
The Prevalence of Congenital Malformations and its
Correlation with Consanguineous Marriages
Naeimeh Tayebi,1 Katayon Yazdani,2 Nazila Naghshin2
Tayebi N, et al. OMJ. 25, 37-40 (2010); doi:10.5001/omj.2010.9
ABSTRACT
Objectives: Consanguinity has been a long standing social habit among some Iranians. This study is aimed at determining the role of consanguinity on congenital malformations and the correlation of inbreeding coefficient with anomalies.
Methods: In this cross-sectional study, all the newborns who were born during 9 months period from April to December 2008. (n=1195) at Shahid Sadoughi hospital, Yazd, Iran were studied.
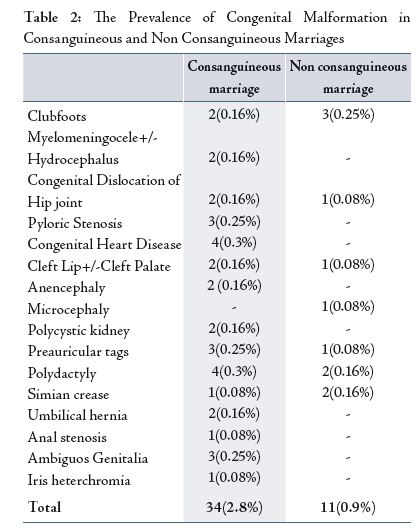
Results: From 1195 neonates, 300 (25%) were from consanguineous marriages and 895 (75%) were from non-familial marriages. From 45 cases with anomalies, 34 (2.8%) cases were from familial marriages, while only 11 (0.9 %) cases were from non-familial marriages. There was a significant correlation between parental marriages and the prevalence of anomaly (p=0.018).
Conclusion: The prevalence of congenital anomalies was mostly observed in consanguineous marriages compared to non consanguineous marriages.
From the 1Department of Genetics, Genetic Research Center, Welfare organization, Yazd, Iran, 2Department of Obstetric & Gynecology, Shahid Sadoughi University, Yazd, Iran.
Received: 13 Nov 2009
Accepted: 02 Jan 2010
Address correspondence and reprint requests to: Dr. Naeimeh Tayebi, 1Department of Genetics, Genetic Research Center, Welfare organization, Yazd, Iran
E-mail: ntayebi@yahoo.com
INTRODUCTION
While infections and malnutrition are the dominant causes of infant morbidity and mortality in the poorer countries, in the developed countries these causes are cancer, accidents and congenital malformations.1,2,3
Congenital malformation (CM) began to emerge as one of the major childhood health problems and it refers to any abnormality, whether genetic or not, which is present at birth. Treatment and rehabilitation of children with CM is costly and complete recovery is usually impossible.4
The etiology of CM is genetic (30-40%) and environmental (5 to 10%). Among the genetic etiology, chromosomal abnormality constitutes 6%, single gene disorders 25% and multifactorial 20-30%; however, for nearly 50% of CM, the cause is yet to be known.5
In one study, the prevalence of CM was 3% for single major anomaly and 0.7% for multiple major anomalies. It has also been shown that 12.3-32% of deaths that have occured during the perinatal period are related to congenital anomalies.6
Consanguineous marriages have been described as an important factor contributing to increased congenital malformations.7A consanguineous marriage can be characterized by the degree of relatedness between the spouses: first cousins, double first cousins, half first cousins, first cousins once removed, second cousins, second cousins once removed and third cousins. Genetic effects of consanguinity can be traced to the fact that the inbred individual may carry two copies of a gene that was present in a single copy in the common ancestor of his/her consanguineous parents. A recessive gene may thus come to light for the first time in an inbred descendant after having remained hidden for generations. For this reason, consanguinity influences the incidence of some inherited diseases.8
Estimated consanguinity ratios in different parts of Iran ranged from 30 to 85%.7 In another country, such as the province of Antalya, Turkey, there has been a significant increase in the incidence of consanguineous marriages, approximately 40.7% between populations and the results showed that the most frequent type of marriage was between first cousins.9 Because of high consanguinity rates within the Muslim population, the incidence of CM in Islamic countries is between 10 to 45%.10 In developed countries such as the United Kingdom, CM account for a substantial proportion (26-34%) of perinatal mortality.11 Also, the prevalence of congenital anomalies in Denmark is approximately 3%.12
This study aims to determine the role of consanguinity on CM and the correlation of inbreeding coefficient with anomalies in Shahid Sadoughi hospital, Yazd, Iran.
