Van der Woude syndrome (VWS) is one of the most common clefting syndromes.1 The classic presentation in patients with VWS are congenital lower lip pits related to cleft lip, cleft palate, or both.2,3 The significance of lip pits is the reported association with the phenotypic expression of cleft lip and or cleft palate of varying degrees of severity.1 Furthermore, studies reported in the literature have described the types of cleft associated with different types of lower lip pits. These reports indicate that the bilateral, unilateral, or mixed-type lip pits are more likely to occur with cleft lip with or without cleft palate.4 The high degree of penetrance and variable expression of VWS emphasizes the need to recognize the condition even in its most subtle form and, once recognized, awareness of the implications. Genetic counseling of affected individuals and their families is also important to assess the likelihood of occurrence of the syndrome in subsequent siblings and future generations.5 We report an interesting case of VWS to highlight its peculiar clinical presentation and management.
Case Report

Figure 1: Repaired bilateral cleft lip and symmetrical paramedian dome-shaped elevations and lower lip pits in a six-year old girl.
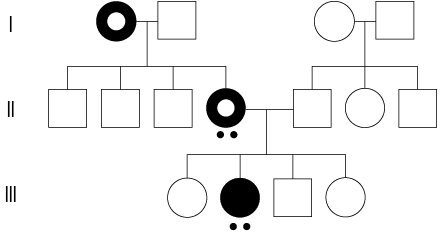
Figure 2: Pedigree of the family: Black and white circle represents grandmother and mother with bilateral cleft of the primary palate. Black circle represents the patient with bilateral cleft of the primary and secondary palate. Double dots represents the presence of lower lip pits.
A six-year-old girl was referred to the plastic surgery clinic at the Ahmadu Bello University Teaching Hospital, Zaria, Nigeria, for repair of a fistula in the hard palate. The parents were concerned about her abnormal speech. She had also recently become introverted after being teased at school. She had a repair of bilateral cleft of the primary and secondary palate performed at four and 22 months of age, respectively. The extraoral examination revealed bilateral dome-shaped swellings with pits, located lateral to the midline on the vermilion border of the lower lip [Figure 1]. There was no saliva or secretions at the base of the pits. The oral examination revealed a narrow fistula in the anterior palate. She had normal dentition and her limbs were normal. The lesions on her lower lip were present since birth. They were asymptomatic and her parents reported no secretions from the lip pits. Her mother had similar symmetrical paramedian elevations on the lower lip, but the father was unaffected. The mother and grandmother were also found to have had repaired bilateral complete cleft of the primary palate. Examination of the other siblings and all close relatives revealed that they were unaffected. The construction of a pedigree led us to a diagnosis of VWS [Figure 2]. The fistula was repaired with mucoperiosteal flaps. However, the father refused any therapeutic intervention of the congenital lower lip pits for both
daughter and mother.
Discussion
VWS (Online Mendelian Inheritance in Man (OMIM) #119300) is a rare craniofacial syndrome.6 The first report in the literature was by Demarquay in 1845,7 and was comprehensively described in detail by Van der Woude in 1954.8 The syndrome is genetically transmitted in an autosomal dominant mode with variable expression, as well as a high and incomplete penetrance (80–100%).3,9,10 Its estimated prevalence varies from 1:40,000 to 1:100,000 live births. Most cases of VWS have been linked to chromosome 1q32-q41 known as VWS locus 1, but a second VWS locus (VWS2 – OMIM #606713) has been mapped to 1p34.1,3 The incidence of lip pits among cleft patients is approximately 2%.10 Other studies show an incidence of 24% to 31% with the classic presentation of a combination of lip pits and cleft lip and/or palate.5,6 Sex distribution is equal and differences in expression are not sex related.11 There is a relatively high incidence in females and this has been attributed to the established fact that women are more likely to consult a physician in cases of cosmetic defects.6
In the development of the lip and palate, fusion of the mandibular arch and lateral sulcus of the lower lip occurs at 5.5 weeks, whereas fusion of the maxillary and nasofrontal processes occurs at six weeks.12 An incomplete reduction of the naturally occurring lateral sulcus, which normally occurs at the same time as fusion of the lip and palate, is thought to be the most plausible cause of lip pits.5,11,13 The whole of the lateral sulcus is usually obliterated with the exception of the cephalic end, which becomes deeper as growth proceeds. At the same time the edges of the furrow become more prominent and ultimately fuse together. This converts the furrow into a tubular canal, which is open at its upper end. The canal is subsequently incorporated into the deeper tissues of the lower lip, as this separates from the mandibular arch and remains as a congenital fistula.14
