
Control of Hypertension among Type II Diabetics
Kawther El-Shafie, Sayed Rizvi
El-Shafie K, et al. OMJ. 25, 32-36 (2010); doi:10.5001/omj.2010.8
ABSTRACT
Objectives: Numerous studies have confirmed the high prevalence of hypertension among type 2 diabetics, and that intensive hypertensive treatment is more beneficial to diabetics than non diabetics. The aim of this study is to assess blood pressure control in patients with type 2 diabetes mellitus and to study the types of antihypertensives used.
Methods: A retrospective study was conducted on hypertensive diabetics followed at a health center in Oman within a year. Patients’ age, sex, duration of diabetes, hypertension and the type of antihypertensive used were noted. Patients were classified according to the degree of systolic and diastolic BP control into 4 groups.
Results: 210 patients with a mean age of 53.7±9.1 years were included with a 2:5 male to female ratio. The mean duration of diabetes was found to be 9 years and 7 years for hypertension. 10% of the subjects were in the systolic group I, 23% in group II, 23% in group III and 41% in group IV. While 56% were in diastolic group I, 19% in group II, 16% in group III, and 7% in group IV. Angiotensin converting enzyme-inhibitors (ACE) were used in 50% of the subjects followed by a combination of angiotensin receptor blockers (ARB) with diuretics in 40%. B blockers were used in 38% of the patients. Calcium channel blockers were used in 18% , while diuretics were used in 16% of the patients.
Conclusion: Only 30% of the BP of the hypertensive diabetics met the recommended BP for diabetes. More effort should be dedicated to control the BP in diabetics. Physicians should be careful in the selection of hypertensive medications, because in some combinations, they are not useful.
From the Department of FAMCO, Sultan Qaboos University, Muscat, Sultanate of Oman.
Received: 07 Nov 2009
Accepted: 15 Dec 2009
Address correspondence and reprint request to: Dr Kawther El-Shafie, Department of FAMCO, Sultan Qaboos University, Muscat, Sultanate of Oman.
E-mail: kawther@squ.edu.om
INTRODUCTION
Hypertension in patients with diabetes is a well recognized cardiovascular risk factor.1 According to the intervention studies, the benefit of its treatment is evidence based.2,3 Recently the 7th Report of the Joint National Committee on prevention, detection, evaluation and treatment of high blood pressure (JNC 7) concluded that BP measurement in diabetic patients should be 130/80 mm Hg or less.4 Primary healthcare physicians play a very important role in treating hypertensive patients, as most of them are being followed up at primary healthcare clinics.5
Data from the recent United Kingdom Prospective Diabetes Study (UKPDS) hypertension study, demonstrated that aggressive lowering of diastolic blood pressure (BP) in diabetes to levels < 85 mm Hg and 80 mm Hg, were accompanied by a reduction of macrovascular events by one third and one half.2 The aim of this study work is to determine the degree of BP control in hypertensive diabetics and to study the appropriate types of antihypertensive agents used to control the BP.
METHODS
This study was conducted at a Primary Health Care Clinic at Sultan Qaboos University Hospital (SQUH) (FAMCO clinic), Oman. The diabetic clinic is specialized in the management and follow ups of diabetic patients. This is a retrospective study of medical records of type 2 diabetic patients seen at the clinic during the period of June 2006-July 2007. Hypertension was diagnosed as blood pressure >140/90; the patients were either known hypertensives or were receiving antihypertensive agents, with no obvious cause for secondary hypertension. The mean systolic and diastolic BP readings of the last 3 clinic visits were calculated. The following information was recorded for the study group; age, sex, duration of diabetes and the degree of control, duration of hypertension as well as the type of antihypertensive agents used. Patients were classified according to the degree of their systolic and diastolic BP control into 4 groups: Systolic BP groups: I: (≤ 120 mm Hg), II: (121-130) mm Hg), III: ( 131-140 mm Hg), IV: >140 mm Hg) and diastolic BP groups: I: (≤80 mm Hg), II: (81-85 mm Hg), III: ( 86-90 mm Hg), and IV: ( >90 mm Hg).