METHODS
This is a descriptive, cross-sectional study with consecutive sampling of newborns babies, who had been delivered at Shahid-Sadoughi hospital, Yazd, Iran during a 9 months period from April to December 2008. All newborns who had been delivered in the hospital during the investigation were examined and screened for congenital malformations by pediatricians. Data collection was performed by means of a structured model which was comprised of two parts, similar to another study by Tootonchi.13
During the first part, recorded variables including maternal and paternal age, method of delivery, number of births, stillbirth and miscarriage, gravidity (defined as the number of times a woman has been pregnant), parity (defined as the number of times she has given birth to a fetus with a gestational age of 24 weeks or more, regardless of whether the child was born alive or stillborn), history of infertility (defined in specific terms as the failure to conceive after a year of regular intercourse without contraception), history of CM in other offspring and members of their family, and parental consanguinity were obtained by interviewing the neonates’ mothers. Also, the inbreeding coefficient (F) was calculated according to Hardy-Weinberg equilibrium. The method for the calculation of the inbreeding coefficient for an individual was expressed as; (1/2) (n1+n2+1), where n1 and n2 are the numbers of generations separating the individuals in the consanguineous mating from their common ancestor.14
The second part was about neonatal characteristics including sex, existence of congenital malformation and the type of malformation. The type of birth defects was classified by the diagnostic standardization of CM from the international classification of disease (ICD-10) codes. The data was analyzed using SPSS version 13. The rates of malformed newborns and malformations were compared using statistical T-test and the Chi-square tests. The level of significance was determined at p<0.05.
RESULTS
The mean maternal and paternal age was observed to be 25.86±5.4 and 30.07±9.6 respectively. 600(50.2%) and 595(49.8%) newborns were delivered by natural vaginal delivery (NVD) and cesarean section (CS) respectively.
From 1195, 300(25%) of the newborns were from consanguineous marriages, while 895(75%) were from non consanguineous marriages. In this study, the most frequent type of marriage was between first cousins (n=256). In 25 (8.3%) cases, the marriage was between double first cousins and in 19(6.3%) of the cases, the marriages was between half first cousins, first cousins once removed. Of the 1195 studied group, the number of positive family history of CM in other offspring and other relatives was 23(1.9%) and 191(15.9%) respectively. Of the 1195 births, 1173(98.2%) were single births, 18(1.5%) were twin births and only 4(0.3%) were multiple births. The mean number of gravid was 2.08±1.3 and parity was 1.85±1.09. 31(2.6%) and 3(0.3%) of the women had experienced stillbirth once and twice respectively. Also, 143(12%), 36(3%) and 10(0.8%) had experienced miscarriages once, twice and more than two times respectively. 52(4.4%) women had a history of infertility during their lives.
During the 9 months period, 1195 newborns were delivered, among whom 567(47.4%) were males, 625(52.3%) females and 3(0.25%) with ambiguous genitalia. Out of these, 45 newborns were diagnosed with congenital malformations. The prevalence of CM in this sample was 3.76% (23 males, 19 females, 3 with ambiguous genitalia). Therefore, there was no statistical difference between the rate of congenital malformations and newborn’s gender (p=0.38).
Table 1 shows the ICD-10 classification of the different types of congenital malformations. The prevalence of CM in consanguineous and non-consanguineous marriage is shown in Table 2. There was an increased rate of anomalies in the consanguineous group compared to the non-consanguineous group (p=0.018).

