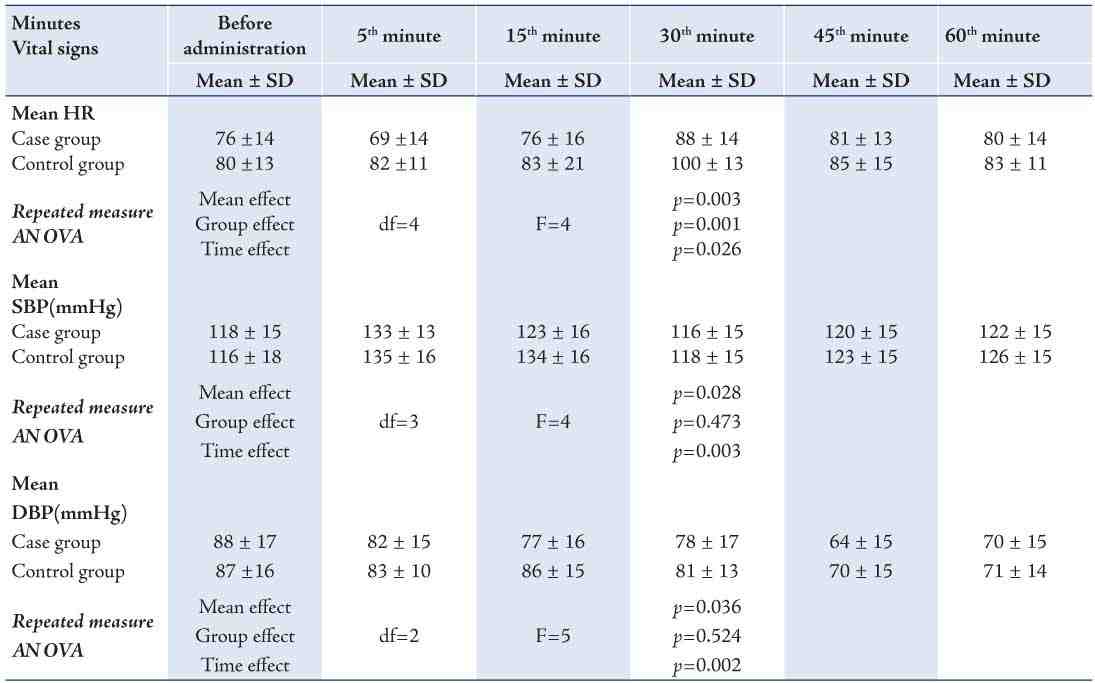
As indicated in Table 2, no significant difference was observed between the two groups in terms of the mean systolic blood pressure measured at different stages. The effect time was significant (p=0.003) but the group effect was not significant (p=0.437). Also, Repeated measure ANOVA showed no significant difference in mean diastolic blood pressure measured at different stages between the two groups, but the time effect (p=0.002) against the effect of the group was however, significant. After fentanyl administration, statistical analysis showed the mean heart rate to be significantly different between the two groups (p=0.001). (Table 4)
Table 2: Mean Pain Scores (0-10) in active phase of labor between the two groups.
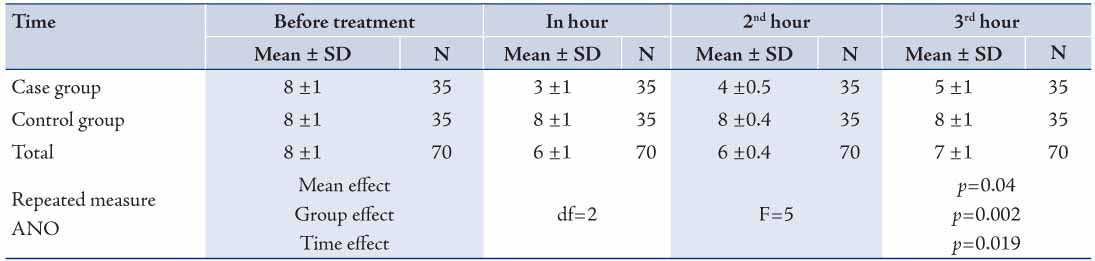
Table 3: Pain intensity at different stages of the active phase between the two groups.