Congenital lip pits may be divided according to their location into three types: commissural, midline upper lip, and lower lip.13 Lower lip pits have been described under several names, including fistula labii inferioris, labial humps, labial cysts, labial fistulae, and paramedian sinuses of the lower lip.5 Reflecting several degrees of gene expression, lower lip pits may manifest clinically as a wide spectrum. These include slight depressions on the vermilion border of the lip, and fistulas that penetrate into subjacent minor or major salivary glands and drain small amounts of saliva.6 Dome shaped elevations, and/or openings, with no depth presumably represent microforms of lower lip pits. The lip elevations may occasionally fuse in the midline, producing a snout like structure.14 There may be a solitary pit in the center of the lip, two pits, or a single pit on either side of the lip. They may occur on the surface of the wet vermillion or dry vermillion, or on the margin between the wet and dry vermillion.15 Lip pits are usually circular or oval in shape, but have also been described in the literature as transverse, slit-like, or sulci.14 They may be shallow or deep, varying from an asymptomatic slight depression on the vermilion border of the lower lip to deep fistulas that penetrate into the accessory salivary glands. These may drain small amounts of saliva, either visible or expressible, in the lip pits.9,13,15 Most of these lesions are asymptomatic and this is similar to what we found in our patient and her mother.
It is important to emphasize that although the occurrence of lip pits may suggest VWS, not all children with lip pits have the syndrome. Pits on the commissures not associated with VWS occur in about 2% of neonates and may be associated with periauricular sinuses. Furthermore, pits of the midline and upper lip are uncommon and often sporadic. The differential diagnosis of VWS includes other congenital anomalies associated with lip pits such as popliteal pterygium syndrome and occasionally type-1 orofaciodigital syndrome and alveolar synechia syndrome.15,16
Cosmetic considerations are the most common indication for surgical intervention. However, persistent mucous secretions and painful recurrent inflammation may also justify a surgical procedure.9,13,17,18 Lip pits with mild symptoms may require no treatment. In our case, the father refused surgical intervention for mother and child and this was acceptable to them both. It is also acknowledged in the literature that many patients neither require nor request surgery.15,17
The goals of treatment are two-fold; removal of sinuses and cosmetic relieve for the disfigurement. The recommended surgical technique requires the complete excision of sinus tracts, correction of abnormal elevations and protrusion, and the maintenance of the orbicularis muscle ring for optimal lip function. It is also critical to ensure the prevention of secondary deformities such as whistling defects.18 Several detailed reviews have described simple excision of the sinuses using horizontal or vertical methods.2,15,17,18 However, due to unsatisfactory surgical outcomes, alternative techniques have been proposed, such as vertical wedge resections, the split lip advancement technique (SLAT), or resection with AlloDerm graft implantation. More recently, the inverted-T lip reduction technique was introduced as an alternative method to treat lower lip pits.2,18
Physical examination of relatives, interviews of older relatives, and a close examination of family photos are considered essential to identify affected family members.15 The identification of familial lip pits is crucial for genetic counseling. Genetic counseling is advised because the probability of a having offspring with cleft lip, with or without cleft palate, is reported to be 10-times greater in a cleft patient who also has lip pits than in those without lip pits. All parents with VWS should be cautioned that there is a 50% risk of having a child with a cleft lip and/or cleft palate due to its autosomal dominant mode of transmission.13,16
Conclusion
VWS is a rare condition with noteworthy clinical presentation. It can be associated with cleft lip with or without cleft palate. Surgical intervention for cosmetic purposes may be considered when lip pits are the only manifestation of the VWS. It is also acknowledged that patients may not request or seek reconstructive surgery. Surgical excision is especially indicated in patients with production of mucous secretions and/or recurrent inflammation. Genetic counseling is crucial for affected parents and patients with information regarding the pattern of inheritance and the consequence of these phenotypes emphasized.
