|
Abstract
Objective: The aim of this study was to estimate the incidence of diabetic ketoacidosis and the mortality rate at Benghazi city.
Methods: A cross-sectional study of the records of all patients admitted with diabetic ketoacidosis to all Benghazi hospitals (governmental and private) between 1st of January and 31st of December 2007.
Results: The annual incidence of diabetic ketoacidosis was 41.7 episodes/100,000 populations with a mean age of 33±20.1 years (2-93). Around 52% of all the episodes occurred in males and 2.6% of adult Diabetic ketoacidosis occurred in pregnant females. Type-2 diabetics were responsible for 27.7% of all episodes. The commonest precipitating factor in the whole study group was dose disruption (35%), followed by infection (20%). The most common presenting symptoms were gastrointestinal, whilst 3.5% of the patients were comatose at presentation. The overall mortality was 11.7% and there was no significant difference in mortality between males and females (11% vs. 12.6%; p=0.6); however, type-2 diabetics showed a significantly higher mortality rate (29.3% vs. 4.9%; p=0.000).
Conclusion: Diabetic ketoacidosis is a common condition in Libya with a high mortality rate and type-2 diabetics constitute a considerable number of the cases.
Keywords: Diabetes; Ketoacidosis; Incidence; Mortality; Epidemiology.
Introduction
Diabetic ketoacidosis (DKA) is a frequent cause of morbidity and mortality in type-1 diabetics; however, occasionally it also occurs in type-2 diabetics during severe stress.1-6 DKA is the presenting feature of about 30% of Libyan children with type-1 DM,7 and it contributes to a significant number of adult hospital admissions in Benghazi as it constitutes almost 9% of all the diabetes-related admissions,8 and 3.2% of all acute admissions to the medical intensive care unit (ICU).9 However, the annual incidence of DKA in Libyan diabetics is unknown. The overall mortality rate from DKA in Libya ranges from 2 to 10% of all DKA admissions according to different reports.1-3,10
Benghazi is the second largest city in Libya with 670,797 inhabitants according to the 2006 census. The prevalence of diabetes mellitus (DM) in Benghazi is 14.1%,11 with type-1 DM constituting about 6% of all cases. The average annual incidence of type-1 diabetes among 0-14 year olds in Benghazi is 7.8 per 100,000.12 There are two governmental general hospitals for adults and one children hospital in Benghazi; these hospitals beside another four small private hospitals treat all patients with acute medical conditions.
The aim of this study is to study the incidence, clinical features and mortality rate of diabetic ketoacidosis in Benghazi city.
Methods
A cross sectional study of the records of all patients admitted with DKA to all Benghazi hospitals was carried out between 1st of January and 31st of December 2007. Patients were classified as adults or children according to the Libyan health ministry classification, where patients older than 15 years are treated as adults. According to the 2006 survey, 67.6% of the Libyan population is older than 15 years. The following parameters were analyzed: age, gender, nationality, duration of diabetes, duration of symptoms before seeking medical advice, precipitating factors, clinical features, laboratory findings at presentation including; plasma glucose, serum Urea, Creatinine, sodium(Na+), and potassium(K+), urine acetone, arterial blood pH, and bicarbonate (Hco3), duration of hospitalization and the outcome. Patients were classified as having type 1 or type 2 DM based on the diagnosis written in the patients` records. The criteria used to diagnose DKA in the included patients were: Hyperglycemia ≥250 mg/dl, pH<7.3, and/or serum bicarbonate ≤18 mmol/l and the presence of ketonuria (2+ or more).13 The severity of DKA was defined according to the American diabetes association (ADA) criteria,13,14 as follows; Mild: pH 7.25-7.30, moderate: pH 7.24-7, and severe: pH<7.
The incidence rate was calculated as the number of new cases between 1st of January and 31st of December 2007 divided by the city population in the same year and multiplied by 100,000. Data were expressed as mean ± standard deviation (SD). The data were statistically analyzed using the Statistical Package for the Social Sciences (Windows version 11.0; SPSS Inc, Chicago [IL], US). Differences between groups were tested statistically using the Chi squared test and independent-samples t-test. Differences were considered statistically significant when the p-value was less than 0.05.
