Angioleiomyomas are infrequent benign tumors originating from smooth muscle cells of arterial or venous walls. They are encountered mostly in the deep layers of the dermis or in the subcutaneous tissues of the lower extremities with a prevalence of only 8.5% in the head and neck We present the case of a male patient with an angioleiomyoma of the nasal cavity, a location described in a few cases in the literature.
Case Report
A 40-year-old man presented with recurrent right sided epistaxis to the Christian Medical College, Vellore, a tertiary care teaching hospital in South India. His medical history revealed two previous episodes of epistaxis; two years prior and five months before this presentation. He subsequently had multiple episodes of nasal bleeding. Each episode began and ended spontaneously and there was about 25ml of blood loss during each episode.
Clinical examination revealed a mass in the right inferior meatus displacing the inferior turbinate upwards. A computed tomography (CT) scan of the paranasal sinuses showed an opacified left maxillary sinus with blocked infundibulum and an enlarged right inferior turbinate filling the nasal cavity. There was also polypoidal mucosal thickening in the right maxillary sinus [Figure 1].
The patient underwent right nasal mass excision and left-limited endoscopic sinus surgery under general anesthesia. Intraoperatively, he was found to have a 3cm×3cm well-defined, spherical, grayish/white mass with broad-based attachment to right inferior meatal lateral wall. An arterial bleeder, which was noted at the base of the mass was cauterized, and the mass was excised in toto.

Figure 1: Computed tomography image of para nasal sinuses showing an enlarged right inferior turbinate filling the right nasal cavity and an opacified left maxillary sinus with blocked infundibulum.
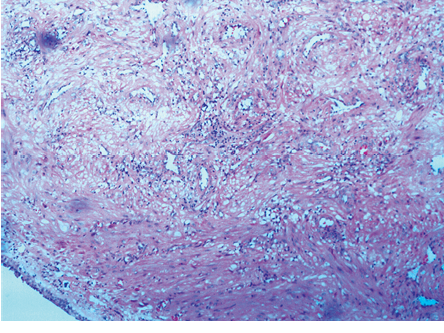
Figure 2: Well-circumscribed tumor lined by respiratory epithelium and composed of numerous vascular channels, magnification= 100×.
Histopathology showed a well-circumscribed tumor, lined by respiratory epithelium, composed of numerous vascular channels. These were surrounded by interlacing bundles of spindle-shaped smooth muscle cells with mildly pleomorphic elongated nuclei having bland chromatin and moderate amounts of cytoplasm [Figures 2 and 3]. Admixed among these smooth muscle bundles were a few clusters of benign adipocytes [Figure 4]. The neoplastic cells were positivie for smooth muscle actin and muscle specific actin. However, desmin and human melanoma black (HMB-45) staining were negative. Hence, a diagnosis of right nasal angioleiomyoma was made. He remained asymptomatic at six months follow-up with no evidence of tumor recurrence.
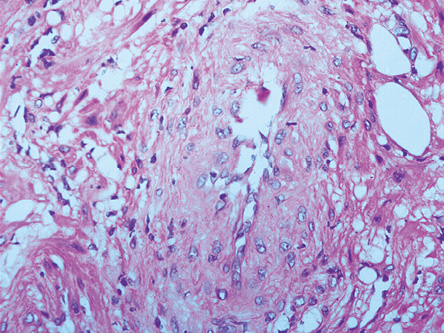
Figure 3: High power magnification (400×) showing a vascular channel the wall composed of bundles of spindle shaped smooth cells with mildly pleomorphic nuclei, finely dispersed chromatin and moderate amounts of cytoplasm.
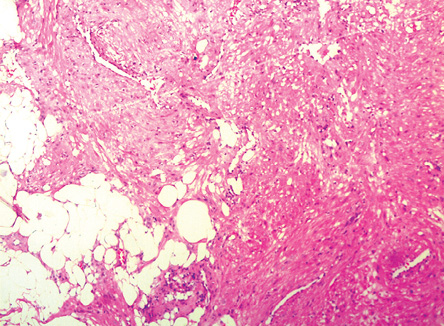
Figure 4: Clusters of mature adipocytes interspersed among the tumour cells, magnification= 200×.
Discussion
Angioleiomyoma, also known as vascular leiomyoma or angiomyoma, was first described by Stout et al,1 in 1937. According to the 2002 World Health Organization (WHO) classification of tumors, angioleiomyoma is defined as “a frequently painful, benign subcutaneous or deep dermal tumor composed of mature smooth muscle bundles which surround and intersect between vascular channels”. However, in the 2013 update, angioleiomyoma, which earlier belonged to the group of ‘smooth muscle tumors’, was reclassified into the ‘pericytic (perivascular)’ tumors group. This is because it shares morphological features with myopericytoma by showing perivascular concentric arrangement of smooth muscle cells.2
Angioleiomyomas are divided into three subtypes based on the dominant histological pattern: solid, venous, and cavernous.3 Solid, the most common subtype, shows a strong female predominance, whereas the venous and cavernous types are slightly more common in males.4
Approximately 89% of angioleiomyomas occur in the extremities. The most common region of occurrence is in lower extremities, which account for almost 67% of these tumors.5 Only 8.5% to 10% of angioleiomyomas arise in the head and neck area. Here, they usually present as venous or cavernous type and exhibit a male preponderance.6 Rarely reported are angioleiomyomas of the nasal cavity. However, they have been described in many other areas including the scrotum and oral cavity.7
The literature reports that angioleiomyomas are more frequent in the fourth, fifth, and sixth decades of life, and that more than 80% of angioleiomyomas are less than 2cm in diameter.3,8 They arise commonly in the deep layers of the dermis or in the subcutaneous tissues. The tumor is generally rounded and forms a nodule that usually elevates the skin.1 Their characteristic, small tumor size may be due to their superficial location and slow-growing nature.6 However, if deeply seated, it could grow large due to the absence of symptoms.
