Substance abuse has large and reciprocal impacts on families.1 The World Health Organization (WHO) defines substance abuse as the harmful or hazardous use of psychoactive substances, including alcohol and illicit drugs.2 It includes the physiological signs of addiction, such as tolerance, withdrawal, social factors (impaired work performance, relationship dysfunction), and behavioral markers (risky use, inability to regulate use).3 People abuse substances like drugs, alcohol, and tobacco for different reasons, including pleasure, improved performance and vigilance, relief of depression, curbing hunger, and weight control.4,5 Psychoactive drug use is responsible for more than 400 000 deaths per year worldwide.6 The global level of alcohol consumption in 2016 was 6.4 L of pure alcohol per person aged ≥ 15 years, and in 2015, more than 1.1 billion people smoked tobacco.7
Substance abuse is associated with other health problems. Psychoactive substance use can lead to dependence syndrome — a cluster of behavioral, cognitive, and physiological phenomena that develop after repeated substance use and that typically include a strong desire to take the drug, difficulties in controlling its use, persisting in its use despite harmful consequences, a higher priority given to drug use than to other activities and obligations, increased tolerance, and sometimes a physical withdrawal state.2 Drug use disorders account for 0.55% of the total global burden of disease, and injection drug use accounts for an estimated 30% of new HIV infections outside sub-Saharan Africa and contributes significantly to hepatitis B and hepatitis C epidemics in all regions.8 Smoking elevates the risk of lung and other cancers, cardiovascular disease, and respiratory conditions.9,10 Alcohol intoxication and the use of substances like marijuana and solvents are associated with traffic and other types of injury, an increased risk of HIV infection, cognitive impairment, and mental disorders.11,12
Alcohol is a leading cause of death and injury in the Pacific.13 The New Zealand Mental Health Survey showed that the lifetime prevalence of any substance use disorder for Pacific people, in general, was 17.7% compared to 12.3% in the general population, and the 12-month prevalence was 4.9% compared to 2.7% in the general population.14 The most prevalent specific substance use disorders were related to alcohol use and marijuana use.15,16 The most recent New Zealand Health Survey found that for drinkers - the proportion engaged in ‘hazardous drinking’ in Pacific adults (39.2%) was almost double that of European/other New Zealanders (20.1%).17 Despite these grave consequences, it was found that there are strategies already in place to help those that seek help or are in need of treatments.
There is a need to identify the determinants of substance abuse to mitigate their burden and contribute preventative and education programs.
There are many factors that increase the likelihood of substance abuse among adolescents. Genetics, age, and gender contribute to adolescent substance abuse.18,19 Family history of substance abuse,20,21 irregular school attendance, and negative peer relationship may also be associated with substance abuse.22 The role of social and demographic structures such as racism, violence, unemployment rate, and low socioeconomic status are determinants of substance abuse among African people.23
Prevention programs can be in the form of short-term such as alcohol-related awareness building, medium-term like alcohol use behavior change, and long-term like cancer prevention. To increase the effectiveness of prevention programs, other factors should also be considered such as the level of education, parents’ education, and family income.24 Studies showed those individuals who are younger, unmarried, unemployed, and consume tobacco, alcohol, and illicit drugs have more chance to adhere substance abuse treatment services.25,26
The review of the literature found that there are limited data available on substance abuse in the Pacific island countries. This paper gathers the most recent studies done about Pacific Islanders on substance abuse. There have been reviews done on some particular substance abuse, however, this systematic review would be the first review done regarding the determinants and prevention strategies in the Pacific region. This review aims to identify the determinants and prevention strategies that have been undertaken to minimize the issue of substance abuse.
Methods
This systematic review was conducted following the Cochrane Library Guidelines and the PRISMA checklist. The following databases were used to obtain relevant articles: Medline, CINAHL, PsychInfo, EMBASE, Scopus, and Web of Science. The databases used were common among studies involving violence, which is why they were selected. Medical subheadings and keywords were used to achieve the relevant articles which included, substance*, abuse, prevent*, strategy, determinants, and Pacific. The search was done without considering the name of a specific region or country. To further the search for articles, AND and OR were used to combine the search parameters. The articles included in this study were published from January 2000 to July 2017, in the English language, peer-reviewed, and had full text accessible.