Results
During the study period, 280 DKA cases (Table 1) were admitted to the medical wards and intensive care units of different hospitals in Benghazi, giving a yearly incidence of 41.7 episode/100 000 populations/year (50.5 episode/100,000 for adult and 23.4 episode/100,000 for children) or 29.6 episode/10,000 diabetic/year. Fourteen patients were responsible for 46 episodes (16.4% of all episodes), 8 patients had 2 episodes, 3 patients had 3 episodes, 2 patient had 6 episodes, and one patient had 9 episodes.
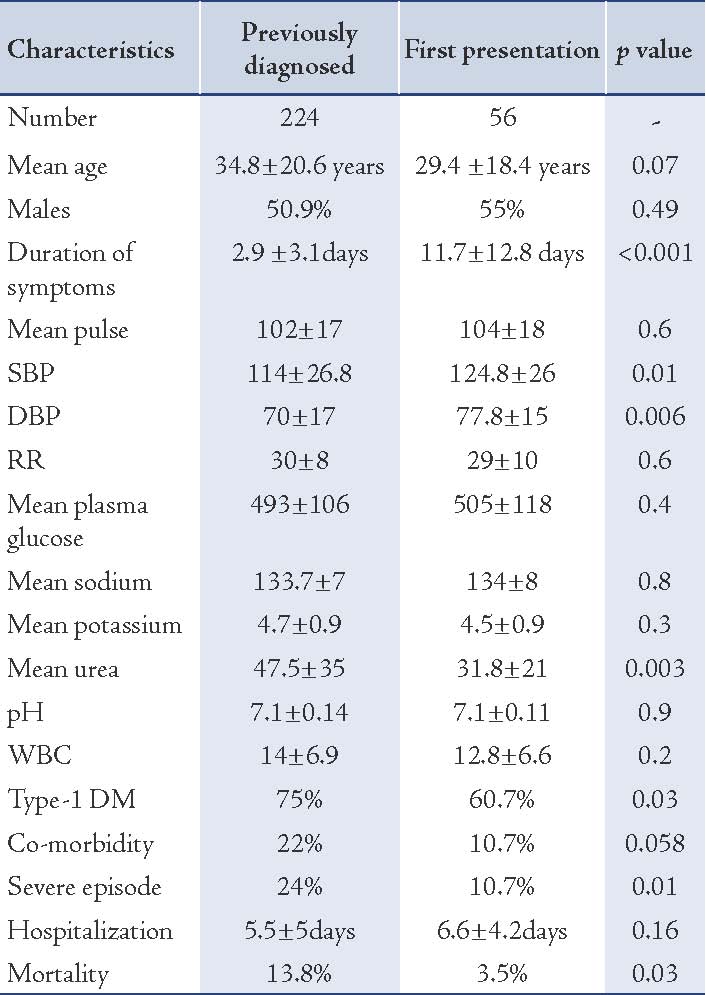
The frequency of episodes progressively increased starting from the age of 2 years to the age of 35 years, then it sharply declined after the age of 40 years. About 65.5% of the episodes occurred in patients younger than 41 years old (Fig. 1). The mean age of all cases was 33±20.1 years (2-93). Adult cases were mostly constituted of Libyans (94.3%), while pediatric cases were exclusively Libyan patients. Around 52% of all the episodes occurred in males and 2.6% of adult DKA episodes occurred in pregnant females. Females had a significantly shorter duration of symptoms before seeking medical help; they also had lower blood pressure, faster pulse rates, lower plasma glucose and arterial pH at admission in comparison to males (Table 2). Type-1 diabetics with DKA had a significantly shorter duration of symptoms, faster pulse rate, lower plasma glucose and serum urea at presentation, while type-2 diabetics had a significantly higher co-morbidity and mortality rates (Table 3). The most common precipitating factor in the whole study group was dose disruption (35%), followed by infection and DKA as the 1st presentation of DM (20% each), the upper respiratory tract infection was the most commonly encountered infection (Table 4). The mean duration of symptoms before presentation was 3.2±3 days with 38.7% of the patients presenting within 24 hrs of onset of symptoms and 73.5% within 3 days. Patients with first presentation had a significantly longer duration of symptoms before being diagnosed (11.7 vs. 2.9; p=0.000), (Table 5). The most common symptoms were polyuria, polydipsia, weakness and fatigue (100% each), followed by vomiting (54.6%), abdominal pain without vomiting (7.5%), headache and dizziness (4.5%), hematemesis (1.8%) and convulsion (1.7%); whilst 3.5% of the patients were comatose at presentation and they were all adult patients.