The degree of BP control was determined, and a comparison was made between the groups according to the type of antihypertensive agents used and the degree of blood glucose control. The blood pressure was considered to be controlled if the current reading was found to be less than 130/85 mm Hg.
Data was entered into a computer, and the statistical package for Social Sciences (SPSS version 16) was used for appropriate statistical analysis. The Chi-square test was used to test the association between the categorized variables and a p-value of 0.05 or less was considered as the indication for statistical significance.
RESULTS
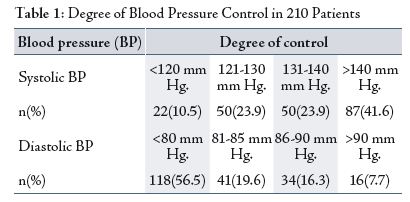
A total of 210 patients were included in the study with a mean age of 53.7±9.1 years with a male to female ratio of 2:5. The mean duration of diabetes was 9 years. A poor control of diabetes was observed among 60.8% of cases (63.6% males and 59.7% females). Only 30% of the diabetic patients were found to have normal blood pressure. The mean duration of hypertension was 7 years. It was observed that a small percentage (34.4%) of patients had their systolic blood pressure controlled, while a high percentage (76.1%) of patients had uncontrolled diastolic BP, and the difference was found to be statistically significant (p<0.001). (Table 1)
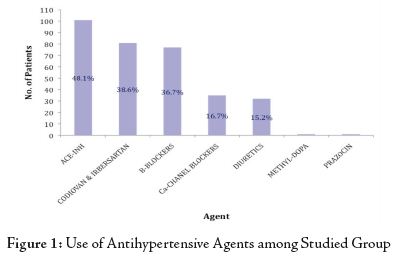
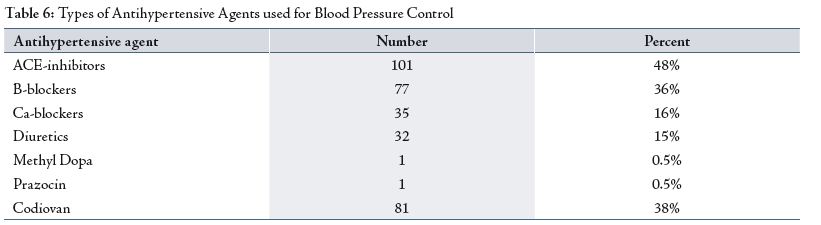
The most frequently used agent was angiotensin converting enzyme inhibitor (ACE) which was used by 48% of patients, followed by angiotensin receptor blockers (ARB) combined with diuretics in 38.57% of the patients, while B-blockers (Atenolol) were used in 36.6% of patients, calcium channel blockers were used by 16.6%, and diuretics (Bendrofluizide) were used in 15.2% of patients. (Fig. 1)
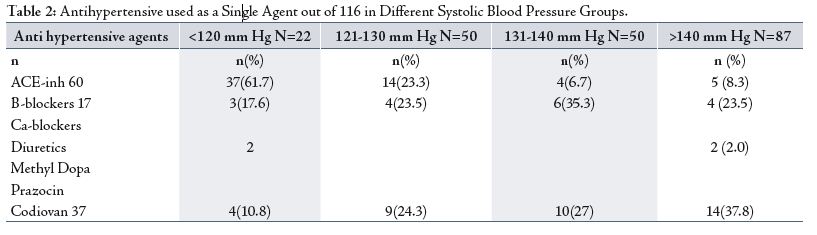
In the study group, more than half of the patients (55.7%) were using antihypertensives as a single agent for the control of BP. A total of 101 (48%) patients were found to take ACE inhibitors (Fig. 1). Among them, 58.4% used these agent as monotherapy and 41.6% used it in combination with other drugs. ACE inhibitors were more effective as