Superior herniation of normal mediastinal thymus is an intermittent migration of the broadest part of normal mediastinal thymus into the suprasternal region during increased intrathoracic pressure.1–4 It is a rare clinical entity and a least considered cause of anterior neck mass due to lack of awareness, leading to extensive unnecessary investigations and interventions. The thymus is necessary for normal immune function in the pediatric age group. It is important to differentiate superior herniation of normal thymus from other causes of anterior neck swelling, particularly ectopic cervical thymus, to avoid unnecessary surgical excision. Therefore, a high level of clinical suspicion and awareness is of paramount importance.5

Figure 1: (a) Appearance of suprasternal swelling during crying (superior herniation of normal thymus during raised intrathoracic pressure). (b) The disappearance of swelling when the child is quiet.
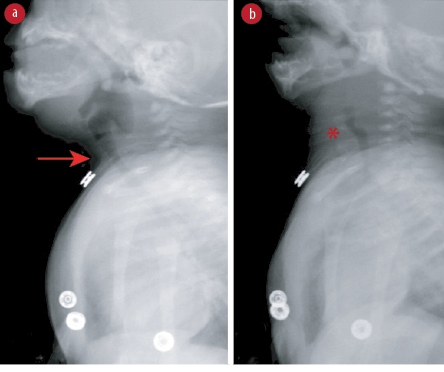
Figure 2: Fluoroscopic examination of the neck in lateral view. (a) The normal appearance of the trachea without the presence of suprasternal soft tissue (arrow). (b) Intermittent appearance of a soft tissue lesion (asterisk) in the suprasternal region anterior to the trachea displacing the
trachea posteriorly.
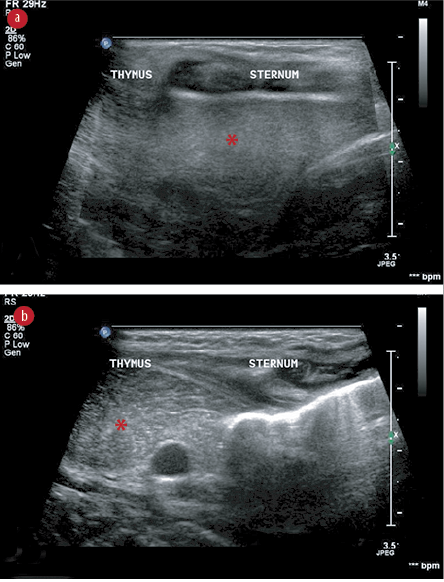
Figure 3: (a) Midline sagittal ultrasound image using a high-frequency linear transducer (5–12 MHz) through the sternal window reveal a homogeneous hypoechoic structure (asterisk) in the retrosternal region with internal echogenic foci giving starry sky appearance, normal sonographic morphology of the thymus in a neonatal period. (b) Shows intermittent interval displacement of the thymus in the suprasternal region in the midline anterior to the trachea. No other soft tissue mass was visualized. The findings are consistent with intermittent suprasternal herniation of the normal thymus gland.

Figure 4: At four years old, the patient showed no obvious suprasternal swelling (a) at rest or
(b) during straining.
Case report
A full-term male neonate with insignificant birth history, who remained clinically well and was discharged on the second day of life, presented at three weeks of age to the emergency department at Sultan Qaboos University Hospital with a history of anterior neck swelling that was only visible during crying and was associated with noisy breathing since the age of two weeks. There was no history of apnea, cyanosis, feeding difficulties, or respiratory distress. On examination, there was an anterior midline neck swelling arising from the suprasternal notch and extending up to the mid of the neck, visible only during crying and associated with stridor [Figure 1]. The swelling was soft in consistency and non-pulsatile. There was no bruit, and the overlying skin appeared normal. Other systemic examination was unremarkable except for bilateral hydrocele. There was no dysmorphism, and he was thriving well with anthropometric measurements at the 50th percentile for age and sex. Our differential diagnosis included apical lung herniation, ectopic cervical thymus, and laryngocele. Chest X-ray revealed the apical part of right upper lobe was hyperinflated. Computed tomography (CT) angiogram of the neck and thorax ruled out congenital and vascular anomalies; there was a bulky thymus, normal for his age. Laryngobronchoscopy revealed normal upper and lower airway anatomy. A noticeable bulge was observed at the suprasternal region, which appeared during inspiration and disappeared during expiration, raising the possibility of pleural bulging or apical lung herniation. However, on clinical examination, there was no correlation between the swelling and normal breathing. Fluoroscopy showed an intermittent soft tissue lesion in the suprasternal region anterior to the trachea [Figure 2]. Finally, ultrasound imaging of the neck revealed a soft tissue lesion from the superior mediastinum, which was solid and in continuity with the thymus [Figure 3]. The diagnosis of superior herniation of normal thymus was established. The patient was managed conservatively and discharged in a stable condition. On follow-up at the age of 14 months, he remained well and thriving with no signs of respiratory distress or stridor noted. A phone follow-up with the mother when the patient was four years old reported that the swelling was no longer evident during straining or Valsalva maneuver [Figure 4].
Discussion
This three-week-old male neonate presented with anterior neck swelling at the suprasternal region apparent only during crying and associated with stridor. He was diagnosed with superior herniation of the normal thymus.