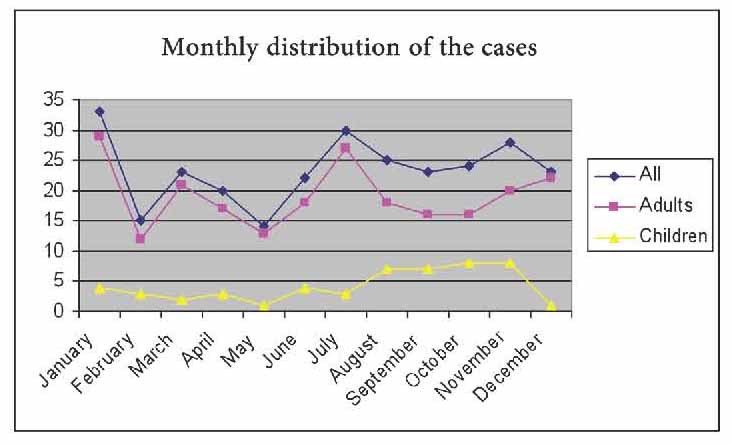
Figure 1: Monthly distribution of the cases
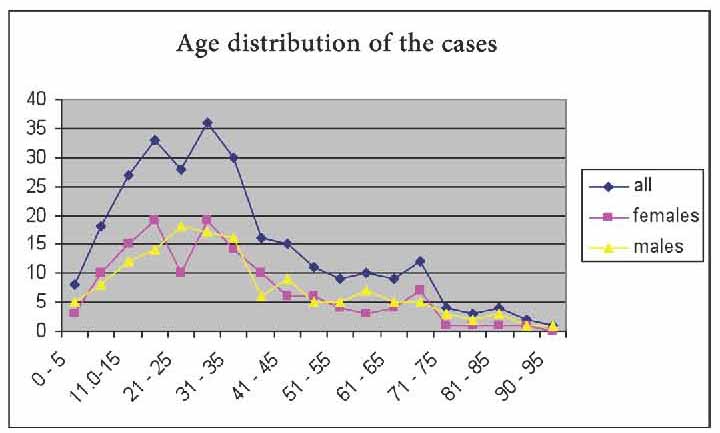
Figure 2: Age distribution of the cases.
Vomiting and headache were significantly more frequent among children than among adults (72.5% vs. 50.6%; p=0.004) and (11.7% vs. 3%; p=0.008) respectively. About 54.2% of all the episodes were managed in the general medical ward. However, 75.5% of severe cases were managed at ICU as compared to 37.9% and 40.7% of mild and moderate cases, respectively (p=0.000). The mean duration of hospitalization were 5.41±4.2 days resulting in a total of 1515 admission days during the year. About 35.5% of the patients were discharged within 3 days of admission and 20% of the patients stayed for longer than 7 days. Patients with severe episodes were admitted for slightly longer periods than non-severe cases (6.8±5.5 vs. 5.6±5.4; p=0.17). Also patients who were managed at ICU stayed significantly longer than patients who were managed in wards (6.7±7 vs. 4.8±2.7; p=0.004).
The overall mortality was 11.7%, which was exclusively in adults (Table 1). Type-2 diabetics showed a significantly higher mortality rate (29.3% vs. 4.9%; p=0.000). Also, known diabetics had a significantly higher mortality than new cases (13.8% vs. 3.5%; p=0.03). Severe cases had a 23.8% mortality rate while moderate cases had a 14.3% mortality rate and mild cases had 13%. The patients who died were significantly older (59±18.8 vs. 29.7±17.8; p=0.000) with longer duration of diabetes (9.5±8.8 vs. 5.4±4.6; p=0.004) and higher rate of co-morbidities (66.6% vs. 13%; p=0.000) and they had significantly faster respiratory rates (38±6.5 vs. 29±9; p=0.000), lower systolic and diastolic blood pressure (102±49 vs. 118±22; p=0.004) and (60.5±31 vs. 73±13; p=0.000), respectively, higher urea (69.7±48 vs. 40±29; p=0.000) and lower platelet count (241±129 vs. 304±108; p=0.009) at presentation. While there was no significant difference (p>0.05) between the patients who died survived in terms of symptom duration (3.3±2.4 vs. 4.9±4), mean pulse rate (104±24 vs. 103±17), mean plasma glucose (529±101 vs. 492±109), mean serum sodium (133±7.4 vs. 134±7.4), mean serum potassium (4.7±0.9 vs. 4.6±0.9), mean leukocyte count (15.5±7.6 vs. 13.5±7) and mean blood pH (7±0.15, 7.1±0.13) at presentation.