monotherapy in the systolic blood pressure group, where 85% of cases exhibited BP below 130 mm Hg (Table 2). However, ACE inhibitors were found to be more effective in diastolic blood pressure when combined with other medications, 73% of cases in the diastolic blood pressure group exhibited BP values below 85 mm Hg. (Table 3)
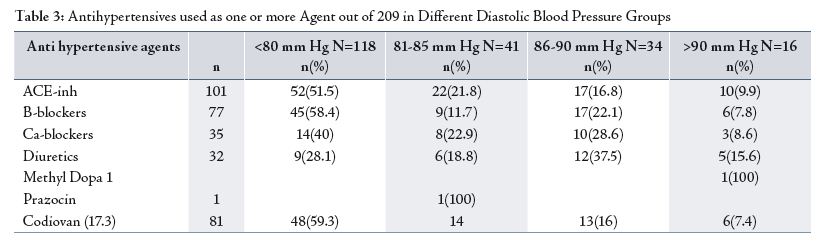
Co-diovan was effective in the diastolic BP whether used as a single agent (in 83% of patients, diastolic BP was below 85 mm Hg) (Table 4), or when combined with other medications, (76.6% of patients’s BP was below 85 mm Hg. (Table 3)
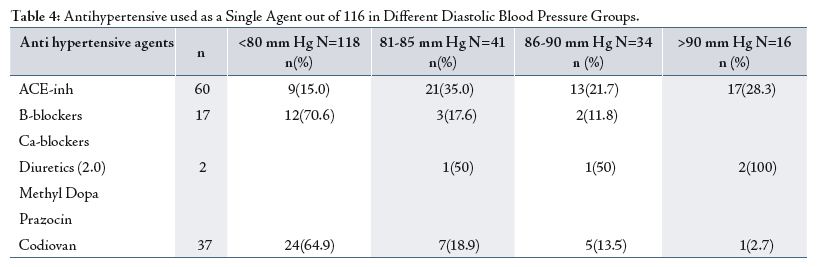
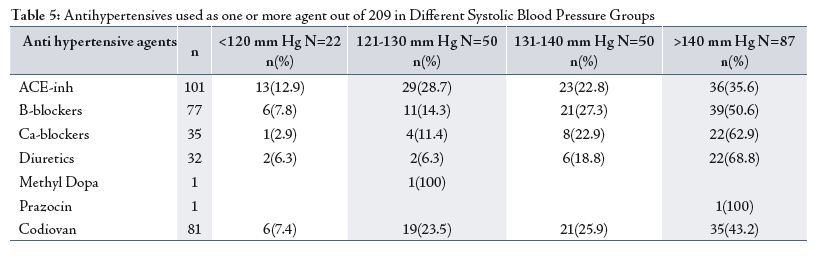
B blockers were more effective as a single agent in the diastolic BP group. 88% of patients exhibited BP values below 85 mm Hg (Table 4), or when combined with other drugs. In 70% of the patients, the diastolic BP was below 85 m Hg, (Table 3). All hypotensive medications were more effective in controlling diastolic BP (Table 5), while they were less effective in controlling systolic BP. ( Table 6)
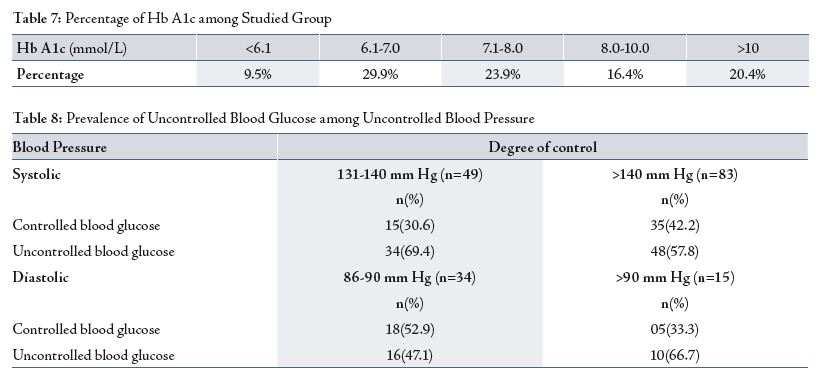
60.8% of patients from the studied group had uncontrolled blood sugar, (Table 7). Patients with uncontrolled systolic BP (group III and IV) were more likely to have poorly controlled blood glucose. (Table 8)
DISCUSSION
Hypertension is twice as common in persons with diabetes as it is in others.6 Hypertension is known to contribute to diabetic micro-and macro-vascular complications.7,8 To reduce the risk, hypertension must be diagnosed accurately and promptly, and the patient must receive adequate treatment. However, new guidelines have been published to stress on the importance of aggressive blood pressure control in diabetics.4 This study attempted to evaluate the blood pressure control in diabetic patients in primary healthcare. A review of 1137 hypertensive diabetics showed that only 21% of the patients met the currently recommended BP for diabetes of <130/85 mm Hg.9 In this current group, the frequency of patients who met this recommendation was only 30%. This indicates that more effort is needed to control BP in diabetics.
