
Laparoscopic Removal of Large and Sharp Foreign Bodies from the Stomach
ABSTRACT
Ingestion of foreign bodies is a common occurrence. Majority would pass spontaneously without any complications. Occasionally large and sharp foreign bodies may get stuck and give rise to complications. Removal of large sharp foreign bodies is recommended due to their potential of danger. Foreign bodies can be removed by endoscopy or by laparotomy. We present the two cases of laparoscopic removal of large sharp foreign bodies from the stomach. Laparoscopic removal of large sharp foreign bodies from the stomach is safe.
Submitted:11 September 2007
Reviewed: 7 October 2007
Accepted: 19 November 2007
Address Correspondence and reprint request to: Golash V., MBBS, MS, FRCS. Sr. Consultant Surgeon, SQH, Salalah
Email: golash@omantel.net.om or haritagolash@hotmail.com
INTRODUCTION
Majority of the foreign bodies of different shapes and sizes are reported to pass spontaneously without much harm to the patients during the observation period. When foreign bodies do not pass spontaneously endoscopic or surgical removal is necessary. Surgery is indicated in failed endoscopic removal. Conventionally foreign bodies are removed by laparotomy; we present our experience with laparoscopic removal.
CASE 1
A 35 year old man admitted with the history of a right upper abdominal pain for last few days. On examination he was found to have a tender mass in right upper quadrant. An abdominal plain x-ray showed a long radio-opaque object in the upper abdomen lying obliquely, most probably in the stomach. (Figure 1a) Ultrasound and the CT scan of the abdomen confirmed a metallic object, perforating the pyloric end of the stomach and embedded in the right lobe of the liver. The colon, gall bladder, rest of the viscera were not affected and no there was no free fluid or gas in the abdomen. With these findings endoscopic removal was avoided. He was resuscitated and prepared for surgery.

Figure 1a: Plain x-ray showing a long radio-opaque object in the upper abdomen
Surgical Procedure: A thorough Laparoscopy was performed through of umbilical port. There was no free fluid, no pus. There was a mass in the right upper quadrant adherent to anterior abdominal wall sealed all around by the greater omentum. The stomach and the right lobe of liver were adherent to the mass. The hepatic flexure of colon was not seen. The greater omentum was separated gently from the mass which exposed the right lobe of liver. The lower half of the stomach was adherent to liver and was separated next. It
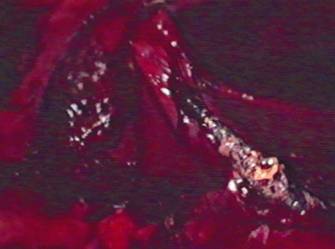
Figure 1b: Foreign body penetrating the liver
revealed a sharp metallic foreign body, perforating through the pyloric end of the stomach and penetrating the right lobe of liver close to the gall bladder (Figure 1b). The hepatic flexure of colon was not involved. The foreign body was impacted in the stomach. A 10 cm long anterior gastrostomy was performed with the help of ultracision to deliver the foreign body. The sharp upper end of the foreign body was close to the esophagus-gastric junction. The foreign body (which was an old rusted screwdriver without a handle) was gently lifted off the stomach at its top free end and was taken out from the stomach (Figure 1c). Both ends of the foreign body were sharp and with great care one end was manipulated and fed into the left lower mid-clavicular port till the end was visible outside the abdomen (Figure 1d). The foreign body along with trocar sheath was removed under vision (Figure 1e). The foreign body was 15.5 cm long (Figure 1f). The gastrostomy wound was closed in two layers and the perforating wound at the pyloric end was closed with the omental patch in the same manner as the closure of perforated peptic ulcer. His post operative recovery was uneventful and was discharged home on 5th. postoperative day. He was seen 4 months after surgery and was asymptomatic.


Figure 1c: Gastrostomy and removal of foreign body Figure 1e: Foreign body along with port removed
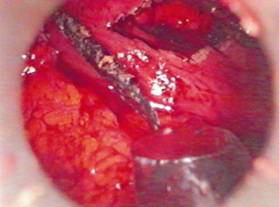

Figure 1d: Foreign body fed in trocar Figure 1f: Foreign body measuring 15.5 cm
Case 2
An eighteen year old, morbidly obese (BMI 65) lady was admitted with the history of having swallowed three A4 size batteries three days prior to admission. While she was as an in-patients she further swallowed a broken long handle of the table spoon. She was asymptomatic. On examination per abdomen there was no sign or symptoms of peritonitis. A plain x-ray abdomen showed the foreign bodies in her stomach (Figure 2a). An endoscopic removal was attempted (Figure 2b). Only three A4 size batteries were seen but broken long