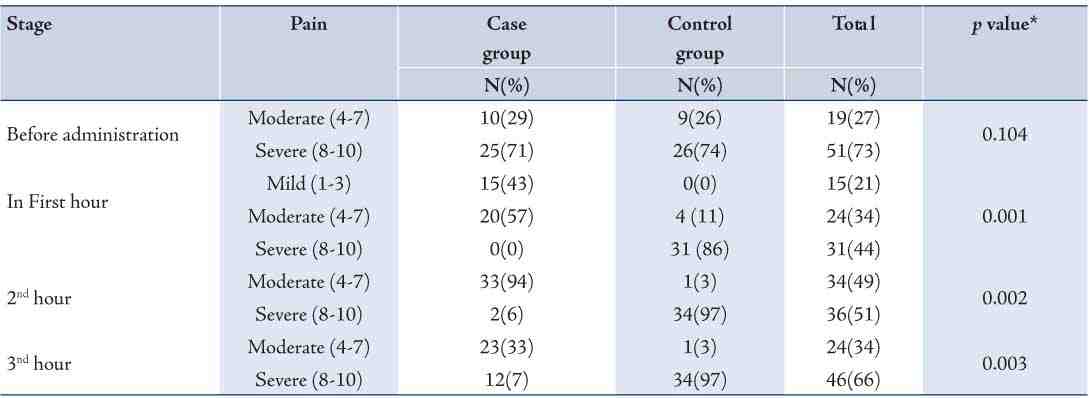
Table 4: Mean heart rate, systolic and diastolic blood pressure in the minutes before and after administration in both groups.
Cesarean delivery was performed in five cases due to fetal distress and meconium staining in the two groups (3 and 2 in the case and control groups, respectively), but the difference was not statistically significant. Apgar scores (1 and 5 mins) were comparable between the two groups, and thus there were no differences in Apgar scores between the two groups. There were also no differences in complications between the two groups (nausea and vomiting, urinary retention and respiratory depression).
Discussion
The present study showed that intravenous administration of Fentanyl decreased pain intensity during the first stage of labor compared to women who received no analgesia. In addition, it shortened the duration of the active phase of labor. There was a significant difference between the control group and the case group (Table 2). Various studies have shown that patient-controlled intravenous infusion of fentanyl (PCA) is effective as epidural analgesia on pain relief when epidural analgesia is contraindicated.1,7 In 2007 Hutchison et al. demonstrated the effect of Fentanyl on pain relief after post-operative orthopedic surgery.13
In the present study, during the third hour of control, pain score increased compared to the second hour. Similar results of analgesia have been shown in other studies.14,15 The results of pain relief after administration of fentanyl are consistent with Douma’s studies on labor pain. Furthermore, Douma et al. (2010) reported that pain scores returned to baseline values within 3 hrs after the start of treatment.14 The short half-life of fentanyl (30-60 minutes) and unrepeated IV fentanyl after the second dose (according to hospital policies) can explain the increasing pain score in third hour. Also, pain scores tended to increase with the progress of labor.15
In the current study, IV fentanyl was desirable for severe pain and 43% of women in the case group expressed mild pain but 86% of women in the control group declared suffering from severe pain (Table 4). Whereas, Thakore et al. (2009) concluded fentanyl to be desirable for moderate pain relief.6 In a randomized controlled trial, Thakore et al. (2009) assessed pain intensity after administration of fentanyl in post-operative hysterectomy.16 Marvah and et al. (2011) reported mild pain reduction after fentanyl intravenous analgesia.15 The difference in results is not clear but this difference could be attributed to differences in culture and emotional state between the groups.6,7
While in the second part of this study, the effect of IV slow fentanyl was investigated on the duration of the first stage of labor. Duration of the active phase was 2±1.5 hours in the case group and 4±1 hours in the control group, the difference between the two groups was significant (p=0.001). We only found two studies that evaluated the effect of fentanyl on the duration of labor. Fleet et al. reported the length of labor to be significantly longer for the fentanyl group than the control group (p=0.001).5 In contrast, Fathi et al. (2006) reported the length of the first stage of labor was shorter in fentanyl group than in the case group (144 minutes vs. 312 minutes, p<0.01).11
In a study which investigated the the effect of spinal analgesia with 50 micrograms fentanyl on stages of labor in nulliparous women, they reported no differences between the different stages of labor; however, the samples were smaller and induced labor was observed.12 While a study reviewing the side effects of IV fentanyl in mother and neonate reported that fentanyl (a short-acting opioid) poses fewer side effects to both mother and infant,5 however, the administration of pethidine was found to be more common in maternity wards in another study.15 The results from this research also expressed that IV administration of fentanyl is safe, while another important finding of the study was that there were no neonatal neurologic complications. The study also reported IV fentanyl to be effective for pain relief and that it can be used by midwives without need to present specialized services (anesthesiologist) in maternity wards.7 Similarly, Rayburn et al. (1989) in their randomized study reported that naloxone was used far less in infants whose mothers received fentanyl for pain relief than infants whose mothers received meperidine for the same indication (2% vs. 13%).17 Similar results with fentanyl were also reported by Atkinson in a comparison between fentanyl and butorphanol, who found that infants whose mothers received fentanyl were more prone to require naloxone than their counterparts whose mothers received butorphanol (28% vs. 16%).18
