| |
Abstract
Objectives: The prevalence of smoking among adolescents varies in different parts of the world. The current study aims to survey the socio-demographic and family characteristics related to adolescent lifetime cigarette smoking among 1201 Iranian adolescents aged 15-18 years old.
Methods: This study is a population-based cross-sectional survey conducted using the multistage random cluster sampling method in Tehran, Iran in the summer of 2010.
Results: The prevalence of lifetime cigarette use amongst boys (30.2%) was about 1.5 times that of girls (22.2%), (p=0.002). Older age, low parental control, very little parental supervision in the adolescent’s selection of friends, and having a friend or family member who smokes were associated with lifetime cigarette use among male adolescents. Moreover, the use of verbal punishment by the parents was a protective factor for female lifetime cigarette use. Smoking has become one of the great health threats among Iranian adolescents.
Conclusions: As a result, health promotion programs should be gender based whilst educational and interventional programs for preventing tobacco use should begin before adolescence.
Keywords: Adolescent; Smoking; Cigarette; Family behavior; Tehran; Iran.
Introduction
Smoking is one of the most common causes of death worldwide. It has been estimated that the number of deaths related to tobacco use will reach 10 million by 2030.1 Previous studies show that the average age of the first cigarette consumption is 15.4 years old and the average age of starting daily consumption of cigarettes is 18 years old.2 Recent studies suggest that people are starting to smoke at an earlier age and also indicate increased prevalence of smoking in children and adolescents. If this pattern continues, smoking will be responsible for 250 million deaths of children and adolescents now and in the future which will mostly affect developing countries.3 In addition, the adolescents starting to smoke at an early age will tend to be more addicted to cigarettes and less willing to quit. The socioeconomic status of the adolescents is an important factor in starting to smoking.4,5 In developing countries, lack of educational programs, especially for girls, leads to little information about the dangers of tobacco.4
If the adolescents experience at least one cigarette before the age of 18, the risk of addiction to cigarettes will increase in adulthood.6,7 Several studies have shown that if smoking is not stopped, addiction to cigarettes and substance abuse will increase in adulthood.8,9 Adolescents can become addicted to nicotine just like adults.10
The prevalence of smoking among adolescents is different in various parts of the world. The current prevalence of cigarette use among adolescents aged 13-15 years is reported to range from just under 1% to 39.6% in 43 countries.11,12 According to reports of the Global Youth Tobacco use Survey (GYTS), gender was not a determinant in the smoking rate among the youth in half of these countries. However, in some countries, tobacco use is increasing among girls.4,13 The differences of the smoking prevalence between the two genders depend on social norms, customs, culture, socioeconomic status and demographic factors.4
Based on previous reports, prevalence of self-reported smoking in 2000 was 26% and 1.4% among Iranian men and women, respectively.14 In a population-based study among Iranians aged 15-64 years old, the prevalence of current and daily consumption of cigarettes were 14.8% and 13.7%, respectively.15 There have been a few studies focused on the prevalence of tobacco use in Iranian adolescents. For example, the prevalence of smoking based on the serum levels of cotinine among 14- to 18-year-old Iranian men and women was 14.6% and 10.6%, respectively.16 Another study showed that the prevalence of self-reported smoking among Iranian students aged 11-18 years old is 14.3%, with a higher prevalence in boys.17 A recent study on male students aged 10-19 years found that the prevalence of lifetime smoking, current cigarette consumption, and frequent consumption of cigarettes was 27.5%, 8.6%, and 2.7%, respectively.18
The metropolis of Tehran, with an approximately 1500 square kilometer space area and a population of 8 million people, is the capital of Iran. Most of the Tehran population live in the cities and have a socioeconomic level of middle to high. In addition, more than 50% of the Tehran population is below the age of 25.19-21 There is very little information about tobacco use among adolescents in the developing world. Regarding Iran, these data are even more less available for adolescents in a population-based study.18,22,23 Therefore, the objective of this population-based study was to determine the prevalence of cigarette smoking among adolescents and look into personal and family factors influencing this.