To protect the study from selection and assessment bias, two independent reviewers scanned the titles of all available studies and removed the irrelevant studies. The reviewers then read the abstracts of the remaining studies, again removing the irrelevant studies. The third step conducted by the reviewers was reading the full texts in order to obtain the final articles. A total of 17 studies met the study inclusion criteria [Figure 1]. 27,28
Once this was done, the reviewers searched the bibliographies of the selected studies to find more relevant articles. Following this, two more articles were included bringing the total to 19. The studies’ full texts were then printed for further analysis. Using the information from the selected studies, we developed an extraction sheet (Annex 1) four sections including: study information, population, methodology, and results. A descriptive analysis was then carried out, and frequencies and percentages were recorded.
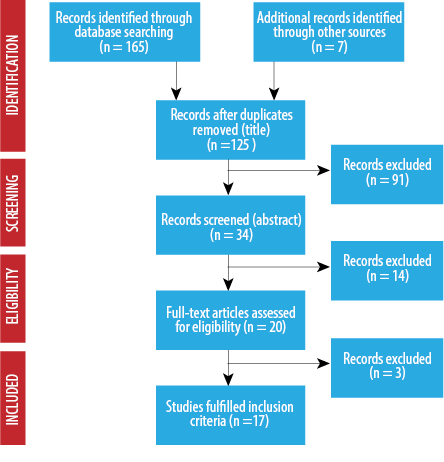
Figure 1: Article selection process.
Table 1: Characteristic of studies based on the year and region of conducting studies and age and gender of recruited participants.
|
Year of studies |
|
|
|
2000–2004 |
1 |
5.3 |
|
2005–2009 |
5 |
26.3 |
|
2010–2017 |
13 |
68.4 |
|
Region of conducted studies |
|
|
|
South Pacific |
|
|
|
New Zealand |
5 |
26.3 |
|
Pohnpei, Tonga and Vanuatu |
1 |
5.3 |
|
American Pacific |
|
|
|
USA |
1 |
5.3 |
|
USA and Hawaii |
7 |
36.8 |
|
Hawaii |
3 |
15.8 |
|
Asia Pacific |
|
|
|
Taiwan |
1 |
5.3 |
|
Taiwan, China, Nepal, Malaysia, and Sri Lanka |
1 |
5.3 |
|
Age of participants |
|
|
|
Adolescents |
2 |
10.5 |
|
Adolescents and adults |
2 |
10.5 |
|
Adolescents, adults, and older |
14 |
73.7 |
|
Not stated |
1 |
5.3 |
|
Gender of participants recruited |
|
Male |
3 |
15.8 |
|
Female |
1 |
5.3 |
|
Both male and female |
10 |
52.6 |
Table 2: Characteristics of studies based on study design, type, sampling, and data collection methods.
|
Study design |
|
|
|
Quantitative study |
14 |
73.7 |
|
Qualitative study |
2 |
10.5 |
|
Mixed methods study |
3 |
15.8 |
|
Type of studies |
|
|
|
Cross-sectional |
17 |
89.5 |
|
Quasi-experimental |
1 |
5.3 |
|
Cohort study |
1 |
5.3 |
|
Sampling methods |
|
|
|
Convenience sampling |
4 |
21.1 |
|
Random sampling |
6 |
31.6 |
|
Purposive sampling |
5 |
26.3 |
|
Stratified sampling |
2 |
10.5 |
|
Snowball sampling |
2 |
10.5 |
|
Data collection methods |
|
|
|
Questionnaire |
12 |
63.2 |
|
Face to face in-depth interview |
6 |
31.6 |
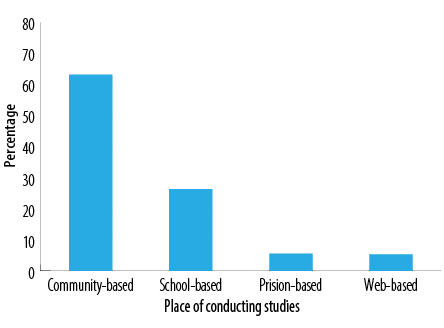
Figure 2: Percentage of studies based on the place of conducting the study.