Also, Forster et al. (1998) observed no differences between 1 min APGAR scores and neonatal respiratory depression between opioid recipient and non-opioid recipient groups.10 In contrast, Nikkola et al. observed numerous events of low saturation (SpO2 <90%) in neonates of mothers who received fentanyl PCA.19 This difference has been attributed to the different dosages and cumulative effect of fentanyl in some studies. Due to the elimination of the cumulative effect, the fixed bolus technique is very desirable for fentanyl and the use of a low-dose infusion has been suggested in some studies.15
In the current study, the mothers’ heart rate was lower in the fentanyl group than the control group at all minutes. This difference was statistically significant (p=0.001) [Table 3], an observation which is similar to the findings reported by Ghaffari et al.20 as a result of Fentanyl’s effect of reducing heart rate.21 The values for systolic and diastolic blood pressure were also lower at all minutes after intravenous administration of fentanyl; however, the differences between the two groups were reported to be of no significance (Table 2). Another study on Fentanyl has also reported very little effect on blood pressure.21 Therefore, similar findings are expected; however, repeated measure ANOVA showed significant statistical differences between values before and after intervention in each group (Table 3). The systolic blood pressure increased with the progression of labor, which could be attributed to the changes in position and fluid intake. In contrast, diastolic blood pressure decreased with the progression of labor in each group; however, we found no explanation for this result, although administration of fentanyl alone leads to little change in systemic blood pressure (SBP and DBP). Thus, further studies are recommended. Our results also showed that there was no significant difference in the incidence of labor complications between the two groups and 63% of fentanyl recipients expressed more satisfaction with analgesia, while only 8% of recipients who received fentanyl intravenously reported little satisfaction with analgesia.
On the other hand, this study presented with several limitations. For instance, it was not possible to control individual differences or previous experiences of the subjects. While another main limitation of the study was the inability to evaluate anxiety, which was induced by sleepiness among the women after drug administration. Thus, we recommend assessing the efficacy and safety of fentanyl on neonatal and maternal outcomes over longer periods of time.
Conclusion
This study revealed that intravenous administration of fentanyl reduces the duration of the active phase of labor, as well as showing fentanyl to provide good satisfaction and proper pain relief during the first stage of labor with no associated side effects observed in infants. Therefore, fentanyl can be used as a desirable agent for pain relief during labor.
Acknowledgments
We would like to thank the midwives and anesthesiologists at the maternity ward of Tamin Ejtemai Hospital in Torbat Heydariyeh for their efforts.
References
1. Cunningham FG, Leveno KJ, Bloom SL, Hauth JC, Rouse D, Spong CY. Williams obstetrics. In: Obstetrical anasthesia. 23th ed. McGraw-Hill: 2010.
2. Kordi M, Rohani S, Fadii AR, Esmaili H. Effect of pressure on point of 6th spleen in labor pain in the first stage of labor. Iranian Journal of Obstetrics Gynecology and Infertility 2009;26(4):7-12.
3. Esfandiari M, Nankaley A, Sanjari N, Almasi A, Karimi S. Effectiveness of Entonox on Severity of Labor Pain in Women Referred to Maternity Ward of Imam Reza hospital, Kermanshah. Scientific Journal of Ilam University of Medical Sciences 2009;17(1):25-33.