Methods
This population-based cross-sectional study was conducted among 1201 adolescents in Tehran, Iran in 2010 using the Persian Youth Risk Behavior System Surveillance (PYRBSS) questionnaire which was adapted according to Iranian culture employing multistage sampling. The YRBSS is a state and national standardized questionnaire consisting of 87 items. The PYRBS is a self-administered questionnaire adapted from the 2009 YRBS. The YRBSS focuses on health-risk behaviors established during youth. These behaviors included unintentional and intentional injuries, tobacco use, alcohol and drug abuse, sexual behaviors that result in HIV infection, other sexually transmitted diseases (STDs), unintended pregnancies, unhealthy dietary behaviors, physical inactivity, being overweight and asthma.24 Ethical approval was obtained from the Ethics Committee of the Tehran University of Medical Sciences (code number: 89-01-28-10494). In addition, the respondents were ensured about confidentiality of responses and their privacy.
A brief demographic survey questionnaire was developed by the research team. The second questionnaire was the Persian Youth Risk Behavior System Surveillance (PYRBSS). The mean correlation coefficient and Cronbach's α in the domain of tobacco use were 0.73 and 0.77, respectively.24 Finally, the tobacco use domain data was used.
It should be mentioned that this study is a part of a large survey, which aimed to investigate the high risk behavior among 1201 adolescents aged 15-18 years old who live in Tehran. The sample is derived through multi-stage cluster sampling of the 22 municipal districts of Tehran. Then, based on the adolescent population of Tehran and the sex ratio within each district, the numbers of girl and boy participants were calculated.
Data collection was conducted with the participation of 33 trained data collectors. Data collection was conducted based on home visit and self-administrated method. Finally, 1201 questionnaires were analyzed using SPSS version 16 and STATA version 10. Descriptive and analytical indicators were determined. The chi-square test was employed for the bivariate analysis. The level of significance was set at 0.05. The results of the univariate analysis were reported with crude odds ratios with 95% confidence intervals, test statistics, and corresponding p-values. Multivariate logistic regression was employed to determine the associated factors for experiencing cigarette smoking. Backward LR stepwise logistic regression was used for the variable under interest which was binary in nature. The results of the multivariate analysis were presented with adjusted odds ratios with 95% confidence intervals and p-values. Lifetime cigarette use was considered as the dependent variable while age, school type, wealth index, parental educational level, parental control, parental punishment, history of consulting with expert individuals, gender bias towards the females from the parents, the pattern of decision-making in the family, educational success, interest in education, family income adequacy, having smoker friends or family members were considered as the independent variables. It should be noted that the variables with p<0.2 in the univariate analysis were entered into the logistic regression model.
The PYRBSS completed by the adolescents collected the data on the socio-demographic variables, lifetime cigarette use, smoked a cigarette before the age of 13, ever smoked cigarettes daily, current cigarette use, frequent cigarette use, and tried to quit smoking cigarettes in the 12 months before the survey. Lifetime cigarette use was defined as having had ever tried cigarette smoking (even one or two puffs). Current cigarette use was defined as the percentage of adolescents having had ever smoked at least one day in the 30 days leading up to the survey. Frequent cigarette use was defined as having had smoked cigarettes on 20 or more days during the 30 days leading up to the survey.
Social class was categorized into four groups, based on the occupation of the man of the family: the higher class, including major landowners, merchants and manufacturers; the middle class, including government administrators, teachers, minor landowners, army officers, clergymen, individuals with personal professions and professionals; the working class, including professional and skilled workers; and the lower class, including the unemployed and the unskilled workers.25
In this study, using principle factor analysis, 12 economic variables (vacuum, separate kitchen, computer, washing machine, bath, freezer, dishwasher, private car, mobile phone, colored TV, any type of video device and home telephone) were combined with each other. The resulted variable (wealth index) was divided into five percentiles from 0 to 20 (the poorest), 21 to 40 (poor), 41 to 60 (intermediate), 61 to 80 (rich), and 81 to 100 (very rich).
Results
The socio-demographic characteristics of the participants are shown in Table 1. Among the 1201 adolescents aged 15-18 years participating in the study, 609 were girls and 592 were boys. Their mean age was 16.74 (SD=1.09).