Table 1: Comparison between DKA episodes in children and adults.
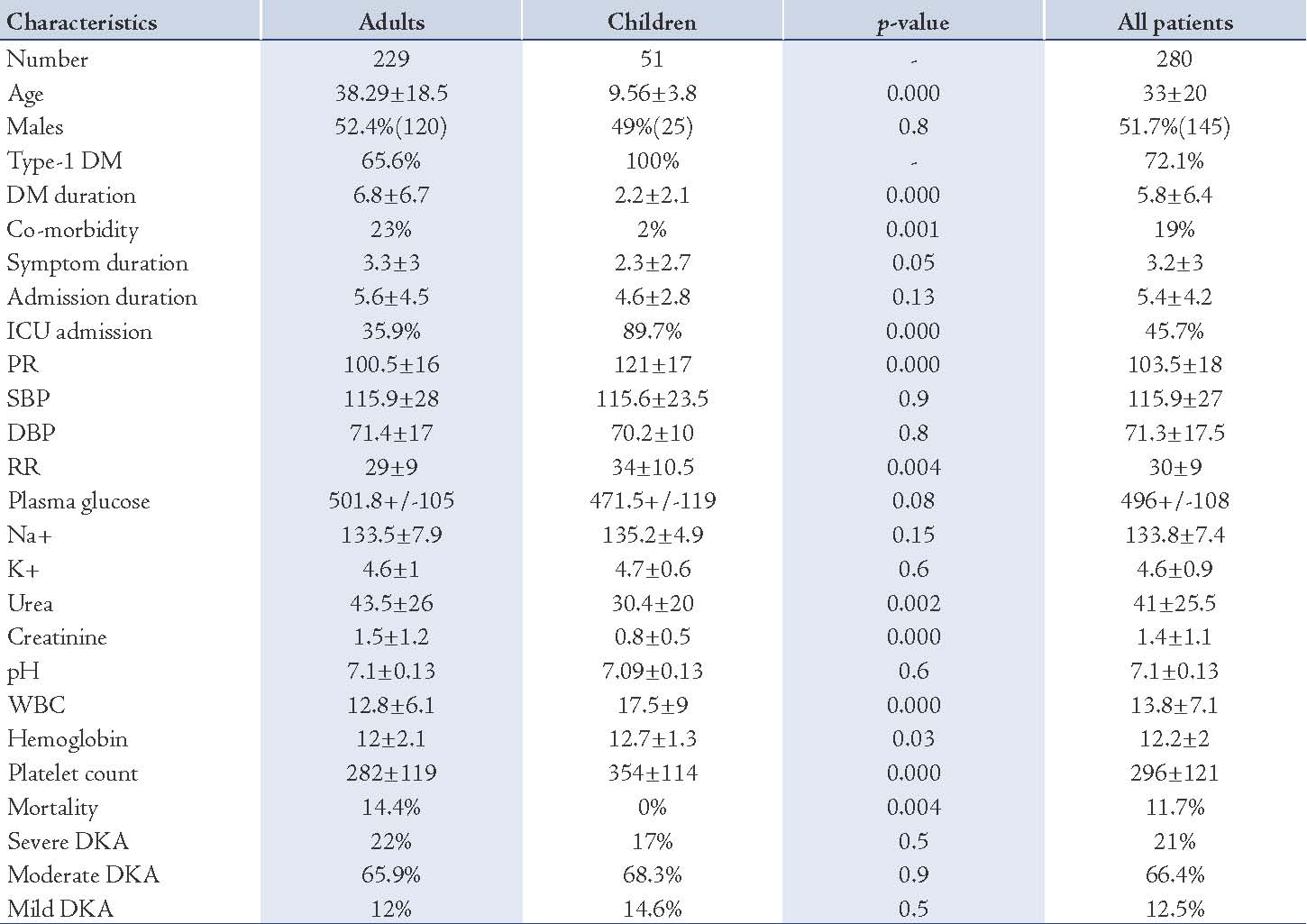
Table 2: Comparison between DKA episodes in males and females.
