|
Introduction
Traumatic panniculitis refers to changes in the subcutaneous fat related to physical or chemical agents.1 The clinical picture of traumatic panniculitis is nonspecific. Cutaneous lesions are indurated, warm, red, subcutaneous plaques or nodules not necessary related to the intensity of the injury.2 The histological picture includes fat microcysts surrounded by histiocytes, collections of foam cells and inflammatory cells. Late lesions may show fibrosis, lipomembranous changes, or dystrophic calcific deposits.3 Traumatic panniculitis is usually a self-limiting disorder and requires only symptomatic treatment.
Case Report
A 24-yr-old male presented with a swelling of the anterior aspect of the right thigh of 4 years duration which developed following a cricket ball injury. He reported having developed a hematoma initially, which resolved completely before this swelling developed. There were no symptoms as such but for cosmesis. Examination revealed a boggy swelling on the antero-medial aspect of the right thigh measuring approximately 7x5 cm in the subcutaneous plane that was mobile and nontender. The skin was pigmented and seemed to be involved, as it could not be pinched up from the swelling (Fig. 1). Clinically, this felt like a peripheral neurofibromatosis. A CT scan of the right thigh was performed which revealed an ill defined area of fat attenuation separated by septae, measuring approximately 9.8x3.9x7.7 cm, in the subcutaneous tissues of the antero-medial aspect of the mid thigh with associated skin thickening. The visualized muscles and the right femur were normal (Fig. 2). These features were consistent with the diagnosis of traumatic panniculitis. As the patient denied a biopsy for histopathological diagnosis, he was been kept under follow-up.

Figure 1: Traumatic panniculitis of right thigh.
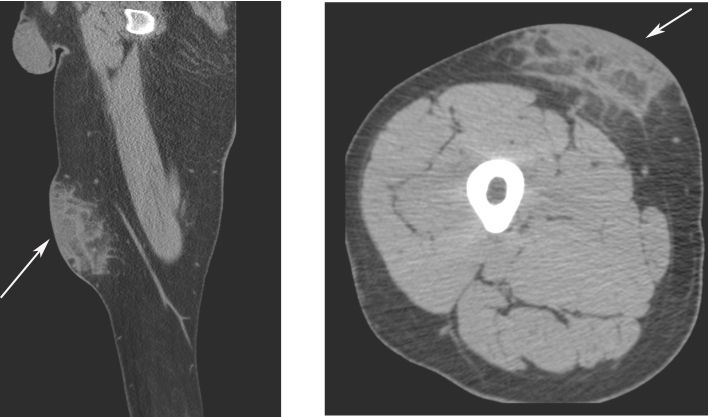
Figure 2: CT right thigh showing area of fat attenuation separated
Discussion
Traumatic panniculitis includes changes in the subcutaneous fat secondary to both physical and chemical agents. The causesof physical injuries are trauma, cold and electricity.1 In general; the intensity of traumatic injury is not necessarily related to the development or the intensity of the cutaneous lesions. History of trauma helps in the diagnosis, although often the antecedent is minor or even unnoticed.2 The clinical picture of traumatic panniculitis is nonspecific, although the clinical distribution of the lesions may suggest an exogenous origin. The cutaneous lesions appear as indurated, warm, red, subcutaneous plaques or nodules and could be confused with neurofibromatosis.1,3 In cases of extensive liquefaction it may be discharged through superficial wound. The histological picture of traumatic panniculitis is not specific, although late lesions are quite characteristic. Early lesions are characterized by an inflammatory infiltrate composed of lymphocytes and macrophages starting around vessels and septa.3 Traumatic panniculitis is usually a self-limiting disorder and requires only symptomatic relief. Some patients may require surgical treatment of local complications (erythema, indurated fibrous masses or large cysts or nodules).3 by septae (arrows).
Conclusion
Cutaneous panniculitis is a rare entity, which needs to be confirmed by a tissue biopsy to rule out other skin and subcutaneous lesions. As this is a self-limiting condition, a conservative approach can be followed. Surgical intervention is required only in patients with intractable pain and complications.
Acknowledgements
The authors reported no conflict of interest and no funding was received on this work.
|