Table 1: Socio-demographic characteristic and crude odds ratio, by gender and lifetime cigarette use in the survey respondents.1
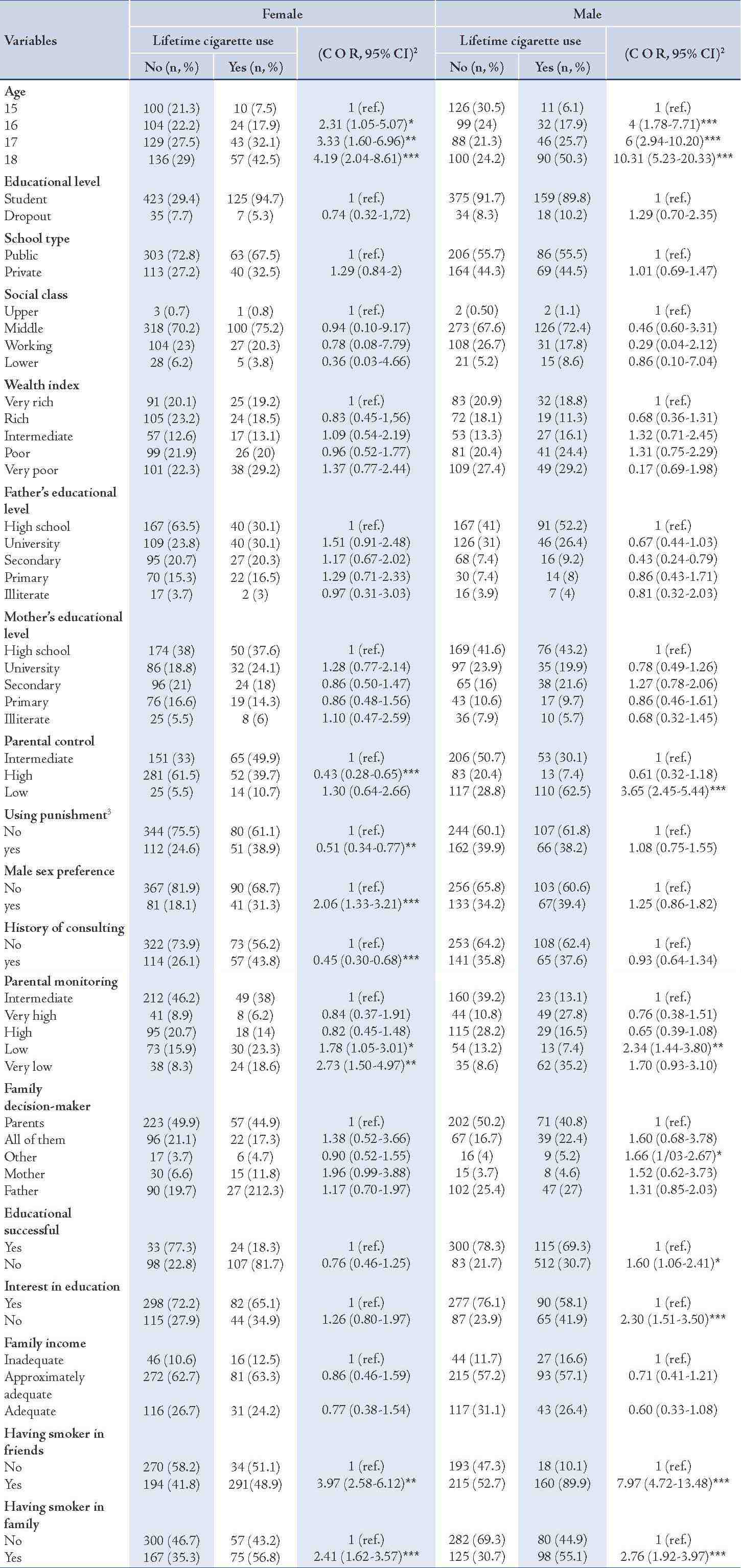
Table 2: Smoking patterns among survey respondents,1 by gender.