Disclosure
The authors declared no conflicts of interest.
Acknowledgments
The authors would like to acknowledge Dr A.O Ibrahim for her valuable comments on the manuscript.
references
- Lam AK, David DJ, Townsend GC, Anderson PJ. Van der Woude syndrome: dentofacial features and implications for clinical practice. Aust Dent J 2010 Mar;55(1):51-58.
- Chen CH, Liao HT, Shyu VB, Chen PK. Inverted-T lip reduction for lower lip repair in Van der Woude syndrome: a review and comparison of aesthetic results. Int J Oral Maxillofac Surg 2013 Feb;42(2):198-203.
- Souto LR. Congenital bilateral lower lip pits associated with fistulae of the minor salivary glands: case report of the principal Van der Woude syndrome’s trait. Aesthetic Plast Surg 2008 Jan;32(1):172-174.
- Ferrero GB, Baldassarre G, Panza E, Valenzise M, Pippucci T, Mussa A, et al. A heritable cause of cleft lip and palate–Van der Woude syndrome caused by a novel IRF6 mutation. Review of the literature and of the differential diagnosis. Eur J Pediatr 2010 Feb;169(2):223-228.
- King NM, Cheong CH, Sanares AM. Van der Woude syndrome: a report of two cases. J Clin Pediatr Dent 2004;28(3):267-271.
- Dissemond J, Haberer D, Franckson T, Hillen U. The Van der Woude syndrome: a case report and review of the literature. J Eur Acad Dermatol Venereol 2004 Sep;18(5):611-613.
- Demarquay JN. Quelques considerations sur le bec-delievre. Gaz Med Paris 1845;13:52-53.
- Van Der Woude A. Fistula labii inferioris congenita and its association with cleft lip and palate. Am J Hum Genet 1954 Jun;6(2):244-256.
- Bardazzi F, Savoia F, Dika E, Rinaldi R. Van der Woude syndrome: a case report. Int J Dermatol 2006 Mar;45(3):299-301.
- Huang JJ, Hou JW, Tan YC, Chen KT, Lo LJ, Chen YR. Van der Woude syndrome: clinical presentation in 64 patients. Cleft Palate Craniofac J 2007 Nov;44(6):649-652.
- Schinzel A, Kläusler M. The Van der Woude syndrome (dominantly inherited lip pits and clefts). J Med Genet 1986 Aug;23(4):291-294.
- Ziai MN, Benson AG, Djalilian HR. Congenital lip pits and van der Woude syndrome. J Craniofac Surg 2005 Sep;16(5):930-932.
- Nagore E, Sánchez-Motilla JM, Febrer MI, Serrano G, Bonillo J, Aliaga A. Congenital lower lip pits (Van der Woude syndrome): presentation of 10 cases. Pediatr Dermatol 1998 Nov-Dec;15(6):443-445.
- Rizos M, Spyropoulos MN. Van der Woude syndrome: a review. Cardinal signs, epidemiology, associated features, differential diagnosis, expressivity, genetic counselling and treatment. Eur J Orthod 2004 Feb;26(1):17-24.
- Souissi A, El Euch D, Mokni M, Badri T, Ben Osman Dhahri A. Congenital lower lip pits: a case report. Dermatol Online J 2004;10(2):10.
- Guner U, Celik N, Ozek C, Cagdas A. Van der Woude syndrome. Scand J Plast Reconstr Surg Hand Surg 2002;36(2):103-105.
- Brookes JT, Canady JW. Surgical correction of congenital lower lip sinuses in Van der Woude syndrome. Cleft Palate Craniofac J 2007 Sep;44(5):555-557.
- Tokat C, Bilkay U, Songur E, Akin Y. Van der Woude syndrome in twins. J Craniofac Surg 2005 Sep;16(5):936-939.