Table 3: Frequency of substance abuse based on participants’ characteristics, facilitator, and environmental and socials factors.
|
Personal factors |
|
|
|
Age |
8 |
42.1 |
|
Ethnicity |
7 |
36.8 |
|
Sex |
12 |
63.2 |
|
Facilitator/promoter |
|
|
|
Peer supporter |
1 |
5.3 |
|
Perceive need for help |
1 |
5.3 |
|
Family members |
4 |
21.1 |
|
Partner support |
1 |
5.3 |
|
Church |
2 |
10.5 |
|
Community participation |
2 |
10.5 |
|
Environmental factors |
|
|
|
Home |
3 |
15.8 |
|
School |
2 |
10.5 |
|
Peers |
3 |
15.8 |
|
Social factors |
|
|
|
Lack of education |
2 |
10.5 |
|
Low income |
4 |
21.1 |
Table 4: Prevention strategies used in studies.
|
Use culturally appropriate and gender-sensitive treatments. |
1 |
5.3 |
Results
The general characteristics of included studies are presented in Table 1. Only 5.3% studies were published between 2000–2004, and the majority (68.4%) were published between 2010–2017. Approximately 36.8% of studies were based in the USA and Hawaii, 26.3% in New Zealand, and only 15.8% were conducted in Hawaii. About 73.7% of studies focused on adolescents, adults, and older age population, and approximately 15.8% of study participants are male.
The methodological features of the included studies are shown in Table 2. Almost 73.7% of studies used a quantitative approach, and only 15.8% of studies followed a mixed-method approach. Almost 89.5% included studies adopted a cross-sectional study design, whereas only 5.3% of studies are both cohort and quasi-experimental design. About 26.3% of studies used a purposive sampling technique to select the respondents, and approximately 31.6% of studies applied a random sampling technique, and 21.1% research studies used a convenience sampling method to identify the respondents for their research. About 63.2% of research studies used a questionnaire survey for their data collection method, and only 31.6% of studies used face to face in-depth interview techniques to collect data from their respondents.
The total number of participants in selected studies was 311 760. About 63.2% of studies were community-based, and 26.3% were school-based, as shown in Figure 2.
The frequency of substance abuse is displayed in Table 3. About 63.2% of studies concluded that gender is one of the most important factors for substance abuse followed by age, which accounts for 42.1%. Almost 21.1% research studies revealed that individuals are introduced to different types of abusing items by their family members, and it has also been reported in most of the studies (21.1%) that low income plays a major role for getting individuals addicted to substance abuse and approximately 15.8% cases the addictions to substance abuse starts from home and due to peer pressure.
About 5.3% of cases used culturally appropriate and gender-sensitive treatments as prevention strategies along with identifying sources of strength in families, communities, individuals, and even spiritual [Table 4].
Discussion
This is a systemic review study conducted in the South Pacific regions, American Pacific regions, and the Asian Pacific regions from 2000 to 2017. The review identifies the determinants and prevention strategies that have been undertaken to minimize the issue of substance abuse. The determinants identified in this review are personal, faciliatory/promotor, environmental, and social factors. The prevention strategies that have been identified are use culturally appropriate and gender-sensitive treatments and identifying sources of strength in families, community, individual, and even spiritual. These determinants and prevention strategies have been discussed below.
In this study, 42.1% of studies reported age as a determinant of substance abuse. Numerous studies have shown the increased issues related to substance abuse among the baby boomer generation and the increased efforts in the rehabilitation and treatment services. Substance abuse is the most common mental health complications emerging in childhood.29 Several anthropological studies in Micronesia have shown that the increased difficulties associated with substance abuse among the young generations are related to the phycological glitches caused by pressures between the western cultural impacts and traditional customs and institutions.30 In this study, 36.8% of studies reviewed reported ethnicity as a determinant of substance abuse. Studies have reported that Pacific Islanders/native Hawaiians had the highest self-reported rates for the treatment of alcohol and/or other drugs.31 Of the studies reviewed, 63.2% reported gender as a determinant of substance abuse. In a study by Smith et al,30 in 2007 it was stated that in all countries alcohol consumption and use of drugs were greater among males than females, whereas in Pohnpei, females used marijuana and methylated spirits more than males.