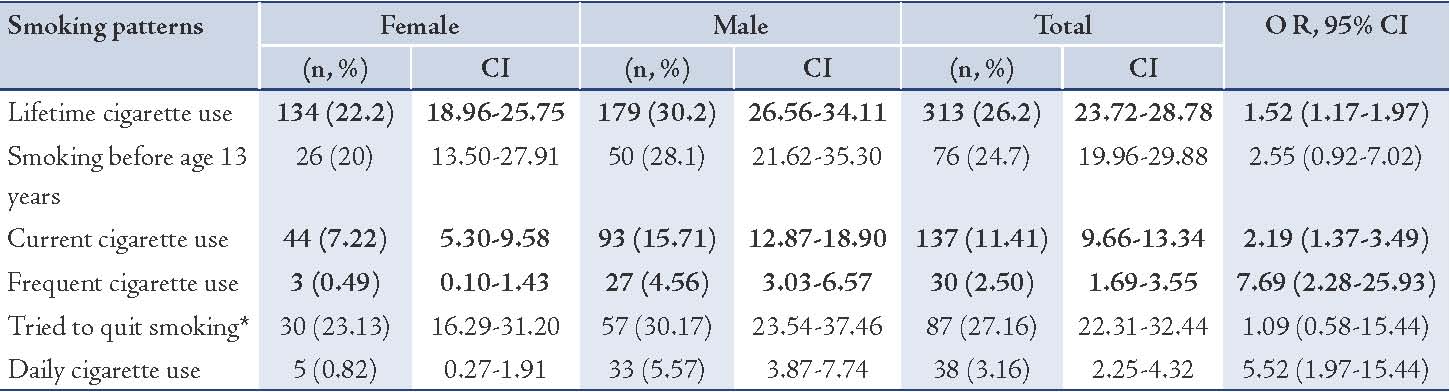
Prevalence cigarette smoking behaviors is reported in Table 2. The Table 2 shows that 26.2% of the adolescents had the experience of smoking. Prevalence of smoking experience in the boys was 1.52 times that of the girls (OR: 1.52; 95% CI: 1.17- 1.97) whereas 24.7% of the smoking adolescents experienced smoking the first time at or before the age of 13. Among the 26.6% of the adolescents who had the experience of smoking, 29.7% reported consumption of at least one cigarette per day for the 30 days before the survey. The odds ratio of daily smoking was 5.52 for boys against the girls (OR: 5.52; 95% CI: 1.97- 15.44). The table also shows that 44.2% were current cigarette consumers (smoking at least one day during the past 30 days before the survey). The odds ratio of current smoking was 2.19 for boys against the girls (OR: 2.19; 95% CI: 1.37-3.49). Prevalence of current cigarette consumption in the whole adolescent participants of the study was 11.41% and 9.7% of them were frequent smokers (smoking 20 days or more during the last 30 days). The prevalence of frequent cigarette use in the whole adolescents participating in the study was 2.5% while 27.16% of the adolescents had tried to quit smoking during the past 12 months. The percentage of boys who tried to quit smoking was reported to be higher compared to the girls which was not statistically significant.
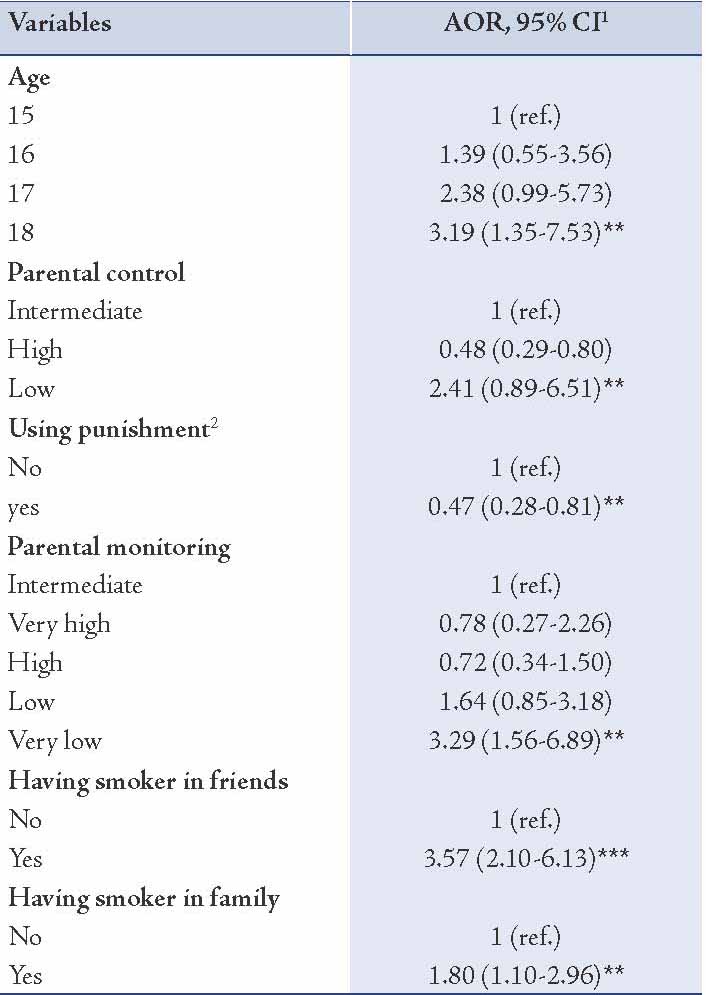
Table 3: Results of multivariate logistic regression analysis of lifetime cigarette use in female adolescent.