In this study, it was observed that the predominant part of blood pressure which was poorly controlled was the systolic blood pressure (>130 mm Hg) which accounted for 65.5% of cases, (Table 1). Results from the Systolic Hypertension in Elderly Program (SHEP), and Systolic Hypertension in Europe (Sys-Eur) trial, favored the aggressive treatment of diabetics with isolated systolic hypertension.10,11 Therefore, more effort is needed to address this aspect of BP.
In this study, Angiotensin lowering enzyme inhibitors (ACE), were found to be the most frequently used antihypertensive agents (used by 48% of the patients), followed by Angiotensin Receptor Blockers (ARB), which were used by 38.57% of the patients, (Fig. 1). Recent trials have suggested that for the prevention of cardiovascular events, ACE inhibitors may be superior to alternative antihypertensive agents.12,13 Results from the Heart Outcome Prevention Evaluation (HOPE) study showed that a reduction of cardiovascular events with ACE inhibitors was much greater than that expected for BP reduction alone compared with placebo.14,15 Angiotensin converting enzyme inhibitors had favorable effects not only on cardiovascular events, but also on renal and quality of life as compared with other regiments.16,17 In this study, almost half of the patients used antihypertensive as a agents as monotherapy. It was observed that ACE-inhibitors were more effective at reducing the systolic blood pressure, but out of the 101 who used ACE-inhibitors, 60 patients used it as a single agent. It seems that it is advisable to combine ACE-inhibitors with other medications in order to have a more potent effect. The JNC 7 favors the combination of drugs for a more potent reduction of BP. However, it does not favor the combination of ACE inhibitors with B blockers, or diuretics with calcium channel blockers. Therefore, for patients with uncontrolled BP, it is advisable to observe the type of drugs used in combination before taking the decision of adding another drug.4 Another factor against the control of BP with combined medication is non compliance.
The Canadian Coalition for Blood Pressure Control, reported a non compliance rate of 50%.18 Non-adherence is the major cause of treatment failure. Patients seen in this clinic may get fed up from taking long term medication for their BP and blood glucose control. It was observed that most patients with uncontrolled hypertension had poorly controlled blood glucose (Table 2). Good blood glucose control was defined as glycosylated hemoglobin <7%, fasting blood glucose <7 mmol/L, or 2 hours post-prandial blood glucose <11 mmol/L.
Inspite of this fact, the message from both ACCORD and ADVANCE trials is that near-normal glycemic control for a median of 3.5 to 5 years does not reduce cardiovascular events within that time frame.19 Physicians’ education with regards to the importance of BP control in diabetics and the better selection of drugs for combination therapy should be considered promptly and efficiently.
CONCLUSION
Only 30% of BP of the hypertensive diabetics met the recommended BP values for diabetes. More effort should be addressed to control the BP in diabetics. Physicians should be careful in selecting hypertensive medications, because some combinations are not useful.
ACKNOWLEDGEMENTS
The authors reported no conflict of interest and no funding has been received on this work.
-
Turner RC, Millns H, Neil HA, Stratton IM, Manley SE, Matthews DR, et al. Risk factors for coronary artery disease in non-insulin dependent diabetes mellitus: United Kingdom Prospective Diabetes. BMJ 1998 Mar; 316(7134):823-828.
