Tracheostomy is one of the most frequent procedures performed in head and neck surgery and is considered a safe procedure to achieve sufficient ventilation for a patient who suffers from an obstruction of the upper airway or who needs long-term ventilation. However, it can be associated with serious late complications including tracheostomal stenosis, erosion of the innominate artery, and tracheoesophageal fistulas. Fracturing and hence aspiration of the tracheostomy tube in the tracheobronchial tree is a rare late complication, which can be potentially life-threatening. Reported cases of a fractured tracheostomy tube presenting as foreign bodies in the tracheobronchial tree are rare and have not been commonly published in the medical literature. Therefore, we share our unique case of right-sided pneumonia due to a migrated fractured metallic tracheostomy tube after 14 years of placement and its management.1
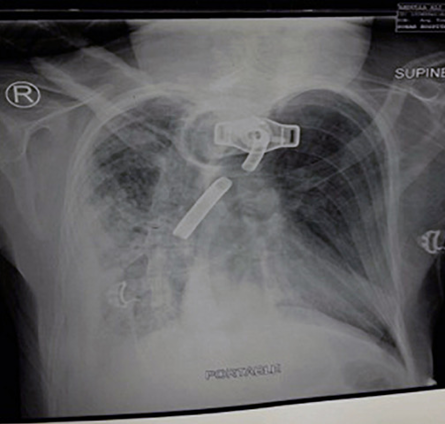
Figure 1: Posterior-anterior chest X-ray showing the fractured flange of the tracheostomy tube in the main bronchus on the right side.
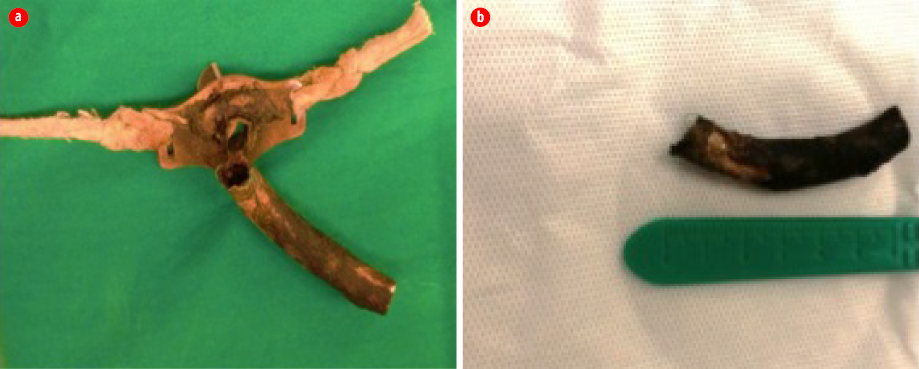
Figure 2: Photographs showing the (a) broken inner tube of the metallic tracheostomy tube, and (b) the broken inner segment of the tube.
Case report
Our patient was a 29-year-old man with a known case of leukodystrophy, and with a tracheostomy tube in place since 2002. He presented to the emergency department of Sohar Hospital in 2016 with high-grade fever, respiratory distress, and an altered level of consciousness. His primary examination showed low oxygen saturation (82%), tachypnea, and tachycardia (respiratory rate 30/minute, heart rate 160/minute, and body temperature 39.4 °C) that were corrected primarily by oxygen supply (100%, 10 L/minute) through the tracheostomy tube (Jackson’s metallic double-lumen tube). A chest examination revealed reduced air entry in the right lung; therefore, a chest X-ray was performed immediately. This revealed a metallic foreign body stricture, possibly a fractured flange from the tracheostomy tube, in the right main bronchus with pneumatic opacification patch [Figure 1]. After obtaining consent from his father, and after anesthesia review, he was taken for an emergency bronchoscopy for foreign body removal and replacement of the tracheostomy tube.
Given the kyphosis of the patient, spine positioning in the classic ‘sniffing’ position was difficult. The operating position was achieved by placing compensatory rolls below the left side of the patient’s chest. A rigid ventilating bronchoscope (size 8.5 mm, length 43 cm; Karl Storz, Tuttlingen, Germany) was used for airway access during the procedure. After the bronchoscope was introduced into the tracheal lumen, the foreign body was seen in the right bronchus. It was a fractured curved piece of the outer lumen of a Jackson metallic double-lumen tube [Figure 2]. Removal was challenging for the surgeon and anesthetist due to fibrosis and ridges around the tube, but the foreign body was successfully removed and eventually the airway was secured with a new tracheostomy tube (Portex cuffed tube no. 7; ID, 7 mm; OD, 9.7 mm; Smiths Medical UK, Luton, UK). The patient was then admitted to the intensive care unit for further management of pneumonia.