Influencing factors on lifetime cigarette use in female and male adolescents are shown in Tables 3 and 4. The result of bivariate analysis in the girls indicated statistically significant differences for the lifetime cigarette use when the subjects were categorized according to older age, high parental control, the use of punishment by the parents (verbal and physical punishment, and prevention from games and entertainments), history of consultation with an expert, very low level of supervision of the parents in the adolescent’s selection of friends, male sex preference by the parents, and having a smoker friend or family member (Table 1).
The results of bivariate analysis in the boys indicated statistically significant differences for the lifetime cigarette use when categorizing the cases into different groups according to older age, low parental control, decision making in the family by people other than the parents and the children, educational failure, lack of interest in education, and having a smoker friend or family member (Table 1).
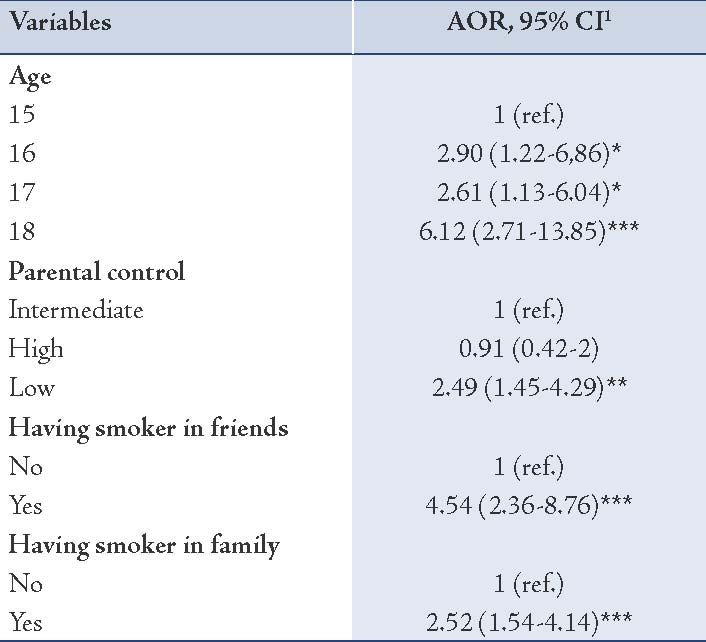
The results of multivariate logistic regression analysis indicated statistically significant associations between lifetime cigarette use and older age, low parental control, very little parental supervision in the adolescent’s selection of friends, and having a smoker friend or family member. Moreover, the use of punishment by the parents was a protective factor for female lifetime cigarette use. (Tables 3 and 4)
Table 4: Results of multivariate logistic regression analysis of lifetime cigarette use in male adolescent.
Discussion
The prevalence of lifetime cigarette use amongst Tehran adolescents aged 15-18 years old was 26.2%. Previous studies have reported the prevalence of smoking in the Iranian adolescents to be 14.3% based on self-reports,17 and 12.5% based on the level of serum cotinine.16 A recent study among students aged 10-19 years old from Tehran schools reported a slightly higher prevalence of tobacco use in the adolescents.18 The higher prevalence of smoking in this study and the study by Ramezankhani et al (2010) could be a warning for the increasing attitude toward tobacco use by the adolescents, especially girls. However, the prevalence of smoking among the adolescents was slightly higher in Ramezankhani's study, but the difference may be due to the method of data collection. In addition, the results of the study suggest a higher prevalence of current and frequent cigarette use among the Iranian adolescents, especially boys. A report published by Warren which based on the GYTS findings of 100 areas of the world, evaluated the prevalence of current cigarette use in the Iranian adolescents to be 2% in the year 2003 and 3% in the year 2007.26 A recent study reported the current and frequent cigarette use by the Iranian boys as 8.6% and 2.7%, respectively.18 In this study, these rates increased to 15.7% and 4.6%.