The results of this study showed that the prevention strategies should be more culturally appropriate and gender-sensitive to be more successful. Some social factors affect the treatment of substance abuse. For example, for abused women the risk of stigma related to their use is high and they are at high risk of physical and sexual abuse.32,33 Tailored programming for women, which induces practices that address abusers’ specific needs, which may help to increase their time in treatment.34 Training staff to provide a more empathetic and female-friendly environment will help the efficiency of prevention programs. Women’s issues are better to be discussed by same-gender groups and with a female therapist.33,35
There are many prevention strategies for substance abuse that have been examined among different groups. Technology-based intervention is a method that has been used to prevent substance abuse among adolescents. For example, web-based cognitive behavioral therapy (CBT) program for adults in substance use treatment.36 Another study showed that web-based CBT is an interesting method to prevent relapse for adolescents.37 In a randomized controlled trial study conducted among 129 adolescent-aged participants, participants in the intervention group were asked to complete 12 core lessons over three months which focused on evidence-based relapse prevention skills which adolescents in the control group have not received any intervention. The results showed that a significant increase in motivation to decrease or not misuse and also a greater decrease in drug use score drugs in three-month and six-month follow-up compared to the control group.38
Delivering motivational interviewing (MI) using different methods to prevent substance abuse has been examined in many studies. Another systematic study assessed 25 studies. The results revealed that telephone-based MI in treating substance abuse was supported by all studies, however, internet-based MI was effective in preventing and treating alcoholism and also smoking cessation. SMS-based MI was useful in controlling tobacco and drinking abuse.39
A pre and post-survey study examined the effectiveness of a national program called 4-H Health Rocks! to prevent tobacco, alcohol, and drug abuse among a total of 1192 respondents aged 8- to14-years old. The program consisted of instruction on the negative health consequences of substance abuse, social, and individual skills such as communication, decision making, and self-esteem practices. The results showed a positive sign in participants’ perceived knowledge, skills, and assets. However, the majority reported no change from before program to after program participation.40
Studies also showed significant effect in preventing substance abuse using interactive prevention programs than didactic-based lectures. Another pre- and post-survey examined the effectiveness of preventative programs among adolescents and their substance use knowledge and program perceptions. Students were divided into small groups led by near-peer health care professional trainees who provided information on the physical effects of substances on human organs. Results demonstrated significant positive increases in knowledge of substance use risks on mental and physical health.
In this study, 21.1% of studies reviewed reported family members, and low income as determinants of substance abuse, 15.8% of studies reported home and peers as determinants of substance abuse, and 10.5% of studies reported church, community participation, school, lack of education, and culture as determinants of substance abuse. Studies have reported evidence of a relationship between drunkenness and indicators of social disengagement and stress. A commonly quoted barrier and facilitator concerned relationships with peers has been reported.41 In Tonga and Vanuatu, students bullying others at school or communicating easily with friends reported higher odds of alcohol misuse and use of illegal drugs, while in Pohnpei and Vanuatu reported higher self-confidence was positively associated with this risk behavior.30 In Vanuatu, the factors associated with alcohol misuse and use of illegal drugs had negative perceptions of school teachers and watching television four hours per day. However, in the population, having informal communication with their family members had associated with a lower likelihood.30 Studies have reported an association between smoking and aggressive, anti-social behavior.30,42 Smokers reported lower general happiness.30
Conclusion
Substance abuse poses significant public health risks and therefore requires adequate interventions such as educating and informing individuals of the health risks associated with substance abuse and must be considered locally to promote the well-being of people. The review presents determinants and prevention strategies of substance abuse in the Pacific region. The review revealed that substance abuse prevention strategies are variable among the Pacific people, and there is a need for further studies on substance abuse in the Pacific and the increase in prevention strategies for substance abuse in the Pacific. The focus of prevention strategies should not only be on behavioral intervention but also should consider a mix of structural and policy-related approaches to prevention.
Disclosure
The authors declared no conflicts of interest. No funding was received for this study.
references
- 1. Gruber KJ, Taylor MF. A family perspective for substance abuse: Implications from the literature. J Soc Work Pract Addict 2006;6(1-2):1-29.
- 2. World Health Organisation. [cited 2018 July] Available from: http://www.who.int/topics/substance_abuse/en/. 2017.
- 3. Hasin D, Hatzenbuehler ML, Keyes K, Ogburn E. Substance use disorders: diagnostic and statistical manual of mental disorders, (DSM-IV) and International Classification of Diseases, (ICD-10). Addiction 2006;101:59-75.
- 4. Tabish S, Syed N, Syed N, Shah PS. Substance use disorder: a cultural catastrophe. Int J Sci Res (Ahmedabad) 2015;4(7):4.438.