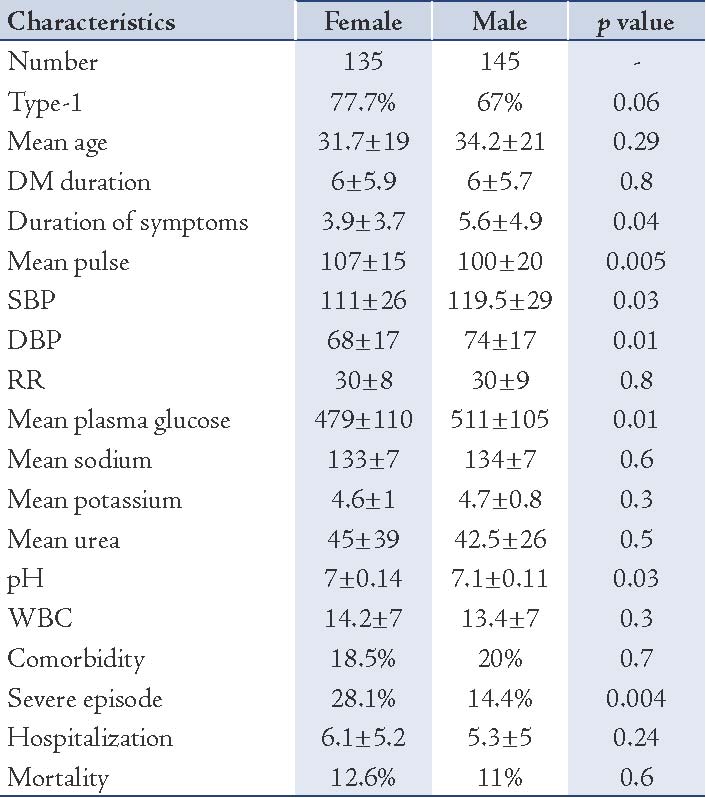
Table 3: Comparison between DKA episodes in type-1 and type-2 diabetics.
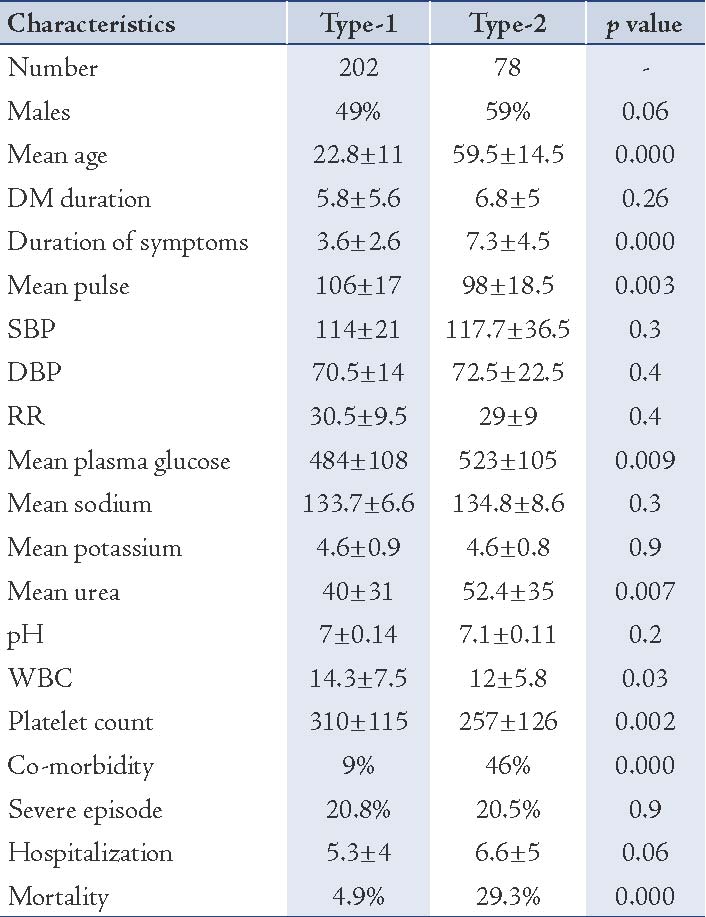
Table 4: Precipitating factors.