DISCUSSION
Most children who are born with major congenital anomalies and survive infancy are affected physically, mentally or socially and can be at increased risk of morbidity due to various health disorders.15 While the prevalence of congenital anomalies at birth in developed countries is reported to be between 3-5%, those reported in Taiwan are said to be approximately 4.3%, 7.92% reported for the United Arab Emirates, 2.46% for Oman, 2.7% for Bahrain, and 3.6% for India.16,17,18, 19,20
However, studies that investigated the number of all infants who were born with a congenital anomaly in some cities of Iran such as Tehran and Gorgan found a birth prevalence of 2.3% and 1.01% respectively.21,22 Similarly, the results from this study showed that the overall prevalence of congenital malformation among the newborns who were born in Yazd, Iran, was 3.76%.
The frequency of malformations in this study was higher compared with other studies which have been conducted in Iran, this may be due to industrial pollution (air pollution created by factories or companies in the cities, and carbon monoxide from cars can produce a large percentage of these pollutants), environmental and chemical factors, nutritional status and habits (because of high cost in nutritional elements and low economic status of some individuals, some pregnant women can not get necessary vitamins during their pregnancy), high consanguinity marriage and etc.
In this study, the gender of the fetus did not affect the prevalence of CM, and both genders were equally distributed. These findings are consistent with Karbasi et al.23 and Biri et al.24 However, the results from this study were in contrast to those reported by Gorgan, where male newborns were more affected than females.22
Increased incidence of genetic malformations in the offspring of consanguineous couples most likely arises from the homozygous expression of recessive genes inherited from their common ancestors.8
In the present study, 25% of the parents with consanguinity. Also, the rate of malformation was 2.8% and 0.9% in consanguineous and non-consanguineous marriages respectively. Although, the prevalence of anomalies was higher in consanguineous marriages than non-consanguineous marriages, there was no significant difference between the inbreeding coefficient and the prevalence of anomalies. The results are in agreement with results from the study by Movahedian, and are in contrast with the results from the study by Nath et al.25,26
Mehrabi et al. (2205) showed that although the consanguinity for malformed patients was high, there was no significant relationship between malformation and the degree of relation of the parents.27 Also, in a study by Bromiker in Palestine, no statistically significant difference was found in the incidence of congenital malformation with the degrees of parents’ relation.10
CONCLUSION
In conclusion, consanguinity may play an important role in the high rates of malformation in children and must be taken into account for genetic counseling in Iran.
For a possible prevention, genetic counseling before marriage must be applied, not only for consanguineous couples but also for any couples that may have a family history of genetic disorders. Of course, currently suitable pre-marriage counseling services are provided by the Iran’s ministry of Health, but there is still room for improvement.
ACKNOWLEDGEMENTS
We would like to express sincere gratitude to Mr. Hossain Khodaee, Mahsa Tashakor for their outstanding support.
-
Asindi AA, Ibia EO, Udo JJ. Mortality pattern in Nigerian children in the 1980s. J Trop Med Hyg 1991 Jun; 94(3):152-155.
-
Behrnan RE. The Field of pediatrics. In: Nelson WE, Behrman RE and Kliegman RM, eds. Nelson Textbook of Pediatrics. 14th ed. Philadelphia: WB Saunders Co, 1992:1-5.
-
Forfar JO. Demography, vital statistics, and the pattern of disease in childhood. In: Campell AGM and McIntosh I, eds. Forfar and Arniel Textbook of pediatrics. 4th ed. London: Churchill Livingstone, 1992:1-17.
-
Turnpenny P, Ellard S. Emery’s Elements of Medical Genetics. 12th edition. Elsevier Churchill Livingstone, Edinburg, UK, 2005.
-
Rajangam S, Devi R. Consanguinity and chromosomal abnormality in mental retardation and or multiple congenital anomaly. J Anat Soc India 2007; 56 (2):30-33.
-
Aksoy F. Konjenital anomaliler: Tanimlama, Siniflama, terminoloji ve anomalili fetusun incelenmesi. (Congenital anomalies: description, classification, terminology and examination of fetus with congenital anomalies). Turk Patol Dergisi 2001; 17:57-62.