- 5. Gupta S, Sarpal SS, Kumar D, Kaur T, Arora S. Prevalence, pattern and familial effects of substance use among the male college students -a north Indian study. J Clin Diagn Res 2013 Aug;7(8):1632-1636.
- 6. World Health Organization. World health statistics 2016: monitoring health for the SDGs sustainable development goals: World Health Organization; 2016.
- 7. World Health Organization. Almost half of all deaths now have a recorded cause, WHO data show. [cited 2019 February]. Available from: http://wwwwhoint/mediacentre/news/releases/2017/half-deaths-recorded/en/. 2017.
- 8. World Health Organization. Public health dimension of the world drug problem including in the context of the Special Session of the United Nations General Assembly on the World Drug Problem, to be held in 2016. [cited 2018 December]. Available from: https://apps.who.int/gb/ebwha/pdf_files/EB138/B138_11-en.pdf.
- 9. Mohammadnezhad M, Mangum T, May W, Lucas JJ, Ailson S. Common Modifiable and Non-Modifiable Risk Factors of Cardiovascular Disease (CVD) among Pacific Countries. World J Cardiovasc Surg 2016;6(11):153.
- 10. Anthonisen NR, Skeans MA, Wise RA, Manfreda J, Kanner RE, Connett JE; Lung Health Study Research Group. The effects of a smoking cessation intervention on 14.5-year mortality: a randomized clinical trial. Ann Intern Med 2005 Feb;142(4):233-239.
- 11. Degenhardt L, Hall W. Extent of illicit drug use and dependence, and their contribution to the global burden of disease. Lancet 2012 Jan;379(9810):55-70.
- 12. ToumbourouJ W, StockwellT, NeighborsC, Marlatt GA, Sturge J, Rehm J. Interventions to reduce harm associated with adolescent substance use. Lancet 2007 Apr;369(9570):1391-1401.
- 13. Hoy D, Roth A, Viney K, Souares Y, LopezAD. Findings and implications of the global burden of disease 2010 study for the Pacific Islands. Prev Chronic Dis 2014;11:E75.
- 14. Wells JE, Oakley Browne MA, Scott KM, McGee MA, Baxter J, Kokaua J; New Zealand Mental Health Survey Research Team. Te Rau Hinengaro: the New Zealand mental health survey: overview of methods and findings. Aust N Z J Psychiatry 2006 Oct;40(10):835-844.
- 15. Ministry of Health. Pacific peoples and mental health: A paper for the Pacific Health and Disability Action Plan Review. Wellington: New Zealand; 2008.
- 16. Ministry of Health. Drug use in New Zealand: key results of the 2007/2008 New Zealand alcohol and drug use survey. Wellington: New Zealand; 2009.
- 17. Sundborn G, Metcalf PA, Gentles D, Scragg R, Schaaf D, Dyall L, et al. ‘From Kava to Lager’–alcohol consumption and drinking patterns for older adults of Pacific ethnic groups, and Europeans in the Diabetes Heart and Health Study (DHAHS) 2002-2003, Auckland New Zealand. Pac Health Dialog 2009 Feb;15(1):47-54.
- 18. Bray JH, Adams GJ, Getz JG, McQueen A. Individuation, peers, and adolescent alcohol use: a latent growth analysis. J Consult Clin Psychol 2003 Jun;71(3):553-564.
- 19. Singh V-A, Thornton T, Tonmyr L. Determinants of substance abuse in a population of children and adolescents involved with the child welfare system. Int J Ment Health Addict 2011;9(4):382-397.
- 20. Braciszewski JM, Stout RL. Substance use among current and former foster youth: a systematic review. Child Youth Serv Rev 2012 Dec;34(12):2337-2344.
- 21. Duncan SC, Duncan TE, Strycker LA. Alcohol use from ages 9 to 16: a cohort-sequential latent growth model. Drug Alcohol Depend 2006 Jan;81(1):71-81.
- 22. Williams S, MacMillan H, Jamieson E. The potential benefits of remaining in school on the long-term mental health functioning of physically and sexually abused children: beyond the academic domain. Am J Orthopsychiatry 2006 Jan;76(1):18-22.
- 23. Pope RC, Wallhagen M, Davis H. The social determinants of substance abuse in African American baby boomers: effects of family, media images, and environment. J Transcult Nurs 2010 Jul;21(3):246-256.