Figure 2a: Plain X-ray of abdomen
end of the table spoon which was seen earlier in the plain x-ray of abdomen was not seen in the stomach. On entering the duodenum the tip of the long handle of the broken spoon was visible in the third part of the duodenum (Figure 2b). It was pulled back in the stomach with the help of the snare but was too dangerous to remove it by endoscopy for the fear of perforation of the esophagus. It was also not possible to snare or hold the A4 batteries. The endoscopy was abandoned and patient was prepared for surgical removal of these foreign bodies. Patient was consented for the laparoscopy/laparotomy removal of several foreign bodies in the stomach. Laparoscopic approach was similar to hiatus hernia repair. Through anterior gastrostomy foreign bodies were removed in the retrieval bag one by one (Figure 2c). Post operative recovery was uneventful. She was doing well two months after the surgery.
DISCUSSION
Removal of foreign bodies from the stomach is controversial. Management of ingested foreign bodies varies according to the type, size, location and patient age. Majority of foreign bodies would pass spontaneously (90%) only 10-20% would require endoscopic and less than 1% surgical removal. 1 Foreign bodies posing danger because of their shape and size should be removed. Various options available include endoscopic, surgical, laparoscopic, and laparo-endoscopic removal of foreign body from stomach. 2, 3, 4 Endoscopic removal is the procedure of choice and is successful in most of patients. Endoscopic removal is more successful in children and in cases of short duration of impaction. 5 Surgery is required for failed endoscopic
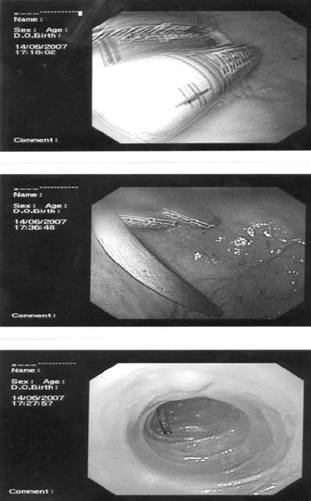
Figure 2b: Foreign bodies in stomach and duodenum
removal and for complications like perforation and obstruction. 6, 7, 8, 9, 10 Removal of Long sharp objects longer than 3 cm is recommended even in asymptomatic patients. 11 The complication rate is increased in case of sharp and impacted foreign body. Perforation is rare and is usually in areas of physiological sphincters, acute angulations and areas of previous surgery. Delayed presentation and silent perforations of stomach caused by foreign bodies has also been reported. In our patient first case, exact duration of swallowed foreign body was not known but it looked very old and rusted .Obstruction, abscess formation, hemorrhage, fistula and mucosal ulcerations are the some other complications reported. In the second case although she was asymptomatic, she had swallowed a sharp broken handle of the table spoon, and the A4 batteries which could have busted or eroded through the stomach.

Figure 2c: Foreign body retrieved
Conventionally foreign bodies are removed from stomach by laparotomy. Laparoscopic removal is an attractive alternative. It is less invasive, less painful and offers faster recovery. It should be the procedure of choice in failed endoscopic removal. Laparoscopic removal of long and sharp foreign bodies from the stomach is feasible.
REFERENCES
1.
Schenk C, Mugomba G, Dabidian RA, Scheuerecker H, Glaser F, Laparoscopic extraction
of a swallowed fork in a patient first diagnosed with bulimia nervosa. Surg Endosc. 2002; 16(2):361.
2.
Caratozzolo E, Massani M, Antoniutti M, Basso S, Monica F, Jelmoni A, Bassi N. Combined
endoscopic and laparoscopic removal of ingested large foreign bodies. Case report
and decision algorithm. Surg Edosc 2001; 15:1226.
3.
Furihata M, Tagaya N, Furihata T, Kubota K. Laparoscopic removal of an intragastric
foreign body with endoscopic assistance. Surg Laparosc Endosc Percutan Tech. 2004;
14:234-237.
4.
Mazza D, Bereder I, Carret V, Bereder JM Laparoscopic removal of intragastric foreign
bodies. Surg Laparosc Endosc Percutan Tech. 2000; 10:329-331.
5.
Park JH, Park CH, Park JH, Lee SJ, Lee WS, Joo YE et al. Review of 209 cases of
foreign bodies in the upper gastrointestinal tract and clinical factors for successful
endoscopic removal. Korean J Gastroenterol.
2004; 43:226-233 (ISSN: 1598-9992).
6.
Stricker T, Kellenberger CJ, Neuhaus TJ, Schwoebel M, Braegger CP. Ingested pins
causing perforation. Arch Dis Child. 2001; 84:165-166.
7.
Rygl M, Pycha K. Perforation of the stomach by a foreign body in a girl with anorexia
nervosa--case report] Rozhl Chir. 2002; 81:628-630.
8.
Lam PY, Marks MK, Fink AM, Oliver MR, Woodward A. Delayed presentation of an ingested
foreign body causing gastric perforation. J Paediatr Child Health. 2001; 37:303-304.
9.
Braumann C, Goette O, Menenakos C, Ordemann J, Jacobi CA Laparoscopic removal of
ingested pin penetrating the gastric wall in an immunosuppressed patient. Surg Endosc.
2004; 18:870.
10.
Omejc M. Laparoscopic removal of an ingested pin migrating into the liver. Surg
Endosc. 2002; 16:537.
11.
Wishner JD, Rogers AM. Laparoscopic removal of a swallowed toothbrush. Surg Endosc.
1997; 11:472-473.