Consistent with other studies, the results suggest an increased prevalence of current cigarette consumption with the increase of age.27 In the present study, boys to girls smoking ratio was 2.2:1. In a previous study in Iran, this ratio was reported to be 4:1.1.18 Therefore, this study indicates the increasing trend of girls' positive attitude toward smoking consistent with other studies indicating the role of gender in tobacco use by adolescents.28 In most countries, the male gender is the greatest predictor for tobacco use. The global prevalence of tobacco use in boys is four times that of girls (48% vs. 12%).29,30 Comparable with other studies in the world, the results of this study showed that 24.7% of the adolescents reported that their first experience in cigarette smoking began when they were or under the age of 13. According to the findings of GYTS, approximately 24% of all the smokers and 25% of the smoking adolescents aged 13-15 years began smoking from a very young age of 10, without a correct understanding of the dangers of tobacco use and addiction.11,31 In agreement with previous studies, the largest percentage of the current smoker adolescents obtained their cigarettes from stores and supermarkets.11,18,32 The study results, consistent with other studies, suggest the high prevalence of attempts to quit smoking among the current cigarette smoking adolescents.11,18,33,34 The findings showed that almost a quarter of the current adolescent cigarette consumers reported an attempt to quit smoking during the past year. Thus, considering the above results, available consultation services and community-based educational programs for smoking cessations are essential.
This study, consistent with others, confirmed the influence of friends and family on tobacco use by adolescents.11,17,31,35-38 The findings, in accordance with the study of Wen and colleagues (2009), showed that there is a significant relationship between parental control over the adolescents and cigarette smoking38; suggesting up to 2.5 times higher probability of adolescent cigarette smoking. Moreover, inadequate parental monitoring on the adolescent’s selection of friends and also the preference of the male sex by the parents increased the probability of smoking amongst girls up to about 3.5 and 2 folds, respectively. However, the use of punishment by the parents reduced the possibility of experiencing smoking among the girls. It should be noted that the most common reported punishment was the use of verbal punishment by the parents. The results also showed that peer pressure and the presence of a smoker in the family was an effective factor in tobacco use. In this study, having a smoker friend or family member increased tobacco use in the adolescents. Adolescents have easy access to tobacco products which leads to experiencing smoking. Although selling tobacco products to people less than 18 years of age is illegal, they are still widely available due to lack of close monitoring and the acceptance of tobacco use as a social behavior.
Consistent with previous studies, having a smoker family member affected adolescent tobacco use.17,39 Generally, 39.1% of the adolescents reported having at least one smoker in the family. As shown in Table 2, having a smoker friend or family member significantly increases the probability of experiencing smoking by the adolescent. The highest probability was seen in adolescents who had a smoker friend; this effect was greater in boys (OR: 4.54; 95% CI: 2.36-8.76) than girls (OR: 3.58; 95% CI: 2.10-6.13).
Conclusion
The study results show that many young Iranians are involved in smoking; 26.2% of Iranian adolescent had experienced smoking, and 11.4% were currently smoking. Although current as well as frequent cigarette use is less likely to cause addiction than long term cigarette smoking, it is associated with serious health problems.
Several cultural constraints were encountered during the different stages of the research. Due to cultural barriers self-reported questionnaires were used. However, self-reporting increases the chance of underreporting. To counter this problem and prevent systematic errors in the study, anonymous questionnaires were used. Due to parental obsession, there were some difficulties in reaching the adolescents, especially the girls; by ensuring the parents of confidentiality of the information, their consent was obtained. In this study, the questionnaires were completed by home visits which might have resulted in underreporting. The reason this method was chosen was to obtain the information of all the adolescents including those who had left school.
One of the strengths of the study was using the standard questionnaire which allowed comparison with other studies around the world. Furthermore, important factors affecting adolescent smoking including demographic information, wealth index, educational status and family relations were taken into consideration.
Smoking has become one of the great health threats among the youths in Iran. The results of this study indicate gender differences among smokers and the key role of the family and peer pressure in becoming a smoker. As a result, health promotion programs should be gender based whilst educational and interventional programs for preventing tobacco use should begin before adolescence. In addition, families and friends should be involved in educational and interventional programs, to allow the participation of all the stakeholders in promoting the health of adolescents and help them become productive and responsible adults in the future.