- 24. Song C, Rutt JN, Anderson-Knott M. Widening the disparity gap: differences in outcomes for racial and ethnic groups in youth substance abuse prevention programming. J Child Adolesc Subst Abuse 2018;27(5-6):1-8 .
- 25. Bali V, Raisch DW, Moffett ML, Khan N. Determinants of nonmedical use, abuse or dependence on prescription drugs, and use of substance abuse treatment. Res Social Adm Pharm 2013 May-Jun;9(3):276-287.
- 26. Becker WC, Sullivan LE, Tetrault JM, Desai RA, Fiellin DA. Non-medical use, abuse and dependence on prescription opioids among U.S. adults: psychiatric, medical and substance use correlates. Drug Alcohol Depend 2008 Apr;94(1-3):38-47.
- 27. Mohammadnezhad M, Mangum T, Tawake K, Konrote A. Prevalence, determinants and other characteristics of violence among pacific countries: a systematic review study. EC Psychology and Psychiatry 2017;5(2):59-70.
- 28. Mohammadnezhad M, Konrote A, Kabir R. Determinants of suicide in Pacific region and needs for considering equality among Pacific people: a systematic review Pacific. Journal of Medical Sciences 2018;19(1):1-14.
- 29. Sahker E, Yeung CW, Garrison YL, Park S, Arndt S. Asian American and Pacific Islander substance use treatment admission trends. Drug Alcohol Depend 2017
Feb;171:1-8.
- 30. Smith BJ, Phongsavan P, Bauman AE, Havea D, Chey T. Comparison of tobacco, alcohol and illegal drug usage among school students in three Pacific Island societies. Drug Alcohol Depend 2007 Apr;88(1):9-18.
- 31. Wong MM, Klingle RS, Price RK. Alcohol, tobacco, and other drug use among Asian American and Pacific Islander adolescents in California and Hawaii. Addict Behav 2004 Jan;29(1):127-141.
- 32. Claus RE, Orwin RG, Kissin W, Krupski A, Campbell K, Stark K. Does gender-specific substance abuse treatment for women promote continuity of care? J Subst Abuse Treat 2007 Jan;32(1):27-39.
- 33. Marsh JC, Cao D, D’Aunno T. Gender differences in the impact of comprehensive services in substance abuse treatment. J Subst Abuse Treat 2004 Dec;27(4):289-300.
- 34. Greenfield SF, Trucco EM, McHugh RK, Lincoln M, Gallop RJ. The women’s recovery group study: a stage I trial of women-focused group therapy for substance use disorders versus mixed-gender group drug counseling. Drug Alcohol Depend 2007 Sep;90(1):39-47.
- 35. Campbell CI, Alexander JA, Lemak CH. Organizational determinants of outpatient substance abuse treatment duration in women. J Subst Abuse Treat 2009 Jul;37(1):64-72.
- 36. Carroll KM, Kiluk BD, Nich C, Gordon MA, Portnoy GA, Marino DR, et al. Computer-assisted delivery of cognitive-behavioral therapy: efficacy and durability of CBT4CBT among cocaine-dependent individuals maintained on methadone. Am J Psychiatry 2014 Apr;171(4):436-444.
- Trudeau KJ, Ainscough J, Charity S. Technology in treatment: are adolescents and counselors interested in online relapse prevention? Child Youth Care Forum. 2012 February ; 41(1): 57–71.
- 38. Trudeau KJ, Black RA, Kamon JL, Sussman S. A randomized controlled trial of an online relapse prevention program for adolescents in substance abuse treatment. Child & Youth Care Forum; 2017: Springer.
- 39. Jiang S, Wu L, Gao X. Beyond face-to-face individual counseling: A systematic review on alternative modes of motivational interviewing in substance abuse treatment and prevention. Addict Behav 2017 Oct;73:216-235.
- 40. Reeves KT, Donaldson JL, Naylor M, LeBleu L. Youths perceive some improvement in substance abuse prevention knowledge, skills, and assets from participation in 4-H health rocks! J Ext 2017;55(4):n4.
- 41. Donovan DM, Thomas LR, Sigo RLW, Price L, Lonczak H, Lawrence N, et al. Healing of the canoe: preliminary results of a culturally grounded intervention to prevent substance abuse and promote tribal identity for native youth in two Pacific northwest tribe. American Indian and Alaska native mental health research. American Indian and Alaska native mental health research. 2015; 22(1): 42–76.