Patients with angioleiomyoma most commonly present with pain and temperature sensitivity. Pain is often paroxysmal and triggered by the slightest touch or exposure of the tumor to environmental stimuli. The presence of pain is related to the histological type of the tumor.3,8 The solid type is usually painful (70%) and the venous or cavernous type is painless (pain rate of 30%). Pain is usually present when the lesion is located on an extremity, whereas angioleiomyomas over the head and neck area are usually painless. Pain on exposure to cold in solid angioleiomyomas is believed to be due to the ischemia caused by contraction of vessels in the tumor. Although the exact etiology of angioleiomyomas is not known, local infection, trauma, arteriovenous malformation, and hormonal influences have been implicated.9
In our patient, the tumor, despite being a small, painless, hidden mass in the nasal cavity was detected early because of the recurrent episodes of epistaxis. Surgical excision with histological study was the only way to determine the diagnosis.
Most vascular leiomyomas can be diagnosed using histology using conventional hematoxylin and eosin (H&E) staining. Histologically, a solid or capillary type of angioleiomyoma consists of smooth muscle bundles, which by their close interlocking structure give the vascular channels a slit-like shape. A cavernous type tumor is composed of a dilated vascular channel with a thin smooth muscular wall whereas a venous angioleiomyoma has a thick smooth muscle.10 Smooth muscle cells of angioleiomyoma are mature and well-differentiated and mitotic figures are usually absent or very rare. Rarely, the tumor may show areas of hyalinization, calcification, or myxoid change.
It is important to distinguish between angioleiomyoma, angiomyolipomas, and leiomyosarcomas. The cutaneous angiomyolipoma is differentiated from angioleiomyoma by the presence of mature adipose tissue within the tumor. Adipose tissue is present in only 2.5% to 3% of angioleiomyomas, whereas it can occupy approximately 20% to 30% of angiomyolipomas. Angiomyolipomas show immunoreactivity with HMB-45. In leiomyosarcoma, which is a malignant smooth muscle tumor, there is nuclear atypia and mitosis and the tumor nuclei are typically cigar-shaped and arranged in interweaving fascicles.4 Other differences include myopericytoma, hemangioma, angiofibroma, and angiofibromyoma. The treatment of choice for angioleiomyoma is surgical excision. After complete excision, the tumor seldom recurs.
Conclusion
Angioleiomyomas are benign tumours, originating from smooth muscle cells of arterial or venous walls, seen mostly in the lower extremities. Their occurrence in the nasal cavity is extremely rare. Endoscopic surgical excision is the treatment of choice and recurrence after complete excision is rare.
Disclosure
The authors declared no conflict of interests.
references
- Stout AP. Solitary cutaneous and subcutaneous leiomyoma. Am J Cancer 1937 Mar;29:435-469.
- Jo VY, Fletcher CD. WHO classification of soft tissue tumours: an update based on the 2013 (4th) edition. Pathology 2014 Feb;46(2):95-104.
- Morimoto N. Angiomyoma (vascular leiomyoma): A clinicopathologic study. Med J Kagoshima Univ 1973;24:663-683.
- Willoughby AD, Schlussel AT, Freeman JH, Lin-Hurtubise K. Angioleiomyoma in a rare location: a case report. Hawaii J Med Public Health 2013 Feb;72(2):45-48.
- Duhig JT, Ayer JP. Vascular leiomyoma: A study of sixty-one cases. Arch Pathol 1959 Oct;68:424-430.
- Wang CP, Chang YL, Sheen TS. Vascular leiomyoma of the head and neck. Laryngoscope 2004 Apr;114(4):661-665.
- Mahima VG, Patil K, Srikanth HS. Recurrent oral angioleiomyoma. Contemp Clin Dent 2011 Apr;2(2):102-105.
- Hachisuga T, Hashimoto H, Enjoji M. Angioleiomyoma. A clinicopathologic reappraisal of 562 cases. Cancer 1984 Jul;54(1):126-130.
- Hung KF, Yan AH, Kao SY, Chang CS. Angioleiomyoma in the right lingual gingiva- a case report. Chin J Oral Maxillofac Surg 2005 Sept;16:179-187.
- Kim HI, Roh SG, Lee NH, Yang KM, Park HS. Angioleiomyoma of the auricle. Arch Plast Surg 2013 Jan;40(1):68-69.