
Blood Lead Level Among Fuel Station Workers
Laith Abdulmajeed Al-Rudainy
doi:10.5001/omj.2010.58
ABSTRACT
Objectives: This study aims to determine the level of lead in blood of fuel station workers and in a group of people not occupationally exposed to lead
Methods: 53 control subjects with low risk lead exposure and 45 fuel station workers comprising the study group were included in this study in a period from September 2008 to December 2009. Blood samples were collected and analyzed for each subject by Lead Care Blood Testing System. The average blood lead levels of each group were compared using the independent sample (Mann – Whitney U) test.
Results: The median (range) 14.1 (7.5–56) µg/dl concentration of lead in the blood of fuel stations workers was significantly higher than the median (range) 6.5 (4.0–1.6) µg/dl concentration of lead in the blood of the control group (p< 0.001).The results obtained also showed that the values of blood lead levels in many workers were higher than action and upper limits acceptable for adults. In fuel station workers, the duration of exposure to leaded fuel was significantly correlated with the blood lead level.
Conclusions: Occupational exposure to lead is prevalent among many fuel station workers in Basrah. A policy action to improve working conditions and to phase out the use of leaded gasoline is recommended.
From the Department of Community Medicine, College of Medicine, University of Basrah, Basrah, Iraq.
Received: 25 Apr 2010
Accepted: 27 Jun 2010
Address correspondence and reprint request to: Dr. Laith Abdulmajeed Alrudainy, Department of Community Medicine, College of Medicine, University of Basrah, Basrah, Iraq.
E-mail: Alrudainy_laith@yahoo.com
INTRODUCTION
Lead is one of the oldest known and most widely studied occupational and environmental toxins.1 Although USA and the European Union have banned lead as an additive to consumer fuel for road-going vehicles, lead continues to be used in petrol in many countries in the Middle East including Iraq.2 Petrol station workers are constantly in contact with leaded benzene and gasoline during their daily lives. Lead in the workplace comes from emissions in the form of fine particles that are inhaled and absorbed through the lungs, by ingestion, and through dermal exposure.3 Recent research has demonstrated that clinical or subclinical toxic effects can occur below the limit of 50 µg/dl in the whole blood.4
The World Health Organization (WHO) permitted 40 µg/dl as a higher limit of blood lead level for adults in the general population.5 In 1991, the Centres for Disease Control (CDC) lowered the action limit for whole blood lead levels to 35 mcg/dL, as an action limit of blood lead level for adults.6 Therefore, determining and controlling lead exposure among the risk workers is very important. This is a case control study conducted to estimates the proportion of workers with blood lead levels that trigger the clinical and subclinical toxic effects, and to determine the difference of blood lead level between the non-exposed subjects and fuel stations workers.
METHODS
The research protocol was approved by the scientific committee in the Medical College, University of Basrah at December 2008. Individuals gave oral consent to give blood samples and answer a questionnaire.
A total of 98 subjects were included in this study. The study group was comprised of 45 subjects who were fuel stations workers and represented approximately 92% of workers in these two stations after the application of inclusion and exclusion criteria. The settings were two fuel stations selected randomly from the six fuel stations that supply leaded benzene and gasoline in the centre of Basrah city. The average work hours per week were 72 + 4.7 hours and most of the workers have been working for at least 2 years. The second group included 53 subjects who comprised the control group with low risk of lead exposure.
All were farmers from a rural agricultural area within the centre of Basrah city without any nearby factories or fuel stations, selected by non-random quota sampling, and distributed by region of residence according to the statistics from agriculture association in Basrah. The reason for choosing these controls was that all of them were drained from the same residential and socioeconomic level as study subjects. Also, the controls were matched with cases for age (within 5 years range). In every region, people were approached at their work site. The questionnaire was translated to the local language. All subjects were interviewed for possible exposure to lead and none reported any. The blood samples were collected for laboratory analysis from each subject. The refusal rate was 0%. General characteristics of subjects were examined by an interview using a questionnaire. The exclusion criterion included subjects unwilling to participate in the study, age below 15 or above 65 years, resident outside centre of Basrah city, and who reported chronic diseases.
The blood samples were collected by the author. A sufficient whole blood sample was obtained from a skin-puncture using a finger stick after thorough washing of the hand to avoid contamination. The lateral side of the middle finger was used. A special heparinized capillary tube that allows collecting exactly (50 µl) of whole blood was used. For each test, the exact 50 µl whole blood sample was dispensed from the capillary tube into the treatment reagent tube using special plungers.
Analysis was conducted at the Environmental Health Laboratory in Basrah Medical College by the same technician. Blood lead level was measured using Lead Care Blood Testing System and Lead Care Blood Test Kits. This system relies on electrochemistry and a sensor to detect lead in the whole blood where the kit is specific for quantitative measurement of lead in fresh whole blood specimens only. The performance of the Lead Care System was checked on each batch run using appropriate quality control materials, i.e. both high and low known readings lead standards by Lead Care as well. Results obtained on control samples were within the expected range. The performance of the Lead Care System was calibrated after every 20 samples with atomic absorption spectrophotometer blood lead standard materials. The precision (the coefficient of variation) ranged from 8% for concentrations between 10 and 30 μg/dl to 1% for higher concentrations.