Acknowledgements
This study was funded and supported by Tehran University of Medical Sciences (TUMS); Grant no.10494. We would like to thank all the adolescents and their parents for their participation.
References
1. Aslam N, Bushra R. Active smoking in adolescents of karachi, pakistan. Oman Med J 2010 Apr;25(2):142.
2. CDC. How Tobacco Smoke Causes Disease: The Biology and Behavioral Basis for Smoking-Attributable Disease: A Report of the Surgeon General. Atlanta: GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health 2010.
3. WHO. World Health Organization, International Agency for Research on Cancer. Working Group on the Evaluation of Carcinogenic Risks to Humans, IARC Monographs on the Evaluation of Carcinogenic Risks to Humans: Tobacco Smoke and Involuntary Smoking: International Agency for Research on Cancer; 2004.
4. Gender WH. women, and the tobacco epidemic Geneva: WHO Library Cataloguing; 2010. Available from: http://apps.who.int/bookorders/anglais/detart1.jsp?sesslan=1&codlan=1&codcol=15&codcch=788.
5. Rezaei F, Majdzadeh R, Nedjat S, Golestan B. Motives for cigarette smoking in 13-to 15-year-old boys: A qualitative study. Journal of School of Public Health and Institute of Public Health Research 2007;5(4).
6. Elders MJ, Perry CL, Eriksen MP, Giovino GA. The report of the Surgeon General: preventing tobacco use among young people. Am J Public Health 1994 Apr;84(4):543-547.
7. Chassin L, Presson CC, Rose JS, Sherman SJ. The natural history of cigarette smoking from adolescence to adulthood: demographic predictors of continuity and change. Health Psychol 1996 Nov;15(6):478-484.
8. Helstrom A. A Smoking Intervention for High-risk Adolescents: University of Colorado; 2003.
9. Johnston L. Smoking, Drinking, and Illicit Drug Use among American Secondary School Students, College Students, and Young Adults, 1975-1991. Volume II: College Students and Young Adults: US Government Printing Office, Superintendent of Documents, Mail Stop: SSOP, Washington, DC 20402-9328.; 1992.
10. Kassel J. Are adolescent smokers addicted to nicotine? The suitability of the nicotine dependence construct as applied to adolescents. J Child Adolesc Subst Abuse 2000;9(4):27-49 .
11. Warren C; The Global Youth Tobacco Survey Collaborative Group. Tobacco use among youth: a cross country comparison. Tob Control 2002;11:52-70.
12. Primack BA, Land SR, Fine MJ. Adolescent smoking and volume of exposure to various forms of media. Public Health 2008 Apr;122(4):379-389.
13. Mackay J, Eriksen M, Shafey O. The Tobacco Atlas. Atlanta, GA. American Cancer Society2006.
14. Sarraf-Zadegan N, Boshtam M, Rafiel M. Risk factors for coronary artery disease in Isfahan, Iran. Eur J Public Health 1999;9(1):20 .
15. Meysamie A, Ghaletaki R, Haghazali M, Asgari F, Rashidi A, Khalilzadeh O, et al. Pattern of tobacco use among the Iranian adult population: results of the national Survey of Risk Factors of Non-Communicable Diseases (SuRFNCD-2007). Tob Control 2010 Apr;19(2):125-128.
16. Sarraf-Zadegan N, Boshtam M, Shahrokhi S, Naderi GA, Asgary S, Shahparian M, et al. Tobacco use among Iranian men, women and adolescents. Eur J Public Health 2004 Mar;14(1):76-78.
17. Kelishadi R, Ardalan G, Gheiratmand R, Majdzadeh R, Delavari A, Heshmat R, et al; CASPIAN Study Group. Smoking behavior and its influencing factors in a national-representative sample of Iranian adolescents: CASPIAN study. Prev Med 2006 Jun;42(6):423-426.
18. Ramezankhani A, Sarbandi Z, Zarghi A, Heydari G, Masjedi M. Pattern of Cigarette Smoking in Adolescent Students in Tehran. Pejouhandeh 2010;15(3 (75)):115-122.
