
Circumferential Pleural Shadow
Jojy George1, Jayakrishnan B1, Rajeev Jain2, Omar A. Al-Rawas1
Submitted: 19 Aug 2008
Reviewed: 09 Sept 2008
Accepted: 22 Sept 2008
From the 1Department of Medicine and 2Radiology, PO Box.35, Postal Code.123,
Al Khod, Muscat, Sultanate of Oman
Address correspondence and reprint request to: Dr. Jojy George, MD, FRCP
Consultant, Department of Medicine, Sultan Qaboos University Hospital, PO Box.35; Postal code.123, Al Khod, Sultanate of Oman
Email: drjojy@hotmail.com
A 40-year-old Omani male, nonsmoker, presented with right-sided chest pain and weight loss of four months duration. He gave a history of pleural effusion five years ago, which was investigated thoroughly including Mantoux and multiple pleural biopsies. Though no definite diagnosis was made at that time, the effusion resolved spontaneously. His current chest radiograph (Figure 1) and a representative picture from the computed tomography (CT) of the chest (Figure 2) are displayed below.
 |
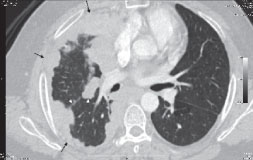 |
| Figure 1: Chest radiograph showing a peripheral opacity with nodular inner margins extending from the apex to the lower zone on the right side with obliteration of the costophrenic angle. Nodular shadows also involve the upper medial aspect of the right lung. | Figure 2: CT showing the circumferential thickening of the pleura involving its entire extent in the costo-parietal, posterior and mediastinal aspects encompassing the lung, and extending into the fissures. |
What is the most likely diagnosis?
1. Pleural plaques
2. Multiloculated pleural effusion
3. Empyema
4. Malignant mesothelioma
5. Metastatic adenocarcinoma
Answer
Malignant mesothelioma
DISCUSSION
Chest radiograph shows circumferential pleural nodules involving the basal, lateral, apical and mediastinal aspects with loss of the right hemidiaphragm shadow and a possible effusion on the right side. CT scan confirms the circumferential thickening of the pleura involving its entire extent in the costo-parietal, posterior and mediastinal aspects encompassing the lung, and extending into the fissures. Ultrasound-guided pleural biopsy confirmed a diagnosis of malignant mesothelioma.
Though chest radiograph suggests the possibility of a multiloculated effusion or an empyema, the CT films confirm the pleural thickening and absence of effusion. Healed pleural involvement in tuberculosis can present as pleural thickening, but is usually patchy with calcifications and seldom encompasses the whole lung as in this case. Metastatic adenocarcinoma also does not usually involve the pleura circumferentially.
Though malignant mesothelioma is uncommon, it is the most common primary pleural neoplasm. Worldwide, the incidence is increasing and it is expected to peak in the year 2020. In 80% of cases, it is associated with exposure to asbestos. The disease is more commonly found unilaterally and that too on the right side. It occurs predominantly in men.
The most common symptoms include dyspnea, non-pleuritic chest pain, cough, and weight loss. CT images show circumferential, nodular pleural thickening >1 cm that may encase the lung. The most common chest radiographic findings are pleural effusion, pleural thickening, discrete pleural masses, large lung nodules, and hilar mass and rib destruction. The diagnosis can be made by a needle biopsy or more accurately by thoracoscopy. Recurrent exudative pleural effusion can occur in mesothelioma.1 Though the tumor is often aggressive, pleural effusions can spontaneously regress and may later present with a totally different radiological appearance in a short time as in our patient.
Surgery has proved most useful for palliation. Combined treatment approach using extra pleural pneumonectomy or pleurectomy/decortication and adjuvant radiotherapy or chemotherapy has shown better prognosis.2 Novel therapies include intrapleural chemotherapy, photodynamic therapy, hyperthermic perfusion and immunomodulating and targeted treatments.3 But the median survival in malignant mesothelioma still remains between six and 18 months.
-
Ferrer JS, Muñoz XG, Orriols RM, Light RW, Morell FB. Evolution of idiopathic pleural effusion: a prospective, long-term follow-up study. Chest. 1996 Jun; 109:1508-1513.
-
Robinson BW, Lake RA. Advances in malignant mesothelioma. N Engl J Med. 2005; 353:1591-1603.
-
Zervos MD, Bizekis C, Pass HI. Malignant mesothelioma 2008.Curr Opin Pulm Med. 2008 Jul;14:303-309.