The data was analyzed using the SPSS, version 15 software. Statistical analysis included descriptive statistics (frequency tables) and Spearmen correlation coefficient analysis. Median and range of blood lead levels in both groups were calculated. The average blood lead levels of each group were compared using the two-sided p-value of independent sample (Mann – Whitney U) test with level p≤ 0.05 considered statistically significant.7
RESULTS
The study population comprised of males from the same ethnicity. There were no significant difference in the other baseline characteristics between the two groups, (Table 1). The distribution of blood lead levels among control subjects and fuel stations workers is shown in Table 2. The median (range) blood lead level in the control group was 6.5 (4.0 – 11.6) μg/dl.
Table 1: Sociodemographic characteristics in control and fuel stations workers.
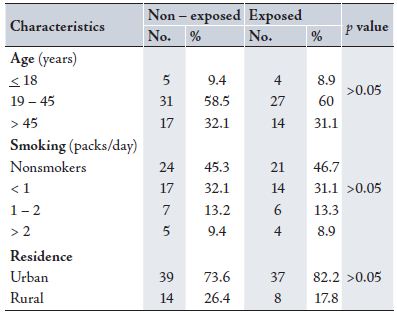
Table 2: Distribution of Blood lead levels in control and fuel stations workers.
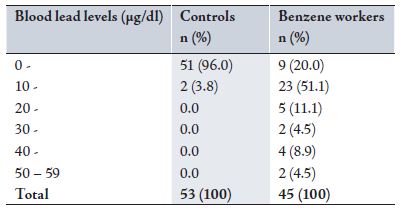
While the median (range) blood lead level in the fuel stations workers was 14.1 (7.5 – 56.0) μg/dl. There was a highly significant difference between the two groups (p<0.001). (Table 3)
The Spearman correlation between the duration of exposure to leaded fuel and the blood lead level in fuel stations workers was performed. A strong positive correlation was found (r= 0.947) which was highly significant (p<0.001), as shown in Fig. 1. However, there was no significant correlation between age and blood lead levels in fuel station workers in this study (r=0.149, p>0.05).
Table 3: Blood lead levels in μg/dl among control and fuel stations workers.
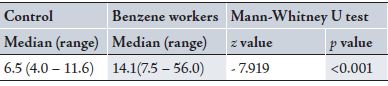
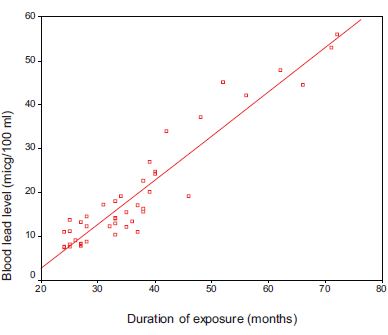
Figure 1. Correlation between duration of exposure to leaded fuel and blood lead level.
All the demographic factors (expected confounders) which were studied in this paper were not statistically associated with the dependent variable (exposed and non-exposed groups to leaded fuel). Therefore, there was no need to conduct a multivariate statistical analysis (logistic or multiple linear regression). Subjects who were found with high blood lead level were advised on the importance of medical examination and other protective measures, however the advice is not reported in this paper since this is not an interventional study. Nonetheless, recommendations, are given in terms of the importance of health promotion and health education for the workers.
DISCUSSION
Lead is an important toxic substance. Its toxicity can cause aberrant function of multiple organs. Therefore, monitoring its toxicity is very important. Blood lead level determination has presently been accepted as the most reliable biomarker.8 An important limitation of the study was the sample size. The cost and the time needed for measuring lead in blood of study population affected the ability to increase the sample size. The results in the current study indicate that blood lead levels are significantly higher among fuel stations workers compared to the control group.
The results obtained also show that values of blood lead levels in many workers were higher than the upper and action limits of lead in the blood for adults. Two scenarios could have been operating in the study workers which may have resulted in elevated blood lead. Firstly, benzene workers neglect to use facemasks during work and this significantly increases blood lead levels due to the inhalation of airborne lead. Secondly, they neglect to use the protective cloths and to wash their body after work and this increases blood lead levels due to dermal absorption.9 This result is consistent with the findings of other studies in Baghdad and Beirut, which supports the conclusion that exposure to leaded benzene and gasoline elevated blood lead level among fuel stations workers.10,11 In another study conducted in 1997 in Basrah, the blood lead level among 62 petrol station workers was found to be within normal limits.12 Instability of workers in their job for a long period of time may explain this reduction in blood lead level in those workers.12
In the current study, the parameter which showed significant relation with blood lead levels included duration of exposure in work place. This was similar to the result from other countries, which found that higher blood lead level is associated with longer duration of lead exposure.13,14
Various control measures are needed to decrease blood lead levels in fuel station workers. Training and health education are thought to be a fundamental tool in the prevention of occupational diseases.15 Motivation programs will be effective to increase job safety by spontaneous safety analysis by the workers themselves.16 Respiratory protective equipment and protective clothing should be used to supplement the engineering measures.