- 42. Kellam SG, Anthony JC. Targeting early antecedents to prevent tobacco smoking: findings from an epidemiologically based randomized field trial. Am J Public Health 1998 Oct;88(10):1490-1495.
- 43. Masson CL, Shopshire MS, Sen S, Hoffman KA, Hengl NS, Bartolome J, et al. Possible barriers to enrollment in substance abuse treatment among a diverse sample of Asian Americans and Pacific Islanders: opinions of treatment clients. J Subst Abuse Treat 2013 Mar;44(3):309-315.
- 44. Huakau J, Asiasiga L, Ford M, Pledger M, Casswell S, Suaalii-Sauni T, et al. New Zealand Pacific ’peoples’ drinking style: too much or nothing at all? The New Zealand Medical Journal. 2005 Jun 3;118(1216):U1491.
- 45. Lee C-Y, Lu B, Shieh T-Y, Chang Y-Y. Patterns of betel quid, cigarette, and alcohol use, and their correlates with betel quid cessation in a male inmate population. Subst Use Misuse 2016;51(4):471-478.
- 46. Lee C-H, Ko AM, Warnakulasuriya S, Ling T-Y, Sunarjo, Rajapakse PS, et al. Population burden of betel quid abuse and its relation to oral premalignant disorders in South, Southeast, and East Asia: an Asian Betel-quid Consortium Study. Am J Public Health 2012 Mar;102(3):e17-e24.
- 47. Okamoto SK, Helm S, Delp JA, Stone K, Dinson A-L, Stetkiewicz J. A community stakeholder analysis of drug resistance strategies of rural native Hawaiian youth. J Prim Prev 2011 Aug;32(3-4):185-193.
- 48. Han Y, Lin V, Wu F, Hser Y-I. Gender comparisons among Asian American and Pacific Islander patients in drug dependency treatment. Subst Use Misuse 2016 May;51(6):752-762.
- 49. Okamoto SK, Pel S, Helm S, Valdez JK. Gender differences in the use of drug resistance strategies: an analysis of rural Asian/Pacific Islander youth. Health Promot Pract 2014 Jul;15(4):568-574.
- 50. Wu L-T, Blazer DG, Swartz MS, Burchett B, Brady KT, Workgroup NA; NIDA AAPI Workgroup. Illicit and nonmedical drug use among Asian Americans, Native Hawaiians/Pacific Islanders, and mixed-race individuals. Drug Alcohol Depend 2013 Dec;133(2):360-367.
- Rasmus S, Allen J, Connor W, Freeman W, Board NTCA, Skewes M. Native transformations in the Pacific Northwest: a strength-based model of protection against substance use disorder. American Indian and Alaska native mental health research. 2016;23(3):158-186.
- 52. Parackal SM, Parackal MK, Harraway JA. Warning labels on alcohol containers as a source of information on alcohol consumption in pregnancy among New Zealand women. Int J Drug Policy 2010 Jul;21(4):302-305.
- 53. Eubanks Fleming CJ. Do as I say, not as I do? An examination of the relationship between partner behaviors and help seeking for alcohol related issues. Subst Use Misuse 2016 Jul;51(9):1185-1194.
- 54. Suaalii-Sauni T, Samu KS, Dunbar L, Pulford J, Wheeler A. A qualitative investigation into key cultural factors that support abstinence or responsible drinking amongst some Pacific youth living in New Zealand. Harm Reduct J 2012 Aug;9(1):36.
- 55. Teevale T, Robinson E, Duffy S, Utter J, Nosa V, Clark T, et al. Binge drinking and alcohol-related behaviours amongst Pacific youth: a national survey of secondary school students. N Z Med J 2012 Mar;125(1352):60-70.
- 56. Operario D, Choi K-H, Chu PL, McFarland W, Secura GM, Behel S, et al. Prevalence and correlates of substance use among young Asian Pacific Islander men who have sex with men. Prev Sci 2006 Mar;7(1):19-29.
- 57. Operario D, Nemoto T. Sexual risk behavior and substance use among a sample of Asian Pacific Islander transgendered women. AIDS Educ Prev 2005 Oct;17(5):430-443.
- 58. Goebert D, Park C, Nishimura S. The co-occurrence of alcohol abuse in alcohol dependence among a treatment sample of Asian/Pacific Islanders. Addict Disord Their Treat 2004 Sep;61(9):891-896.