Superior herniation of the normal thymus is a benign cause of anterior midline neck swelling and requires no surgical intervention as the thymus involutes with age.2 It is defined as an intermittent herniation of the broadest part of normal thymus in suprasternal region out of superior mediastinum during raised intrathoracic pressure.1–4 This abnormal movement of the thymus is possible because of loose connective tissue surrounding the thymus.3,6 It is a rare clinical entity, and only a few cases are reported in the literature. However, its incidence on ultrasonography is reported as 9%.6 There is no particular gender predilection. However, it is reported to be more common in younger children,7 and familial patterns have also been reported.1 Other causes of neck masses that appear only during increase intrathoracic pressure include apical lung herniation, jugular phlebectasia, and laryngocele. All of these are easily differentiated from each other through imaging.2
It is crucial to differentiate benign superior herniation of the normal mediastinal thymus from the ectopic cervical thymus, which is due to a migrational defect during thymus embryogenesis and tends to malignant transformation. Surgical removal and histological examination are required for the establishment of a diagnosis of ectopic cervical thymus.5,8 Characteristic history, examination, and ultrasonography led to definitive diagnosis of superior herniation of normal thymus and avoidance of unnecessary invasive investigations such as biopsy and surgical removal.3 In classical cases, the parents primarily report a noticeable swelling in their child’s neck during crying or straining that is reproducible with Valsalva maneuver on examination in older children.3 Ultrasonography as the first imaging of choice reveals a midline suprasternal soft tissue with echogenicity and echo pattern similar to that of normal thymus and seen in direct continuity with the thymus in the upper mediastinum.6,9 However, in cervical ectopic thymus, anatomic continuity between normal thymus and ectopic tissue could not be demonstrated, and a Tru-cut biopsy is required to confirm the diagnosis.3,4 Magnetic resonance imaging is helpful to evaluate for any compression on adjacent structures.3
This neonate had an anterior midline neck swelling in the suprasternal region, which appeared during crying and disappeared at rest and during sleep. It was also associated with stridor, so laryngobronchoscopy and CT angiogram were done to rule out other structural abnormalities of the airway. We diagnosed our case using ultrasonography and managed him conservatively. Badawi et al,10reported a case of superior herniation of thymus in a preterm female infant who was born at 26 weeks gestation and presented at 38 weeks corrected gestational age with a similar clinical picture and diagnosed on ultrasound. McDougall et al,6 reported an eight-month-old male infant who presented with a three-month history of intermittent anterior midline neck swelling only during straining and was diagnosed by airway fluoroscopy rather than ultrasonography.
No surgical intervention is needed for superior herniation of normal mediastinal thymus, and it is expected to disappear with time, as depicted in our case.6,10
Conclusion
Herniation of normal thymus is the least considered cause of anterior neck swelling among physicians and radiologists due to its rarity. However, with the awareness of its clinical presentation, normal anatomy, and radiological findings, we can avoid unnecessary extensive investigations, misinterpretation, and even surgical excision. We recommend that for any child with anterior midline suprasternal swelling that appears during increased intrathoracic pressure and disappears at rest, radiological investigation with X-ray followed by ultrasound must be carried out before opting for more advanced investigations and invasive procedures.
Disclosure
The authors declared no conflicts of interest. Parental consent was obtained.
Acknowledgements
The authors would like to thank Sheila Magpayo, PTRP, EMT-D, for the help in editing this report.
references
- 1. Senel S, Erkek N, Otgun I, Cinar G, Cifci A, Yoney A. Superior herniation of the thymus into the neck–a familial pattern. J Thorac Imaging 2008 May;23(2):131-134.
- 2. Su SC, Hess T, Whybourne A, Chang AB. Intermittent midline suprasternal neck mass caused by superior herniation of the thymus. J Paediatr Child Health 2015 Mar;51(3):344-346.
- 3. Stuut M, van Zwieten G, Straetmans JM, Lacko M, Stumpel CT. The inflatable thymus herniation of the normal mediastinal thymus: a case report and review of the literature. Int J Pediatr Otorhinolaryngol 2016 Apr;83:74-77.
- 4. Ranga U, Aiyappan SK, Sujatha B, Pathy A, Veeraiyan S. Unusual cause of suprasternal swelling: cervical extension with herniation of mediastinal thymus. Indian J Pediatr 2015 Jul;82(7):657-658.
- 5. Senel S. A reminder on superior herniation of normal mediastinal thymus. Eur J Pediatr 2011 May;170(5):675.
- 6. McDougall CM, Culham G, Seear MD, Chilvers MA. Superior herniation of the mediastinum presenting as an anterior neck mass on straining. Pediatr Pulmonol 2012 Jul;47(7):710-712.
- 7. Costa NS, Laor T, Donnelly LF. Superior cervical extension of the thymus: a normal finding that should not be mistaken for a mass. Radiology 2010;256(1):238-242.
- 8. De Foer B, Vercruysse JP, Mariën P, Colpaert C, Pilet B, Pouillon M, et al. Cervical ectopic thymus presenting as a painless neck mass in a child. JBR-BTR 2007 Jul-Aug;90(4):281-283.
- 9. Mandell GA, Bellah RD, Boulden ME, Sherman NH, Harcke HT, Padman RJ, et al. Cervical trachea: dynamics in response to herniation of the normal thymus. Radiology 1993 Feb;186(2):383-386.
- 10. Badawi MAS, Jassim FA, Melhat AE, Zefov V, Singh D. Intermittent suprasternal neck mass in preterm infant. Ann Pediatr Child care 2019;1:1-4.