Also, personal hygienic behavior and life habits such as eating, drinking and smoking in different workplace are also thought to be important.17 Furthermore, phasing lead out of gasoline makes a very important contribution to avoid the negative impact of high blood lead levels on the health of workers. Finally, periodic screening for blood lead levels among all fuel station workers, with follow-up assessment, treatment, and monitoring for those with elevated blood lead levels.
CONCLUSION
The results from this study revealed a prevalence of elevated blood lead levels among many fuel stations workers in Basrah, and it is higher than the limit permitted by the World Health Organization. Therefore, it is important to recognize that in addition to research, good health promotion and protection measures should be taken for fuel stations workers in Basrah.
ACKNOWLEDGEMENTS
The author reported no conflict of interest and no funding was received on this work.
-
Gidlow DA. Lead toxicity. Occupational Medicine 2004; 54:76-81.
-
Gordon B, Mackay R, Rehfuess E. Inheriting the world: The Atlas of Children’s Health and the Environment. Brighton, US: WHO, 2004.
-
Herman DS, Geraldine M, Scott CC, Venkatesh T. Health hazards by lead exposure: evaluation using ASV and XRF. Toxicology and Industrial Health 2006; 22 (6):249-254.
-
Tak SW, Roscoe RJ, Walter AW, Sestito JJ, Sussell AL, Calvert GM. Characteristics of US workers whose blood lead levels trigger the medical removal protection provision, and conformity with biological monitoring requirements, 2003-2005. American Journal of Industrial Medicine 2008; 51(9):691-700.
-
Recommended health-based limits in occupational exposure to heavy metals. Report of a WHO Study Group. Geneva, Switzerland, 1980 (WHO Technical Report Series, No. 647).
-
CDC (1991) Weekly Morbidity Reports, Oct. 1991, Centres for Disease Control, U.S. Dept. of Health and Human Services, Atlanta.
-
Thompson WD. Statistical analysis of case-control studies. Epidemiological Review 1994; 16(1):33-50.
-
Barbosa JF, Tanus-Santos JE, Gerlach RF, Parsons PJ. A Critical Review of Biomarkers Used for Monitoring Human Exposure to Lead: Advantages, Limitations, and Future Needs. Environmental Health Perspectives 2005; 113(12):1669-1674.
-
Moline JM, Landrigan. Lead. In: Rosenstock L, Cullen MR, Brodkin CA, Redlich CA. Textbook of occupational and environmental medicine. Second ed. Philadelphia: Elsevier Saunders, 2005; 986-977.
-
Hikmet J, Dhia JA, Saad IA, Qasim IV. Lead absorption in petrol filling station workers in Baghdad city. J Fac Med Baghdad 1987; 29(1):95-102.
-
Nuwayhid I, McPhaul K, Bu-Khuzam R, Duh SH, Christenson RH, Keogh JP. Determinants of elevated blood lead levels among working men in Greater Beirut. J Med Liban. 2001; 49(3):132-139.
-
Mahdi JK. Levels of heavy metals in seledted risk groups in Basrh. MSc thesis, University of Basrah, 1997.
-
DE Medinilla J, Espigares M. Environmental and Biological Monitoring of Workers Exposed to Inorganic Lead. Occupational Medicine 1991; 41(3):107-112.
-
Mason H, Williams N. The decay of blood lead levels in workers suspended under the control of lead at work regulations. Occupational Medicine 2005; 55(5):371-374.
-
Porru S, Donato F, Apostoli P, Coniglio L, Duca P, Alessio L. The utility of health education among lead workers: the experience of one program. Am J Ind Med 1993; 23 (3): 473-81.
-
Maples TW, Jacoby JA, Johnson DE, Terhaar GL, Buckingham FM. Effectiveness of employee training and motivation programs in reducing exposure to inorganic lead and lead alkyls. Am Ind Hyg Assoc J 1982; 43 (9):692-694.
-
Lormphongs S, Miyashita K, Morioka I, Chaikittiporn Ch, Miyai N, Yamamoto H. Lead Exposure and Blood Lead Level of Workers in a Battery Manufacturing Plant in Thailand. Industrial Health 2003; 41(4):348-353.
How to cite this article
Al-Rudainy LA. Blood Lead Level Among Fuel Station Workers. OMJ 2010 July; 25(3):208-211.
How to cite this URL
Al-Rudainy LA. Blood Lead Level Among Fuel Station Workers. OMJ [Online] 2010 July; 25(3):208-211. Available at http://www.omjournal.org/OriginalArticles/FullText/201007/FT_BloodLeadLevelAmong.html.