-
UK Prospective Diabetes Study group. Tight blood pressure control and risk of macro and micro vascular complications in type 2 diabetes. BMJ 1998 Sep; 317(7160):703-713.
-
The ALLHAT officers and coordinators for the ALLHAT Collaborative Research Group. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs. diuretic. The Antihypertensive and Lipid Lowering Treatment to prevent Heart Attack Trial (ALLHAT). JAMA 2002 Dec; 288(23):2981-2997.
-
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL JR, et al. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: The JNC 7 report. JAMA 2003 May; 289(19):2560-2572.
-
Goral AH, Mully AG Jr. Hypertension. 4th ed. Joint National Committee the seventh. Philadelphia: Lippincott; 2001.
-
Epstein M, Sowers JR. Diabetes Mellitus and hypertension. Hypertension 1992 May; 19(5):403-418.
-
AL-Nozha MM, AL-Maatoug MA, AL-Mazroie YY, AL Harthi SS, Arafah MR, Khalil MZ, et al. Diabetes Mellitus in Saudi Arabia- Saudi Med J 2004 Nov; 25(11):1603-1610.
-
Al Mustafa BA, Abulrahi HA. The role of primary health care center in managing hypertension. How far are they involved? Saudi med J 2003 May; 24(5):460-465.
-
Maue SK, Farrely EW, Frech F. The need for improved blood pressure control within the diabetic hypertensive population. Program and abstracts of the 61st Scientific Session of the American Diabetes Association. 2001 June 22-26. Philadelphia: United States of America. Diabetes 2001 Jun; 50(2):12.
-
Curb JD, Pressel SL, Cutler JA, Savage PJ, Applegate WB, Black H, et al. ‘Effect of diuretic-base antihypertensive treatment on cardiovascular disease risk in older diabetic patients with isolated systolic hypertension: Systolic Hypertension in Elderly Program Cooperation Research Group. JAMA 1996; 76:1886-1892.
-
Tuomile hto J, Rastenyte D, Brikenhager WH, Thijs L, Antikainen R, Bulpitt CJ, et al. Effects of calcium-channel blockade in older patients with diabetes and systolic hypertension. N Eng J Med 1999; 340:677-684.
-
Pahor M, Psaty BM, Furberg CD. Treatment of hypertensive patients with diabetes. Lancet 1998 Mar; 351(9104):689-690.
-
Pahor M, Psaty BM, Furberg CD. New evidence on the prevention of cardiovascular events in hypertensive patients with type 2 diabetes. J cardiovascular pharmacol 1998; 32(2):518-523.
-
The Heart Outcomes Prevention Education Study Investigators. Effects of an angiotensin-converting enzyme inhibitor ramipril on cardiovascular events in high-risk patients. N Eng J Med 2000 Jan; 342(3):145-153.
-
Heart Outcomes Prevention Evaluation Study Investigators. Effects of ramipril on cardiovascular outcomes in people with diabetes mellitus: results of the HOPE study and MICRO-HOPE substudy. Lancet 2000 Jan; 355(9200):253-259.
-
Lewis EJ, Hunsicker LG, Bain RP, Rohde RD. for the Collaborative Study Group: The effect of angiotensin-converting –enzyme inhibitor on diabetic nephropathy. N Eng J Med 1993 Nov; 329(20):1456-1462.
-
Croogh SH, Levine S, Testa MA, B Bulpitt CJ, Jenkins CD, et al. The effect pf antihypertensive therapy on the quality of life. N Engl J Med 1984; 314: 1655-1664.
-
Chockalingam A, Bacher M, Camphell N, Cutler H, Drover A, Feldman R, et al. Adherence to management of high blood pressure: recommendations of the Canadian Coalition for High Blood Pressure Prevention and control. Can J Public Health 1998; 89:15-111.
-
Dluhy RG. Intensive Glycemic Control in the ACCORD and ADVANCE Trials. N Eng J Med 2008 Jun; 358(24):2630-2633.