19. Mosavi-Jarrahi A, Moini M, Mohagheghi MA, Alebouyeh M, Yazdizadeh B, Shahabian A, et al. Clustering of childhood cancer in the inner city of Tehran metropolitan area: a GIS-based analysis. Int J Hyg Environ Health 2007 Mar;210(2):113-119.
20. Sheikhazadi A, Mehrzad K, Fakhredin T. Violence in forensic medicine practice: a survey of legal medicine practitioners’ views. Am J Forensic Med Pathol 2009 Sep;30(3):238-241.
21. Taghaddosinejad F, Sheikhazadi A, Yaghmaei A, Vakili V, Saberi SM, Behnoush B. A survey of self-mutilation from forensic medicine viewpoint. Am J Forensic Med Pathol 2009 Dec;30(4):313-317.
22. Momenan A, Sarbandi Z, Etemadi A, Azizi F. Pattern Of Waterpipe (Ghalyan) Use Among Intermediate And High School Students: A Cross-Sectional Study In Tehran, Iran. Payesh 2007;6(2):135-144.
23. Tavafian SS, Aghamolaei T, Zare S. Water pipe smoking and health-related quality of life: a population-based study. Arch Iran Med 2009 May;12(3):232-237.
24. Baheiraei A, Hamzehgardeshi Z, Mohammadi MR, Nedjat S, Mohammadi E. Psychometric Properties of the Persian Version of the Youth Risk Behavior Survey Questionnaire. Iran Red Crescent Med J2012;14(6):1-8.
25. Curtis GE, Hooglund EJ, eds. Iran: a country study2008: Library of Congress.
26. Warren C, Lea V, Lee J, Jones N, Asma S, McKenna M. Change in tobacco use among 13—15 year olds between 1999 and 2008: findings from the Global Youth Tobacco Survey. Global health promotion2009;16(2 suppl):38.
27. Eaton DK, Kann L, Kinchen S, Shanklin S, Ross J, Hawkins J, et al; Centers for Disease Control and Prevention (CDC). Youth risk behavior surveillance - United States, 2009. MMWR Surveill Summ 2010 Jun;59(5):1-142.
28. Anderson Johnson C, Palmer PH, Chou CP, Pang Z, Zhou D, Dong L, et al. Tobacco use among youth and adults in Mainland China: the China Seven Cities Study. Public Health 2006 Dec;120(12):1156-1169.
29. Corrao MA, Guindon GE, Cokkinides V, Sharma N. Building the evidence base for global tobacco control. Bull World Health Organ 2000;78(7):884-890.
30. Mackay J, Amos A. Women and tobacco. Respirology 2003 Jun;8(2):123-130.
31. Warren CW, Riley L, Asma S, Eriksen MP, Green L, Blanton C, et al. Tobacco use by youth: a surveillance report from the Global Youth Tobacco Survey project. Bull World Health Organ 2000;78(7):868-876.
32. Kyrlesi A, Soteriades ES, Warren CW, Kremastinou J, Papastergiou P, Jones NR, et al. Tobacco use among students aged 13-15 years in Greece: the GYTS project. BMC Public Health 2007;7(1):3.
33. Rozi S, Butt ZA, Akhtar S. Correlates of cigarette smoking among male college students in Karachi, Pakistan. BMC Public Health 2007;7(1):312.
34. Ergüder T, Soydal T, U urlu M, اak r B, Warren CW. Tobacco use among youth and related characteristics, Turkey. Sozial- und Präventivmedizin/Social and Preventive Medicine2006;51(2):91-8.
35. Hill KG, Hawkins JD, Catalano RF, Abbott RD, Guo J. Family influences on the risk of daily smoking initiation. J Adolesc Health 2005 Sep;37(3):202-210.
36. Kobus K. Peers and adolescent smoking. Addiction 2003 May;98(s1)(Suppl 1):37-55.
37. Engels RC, Vitaro F, Blokland ED, de Kemp R, Scholte RH. Influence and selection processes in friendships and adolescent smoking behaviour: the role of parental smoking. J Adolesc 2004 Oct;27(5):531-544.
38. Wen M, Van Duker H, Olson LM. Social contexts of regular smoking in adolescence: towards a multidimensional ecological model. J Adolesc 2009 Jun;32(3):671-692.
39. Griesbach D, Amos A, Currie C. Adolescent smoking and family structure in Europe. Soc Sci Med 2003 Jan;56(1):41-52.
|
|