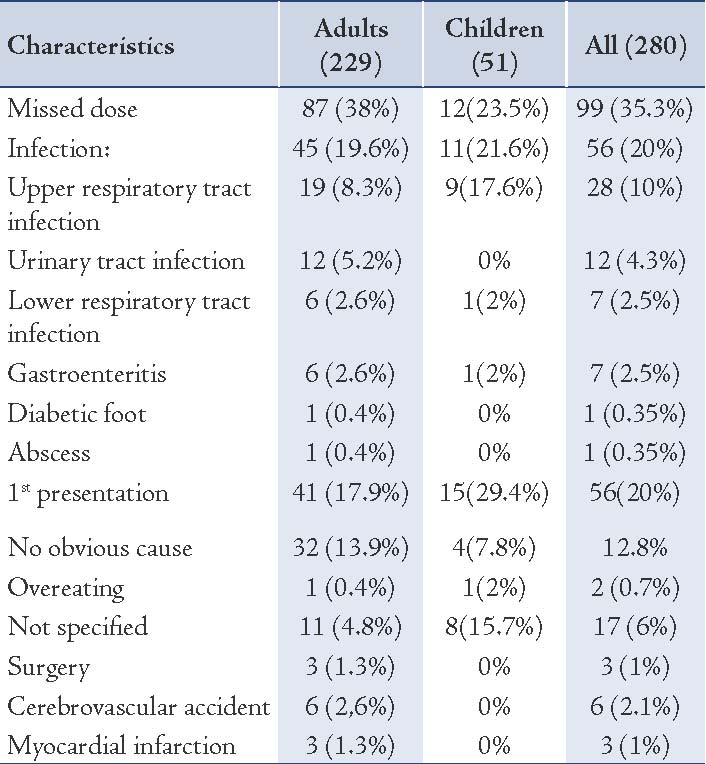
Table 5: Comparison between DKA episodes among previously diagnosed and newly diagnosed diabetics.
Discussion
The incidence rate of 41.7 episodes /100,000 populations /year is three times higher than the 12.9 reported from Denmark.15 This does not necessarily means a higher rate of diabetes in Libya, but perhaps a lesser rate of DKA in Denmark, probably because of better patient education. If we can generalize this incidence rate in Benghazi city to the 532,399,1 populations in the whole country, we estimate that there were 2167 DKA episodes (1817 adults and 350 children) in Libya during the year 2007. Most of the episodes were due to type-1 DM, while around 27.7% were due to type-2, which is much higher than the 15% previously reported by Roaeid between 1997 and 1999,1 and also more than 11.6% reported by El-sharief from Tripoli Medical Center (TMC).2
The mean age of all patients was 33 years, which is higher than what was previously reported from Benghazi (28.9 to 29.2 yrs).1,3 However patients with type-2 DM were significantly older than patients with type-1 (59.5 and 22.8 years respectively [p-value: <0.001]) and this is likely due to type-2 DM usually developing in adults older than 40 years while type-1 DM tends to starts among much younger age groups.
The approximately equal male to female ratio contrasts with what has been previously demonstrated in Benghazi where a female preponderance was observed.1,3 Sex ratio among Libyan patients in this study was nearly equal (male: female ration = 1:0.98), while non-Libyans showed male dominance (males: females ratio 2.25:1), which is similar to the previously reported figures from Tripoli,2 This male preponderance among non Libyans with DKA is possibly because most of non-Libyan citizens are young male workers.
Unlike developed countries where infection is the most common precipitating factor for DKA,16 insulin disruption was the major precipitating factor for DKA in the studied patients (35%); which is similar to what was reported by El-sharief from TMC (36.7%),2 and less than 54.4% reported from Saudi Arabia.17 However, it is worth mentioning that the rate of DKA due to treatment disruption showed a significant reduction in Benghazi from nearly 64% between the years 1997 and 1999,1 to 35% in the current study (2007); this reflects an improvement in patients compliance and education. Infection ranked the second in adults and the third in children as a precipitating factor; this is probably because patients fail to realize that they need to increase their insulin dosage during sick days, which again highlights the importance of patient education. In our opinion more than half of all DKA episodes in this study (due to insulin omission and infection) were potentially preventable episodes with good patient education and proper out-patient management.