-
Sorouri A. Consanguineous marriage and congenital anomalies. First edition, Isfahan University of Medical Sciences, 1380:1-15.
-
Khlat M, Khoury M. Consanguinity and diseases: Demographic, Genetic, and epidemiologic perspectives. Epidemiologic reviews 1991; 13:28-30.
-
Alper ÖM, Erengin H, Manguo AE, Bilgen T, Çetin Z, Dedeo lu N, et al. Consanguineous marriages in the province of Antalya, Turkey. Annales deGénétique, 2004 Jun; 47(2):129-138.
-
Bromiker R, Baruch M. Association of parental consanguinity with congenital malformations among Arab newborns in Jerusalem. Clinical Genetics 2004; 66:63.
-
Young I, Clarke M. Lethal malformations and perinatal mortality: a 10- year review with comparison of ethnic differences. Br Med J 1987 Jul; 295:89-91.
-
Søgaard M, Vedsted-Jakobsen A. Consanguinity and congenital abnormalities. Ugeskr Laeger. 2003 Apr;165(18):1851-1855.
-
Tootonchi P. Easily identification congenital anomalies. Prevalence and risk factors. Acta Medica Iranica 2003; 41:15-19.
-
Bronya J.B. Keats and Stephanie L. Sherman. Population genetics. In: Emery and Rimoin’s principles and practice of medical genetics, eds. Rimoin DL, Connor J.M , Pyeritz RE and Korf BR. 4th edition. Elsevier Churchill Livingstone, Edinburg, UK, 2002: 425-438.
-
Correa-Villasenor A, Cragan J, Kucik J, O’leary L, et al. The metropolitan Atlanta congenital defects program: 35 years of birth defects surveillance at the centers for disease control and prevention. Birth Defects Res A Clin Mol Teratol 2003 Sep; 67(9):617-624.
-
Zlotogora J. Genetic disorders among Palestinian Arabs: effect of consanguinity. Am J Med Genet 1997 Feb; 68(4):472-475.
-
Al Hosani H, Salah M, Abu-Zeid H, Farag HM, Saade D. The National congenital anomalies register in the United Arab Emirates. East Mediterr Health J 2005 Jul; 11(4):690-699.
-
Sawardekar KP. Profile of major congenital malformations at Nizwa spital, Oman 10-year review. J Paediatr Child Health 2005 Jul; 41(7):323-330.
-
Al Arrayed SS.Epidemiology of congenital abnormalities in Bahrain. Mediterr Health J 1995; 1:248-252.
-
Verma M, Chhatwal J, Singh D. Congenital malformations: A retrospective study of 10,000 cases. Indian Pediatr 1991; 28:245-252.
-
Farhud DD, Walizadeh GHR, Kamali MS. Cngenital malformations and genetic diseases in Iranian infants. Hum Genet 1986 Dec; 74(4):382-385.
-
Golalipour M.J, Ahmadpour-Kacho M, Vakili MA. Congenital malformations at a referral hospital in Gorgan, Islamic Republic of Iran. East Mediterr Health J 2005; 11(4):707-715.
-
Akhavan Karbasi S, Golestan M, Fallah R, Mirnaseri F, Barkhordari K, Sadr M. Prevalence of congenital malformations. Acta Medica Iranica.2009; 47(2):149-153.
-
Biri A, Onan A, Korucuoglu U, Tiras B et al. Birth prevalence and distribution of congenital anomalies in a university hospital. PerinatolDergisi 2005; 13:86-90.
-
Movahedian A, Mosayebi Z, Yosofian S. The prevalence of congenital malformations in consanguineous and non consanguineous marriages. Feyz J 2005; 81:84-88.
-
Nath A, Patil C, Naik V.A. Prevalence of consanguineous marriages in a rural community and its effect on pregnancy outcome. Indian Journal of community Medicine 2004; 29(1):41-43.
-
Mehhrabi Kushki A, Zeyghami B. The effect of consanguineous marriage on congenital malformation. Journal of Research in Medical Sciences 2005:10(5):298-301.