4. Mirzaii F, Kaviani M, Jafari P. Evaluation of effect of foot reflexology in labor pain and duration of the first stage of labor. Iranian Journal of Obstetrics Gynecology and Infertility 2010;13(1):27-32.
5. Fleet J, Jones M, Belan I. Subcutaneous administration of fentanyl in childbirth: An observational study on the clinical effectiveness of fentanyl for mother and neonate. Midwifery. In Press.
6. Hoffman H, Chambers G, Meyer W, Arceneaux L, Russel W, Seibel E, et al. Virtual reality as an adjunctive non-pharmacologic analegesic for acute burn pain during medical procedures.Annual behavoreal medicine 2011;41:183-191.
7. Murray ML, Huelsmann GM. labor and delivery nursing. A guide. To Evidence Based Practice. In: Phases and stages of labor (Murray ML, Huelsmann GM.). First ed. Pub Springer: New York, 2008: 49.
8. Posnenkova OM, Kiselev AR, Gridnev VI, Popova YV, Shvartz VA. View on the problem of managing of medical care quality. Oman Med J 2012 May;27(3):261-262.
9. Miller RD. Miller’s Anesthesia. 6th ed. Pub Elsevier ChurcHill Livingstone: Philadelphia Pennsylvania, 2005: 2317.
10. Morley-Forster PK, Weberpals J. Neonatal effects of patient-controlled analgesia using fentanyl in labor. Int J Obstet Anesth 1998 Apr;7(2):103-107.
11. Goetzl LM; ACOG Committee on Practice Bulletins-Obstetrics. ACOG Practice Bulletin. Clinical Management Guideline for Obstetrician-Gynecologists. J Obstet Gynaecol 2002 Jul;100(36):177-191.
12. Fathi T, Asgrian YM, Mazlom SR. Efficacy of spinal analgesia on stages of labor 17 Shahrivar Hospital Mashhad. J obstetrics and gynecology research - scientific research (Medicine). 2006; 2(18).
13. Hutchison RW, Hae Chon E. Tucker WF, Gilder R. A Comparison of a Fentanyl, Morphine and Hydromorphone Patient-Controlled Intravenous Delivery for Acute Postoperative Analgesia: A Multicenter Study of Opioid-Induced Adverse Reactions Wolters Kluwer Health, Pub. 2006; 659-663.
14. Douma MR, Verwey RA, Kam-Endtz CE, van der Linden PD, Stienstra R. Obstetric analgesia: a comparison of patient-controlled meperidine, remifentanil, and fentanyl in labour. Br J Anaesth 2010 Feb;104(2):209-215.
15. Marwah R, Samah Hassan S, Carvalho JA, Balki M. Remifentanil versus fentanyl for intravenous patient-controlled labour analgesia: an observational study. Can J Anesth 2012 Oct 59:246-254.
16. Thakore B, Jacquelin DM, Saksen S, Butani M. Comparison of fentanyl and butorphanol for postoperatrative pain relief with intravenous patient controlled analgesia. J acute pain. 2009 December;11(3):93-99.
17. Rayburn WF, Rathke A, Leuschen MP, Chleborad J, Weidner W. Fentanyl citrate analgesia during labor. Am J Obstet Gynecol 1989 Jul;161(1):202-206.
18. Atkinson BD, Truitt LJ, Rayburn WF, Turnbull GL, Christensen HD, Wlodaver A. Double-blind comparison of intravenous butorphanol (Stadol) and fentanyl (Sublimaze) for analgesia during labor. Am J Obstet Gynecol 1994 Oct;171(4):993-998.
19. Nikkola EM, Ekblad UU, Kero PO, Alihanka JJ, Salonen MA. Intravenous fentanyl PCA during labour. Can J Anaesth 1997 Dec;44(12):1248-1255.
20. Ghaffari MH, Aslani SH, Marashi M. Remifentanyl effects on hemodynamics of pregnant women to elective cesarean section with general anesthesia. J Asrar. 2009;16:94-99.
21. Sdarles LM, Miller RD. Miller’s Anesthesia review -2 ed. Pub Elsevier ChurcHill Livingstone: Philadelphia Pennsylvania, 2013: 71.
|
|