Fatigue, polyuria, abdominal pain and vomiting appeared to be the most common presenting symptoms in our study, which is similar to other national, and regional reports.2,3,18 Only 3.5% of all patients were in a coma at presentation as compared to 25% reported from Nairobi,19 this is possibly because the condition is tends to be more severe among blacks and may be because of the easy availability of immediate free healthcare services in Libya which could contribute to earlier presentation, hence less severe clinical features. The mean duration of symptoms before presentation to the hospital was 3.3±3 days with about one-third of the patients presented within the same day as the onset of symptoms and two-thirds within 72 hours; this relatively early presentation to outpatient department probably contributes to the low rate of serious clinical features at presentation like convulsion and coma. However, one-third of the patients presented later than 3 days after the onset of symptoms, which is a quite a long period and puts the patient at risk of more severe DKA and more serious complications. We believe that proper patient education will play an important role in early presentation. The duration was longer in patients who were not known diabetics before presentation (11.7 vs. 2.9 days; p=0.000), possibly because they did not quickly realize what was going on.
Moreover, about half of all the episodes were managed in the general medical word, while nearly three-forth of the severe cases were managed at ICU. The place where patient management takes place may have an effect on the mortality rate, the rate of complication and the cost of management. The mean duration of hospitalization was 5.4±4.2 days although some patients (20%) were hospitalized for more than one week for treatment of the precipitating factors and/or complications or for social reasons. This is similar to the average length of staying given by other national reports.1,2 However, this is longer than the USA average length of stay for DKA which is 3.6 days,20 and longer than the duration reported from southern Jordan where the average length of staying was 3.4 days.21 Moreover, patients who were managed at ICU stayed significantly longer than those managed in general medical wards this longer hospitalization results in higher cost and an increased risk of hospital acquired infections.
The morality rate was considerably high in this study (11.7%) and this is similar to that reported from Tripoli (9.4%),2 and Benghazi (10%),3 but it is much higher than what has previously been reported by Roaeid from the same city (3.8%) between 1997 and 1999.1 Mortality was also worse than the figures from Saudi Arabia,17 and Jordan,21 where the mortality rates were 2.9%, and 4.8%, respectively. The reason behind this high mortality rate is not clear and needs to be explored further in future studies. The patients who died had significantly longer duration of DM (9.5 vs. 5.4; p=0.004), which may indicate that they were more likely to suffer from the chronic complications of diabetes and this naturally will increase the risk of death, particularly given that they were significantly older (59 vs. 29.7; p=0.000), and with more co-morbidity (66.6% vs. 13%; p=0.000). The patients who died also had a significantly higher rate of co-morbidities and had significantly faster respiratory rate, lower blood pressure, higher urea and lower platelet count at presentation, which could possibly mean that these factors are either markers or risk factors for increased mortality, and thus patients with such clinical and biochemical abnormalities should be treated cautiously.
Children with DKA exhibited no mortality at all, not merely because the children were significantly younger with less frequent co-morbidities (2% vs. 23%; p=0.001) and shorter duration of DM (2.2 vs. 6.8 years; p=0.000), but also this may reflect a better standard of DKA managements in the pediatric hospital compared to the adult hospitals. For example, nearly 90% of children with DKA in this study were managed at ICU, while only 36% of adults were managed at ICU.
DKA is more fatal when it occurs in patients with type-2 DM (29.3%) in comparison to patients with type-1 DM (4.9%), this is probably because type-2 DM patients are significantly much older (59.5 vs. 22.8; p=0.000) and more likely to have significant co-morbidities (46% vs. 9%; p=0.000).
Since this is a retrospective analysis, we depended mainly on what is written in the hospital records, which can sometimes lack full descriptions and the exact details of specific aspects of the patients’ symptoms, and the exact duration of each symptom. Also, the details of residence of a few patients were missing in the records, thus we cannot be 100% sure that they were really living in Benghazi. Similarly, there might be some diabetic patients from Benghazi who developed DKA but was treated some where else, outside Benghazi, and thus they were not included in this study.
In addition, we acknowledge that one of the limitations in this study is the lack of multivariate analysis of confounding variables, particularly those affecting the DKA mortality. However, despite of these limitations, we think that this study was able to elicit important epidemiological information about this condition in Libya, perhaps most notable of which is its high incidence and high mortality.