Discussion
Although tracheostomy is considered a relatively safe procedure, it has complications that can be divided into early (< 1 week as the stoma takes around one week to mature) or late complications. Complications can occur after open surgical tracheostomy or percutaneous tracheostomy via percutaneous dilational tracheostomy. Early complications include bleeding (5.7%), infection (6.6%), tracheostomy tube obstruction, and early extubation.2 On the other hand, the reported incidence of late complications following tracheostomy tube placement is approximately 65%.3 These late complications can be subdivided in relation to the stoma into suprastomal (subglottic stenosis, tracheal stenosis, and granulation tissue formation), stomal (stomal stenosis and granulation tissue formation), or infrastomal (tracheal stenosis, tracheomalacia, tracheoesophageal, and tracheoinnominate fistulas).3–5
Fracturing and hence aspiration of the tracheostomy tube in the tracheobronchial tree is considered a rare late complication of tracheostomy. Bassoe and Boe were the first to report this in the literature in 1960.6 This rare complication was also reported with various tracheostomy tube materials such as silver, sterling silver, stainless steel, polyvinylchloride, and silicone.7 Different contributing factors for weakening and subsequent fracturing of the tracheostomy tubes have been described including repeated boiling and sterilization of tubes, especially with bleaching solutions.8 Repeated mechanical stresses due to frequent use and out-and-down movements are likely to be greatest in the tube-flange junction area, especially in the presence of tracheostomy stenosis.8
Another important contributing factor is the corrosive action of alkaline bronchial secretions which accumulate around the tracheostomy tube and are reported to be more significant with prolonged use of the tracheostomy tube, particularly with metal tubes such as in our case.1,9 In a minority of cases, the tube fractures within hours to days of insertion, most likely due to manufacturing defects.1,9
In our case, the tracheostomy tube was used for 14 years before fracturing. In the literature, fracturing of the tracheostomy tube after placement was reported after periods varying from five days to 22 years.3 As in our case, the most common site of fracturing of a metallic tracheostomy tube is its neck, which is the weak point that is prone to be damaged by repeated mechanical stress.10–12
The best way to minimize this complication is to properly train the patient’s family at home about the methods of tracheostomy care and to adequately stress the importance of regular follow-up to check for any changes in the tracheostomy tube. In addition, conducting workshops and courses on tracheostomy care for health care professionals can improve awareness and early detection of such an event. On the other hand, the surgical team should check for any manufacturing defects or signs of wear and tear before inserting the tube and provide feedback to the manufacturing company.
Conclusion
A fractured tracheostomy tube with aspiration is a rare cause of respiratory distress and death, but early diagnosis and the presence of a skillful otolaryngological surgeon can lead to successful management. Proper education aimed at increasing awareness about tracheostomy tube care among caregivers and family members is important to reduce the morbidity and mortality associated with the tracheostomy tube.
Disclosure
The authors declared no conflicts of interest.
Acknowledgements
We would like to thank the ENT, anesthesia, and medicine departments in Sohar Hospital for their help and support in editing this manuscript and for management of this case. We would also like to extend our deepest thanks to the patient’s family members for their cooperation.
references
- 1. Parida PK, Kalaiarasi R, Gopalakrishnan S, Saxena SK. Fractured and migrated tracheostomy tube in the tracheobronchial tree. Int J Pediatr Otorhinolaryngol 2014 Sep;78(9):1472-1475.
- 2. Delaney A, Bagshaw SM, Nalos M. Percutaneous dilatational tracheostomy versus surgical tracheostomy in critically ill patients: a systematic review and meta-analysis. Crit Care 2006;10(2):R55.
- 3. Agarwal N, Agarwal R. Fractured tracheostomy tube migrating into the tracheobronchial tree: a rare complication. Indian J Chest Dis Allied Sci 2011 Apr-Jun;53(2):111-112.
- 4. Streitz JM Jr, Shapshay SM. Airway injury after tracheotomy and endotracheal intubation. Surg Clin North Am 1991 Dec;71(6):1211-1230.
- 5. Pawar MS, Suri N. A rare early complication of tracheostomy. Oman Med J 2011 Jan;26(1):48-49.
- 6. Bassoe HH, Boe J. Broken tracheotomy tube as a foreign body. Lancet 1960 May;1(7132):1006-1007.
- 7. Sullivan MJ, Hom DB, Passamani PP, DiPietro MA. An unusual complication of tracheostomy. Arch Otolaryngol Head Neck Surg 1987 Feb;113(2):198-199.
- 8. Okafor BC. Fracture of tracheostomy tubes. Pathogenesis and prevention. J Laryngol Otol 1983 Aug;97(8):771-774.
- 9. White AC, Kher S, O’Connor HH. When to change a tracheostomy tube. Respir Care 2010 Aug;55(8):1069-1075.
- 10. Piromchai P, Lertchanaruengrit P, Vatanasapt P, Ratanaanekchai T, Thanaviratananich S. Fractured metallic tracheostomy tube in a child: a case report and review of the literature. J Med Case Rep 2010 Aug;4:234.
- 11. Sue RD, Susanto I. Long-term complications of artificial airways. Clin Chest Med 2003 Sep;24(3):457-471.
- 12. Ambasta S, Gupta SL, Rajiv G, Swaminathan S. Fractured tracheostomy tube posted for bronchoscopic removal: An anesthetic challenge. Saudi J Anaesth 2018 Jan-Mar;12(1):142-143.