Conclusion
DKA is a common and costly condition in Libya with a high mortality rate. A considerable number of DKA episodes are potentially preventable with good patient education. The mortality rate for DKA is quite high in Libya and this endorses the importance of high standards of management, as well as using a standardized formal treatment protocols. Older age, co-morbidities and longer duration of diabetes are associated with increased risk of mortality; therefore, such patients should receive extra attention during management.
Acknowledgements
The authors reported no conflict of interest and no funding was received for this work.
References
1. Roaeid R, Kablan A. Diabetic Ketoacidosis in Benghazi characteristics and outcome in 211 patients. Garyounis Med J 2004;21(1):11-14.
2. EL-sharief H J. Diabetic Ketoacidosis TMC experience. Jamahiriya med J. 2006;5 (1):51-54.
3. Elmehdawi RR, Elmagerhei HM. Profile of diabetic ketoacidosis at a teaching hospital in Benghazi, Libyan Arab Jamahiriya. East Mediterr Health J 2010 Mar;16(3):292-299.
4. Seyoum B, Berhanu P. Profile of diabetic ketoacidosis in a predominantly African American urban patient population. Ethn Dis 2007;17(2):234-237.
5. Newton CA, Raskin P. Diabetic ketoacidosis in type 1 and type 2 diabetes mellitus: clinical and biochemical differences. Arch Intern Med. 2004. 27;164 (17):1925-31.[REMOVED HYPERLINK FIELD]
6. Umpierrez GE, Smiley D, Kitabchi AE. Narrative review: ketosis-prone type 2 diabetes mellitus. Ann Intern Med 2006 Mar;144(5):350-357.
7. Kadiki OA, Gerryo SE, Khan MM. Childhood diabetes mellitus in Benghazi (Libya). J Trop Pediatr 1987 Jun;33(3):136-139.
8. Roaeid RB. Hospital admissions of diabetic patients in Benghazi. Diabetes International 2002;12(1):24-25.
9. Roaeid RB, Elgazwi I, El-Sharef KB. El- Bash A, El-Fageh HA. Admission Patterns and Outcome in an Adult Medical Intensive Care Unit in Benghazi. Garyounis Med J 2005;22(1):61-66.
10. Lakhdar AA, Elharboush S. Characteristics and outcome of ketoacidosis in Libyan diabetic patients. Diabetes Int 1999;16(6):171-173 .
11. Kadiki OA, Roaeid RB. Prevalence of diabetes mellitus and impaired glucose tolerance in Benghazi Libya. Diabetes Metab 2001 Dec;27(6):647-654.
12. Kadiki OA, Roaeid RB. Incidence of type 1 diabetes in children (0-14 years) in Benghazi Libya (1991-2000). Diabetes Metab 2002 Dec;28(6 Pt 1):463-467.
13. Kitabchi AE, Umpierrez GE, Murphy MB, Kreisberg RA. Hyperglycemic crises in adult patients with diabetes: a consensus statement from the American Diabetes Association. Diabetes Care 2006 Dec;29(12):2739-2748.
14. Kitabchi AE, Umpierrez GE, Murphy MB, Barrett EJ, Kreisberg RA, Malone JI, et al; American Diabetes Association. Hyperglycemic crises in diabetes. Diabetes Care 2004 Jan;27(Suppl 1):S94-S102.
15. Henriksen OM, Røder ME, Svendsen OL. [Diabetic ketoacidosis in Denmark–registry-based estimation of incidence and mortality. Secondary publication]. Ugeskr Laeger 2007 Jun;169(24):2335-2337.
16. Wallace TM, Matthews DR. Recent advances in the monitoring and management of diabetic ketoacidosis. QJM 2004 Dec;97(12):773-780.
17. Qari FA. Precipitating factors for diabetic ketoacidosis. Saudi Med J 2002 Feb;23(2):173-176.
18. Razavi Z. Frequency of ketoacidosis in newly diagnosed type 1 diabetic children. Oman Med J 2010 Apr;25(2):114-117.
19. Mbugua PK, Otieno CF, Kayima JK, Amayo AA, McLigeyo SO. Diabetic ketoacidosis: clinical presentation and precipitating factors at Kenyatta National Hospital, Nairobi. East Afr Med J 2005 Dec;82(12)(Suppl):S191-S196.
20. Diabetes data and trends. Centers for Disease Control and prevention. ([http://www.cdc.gov/Diabetes/statistics/dkafirst/fig2.htm] accessed 5 September, 2009).
21. Tahboub I, Shalan JB. Diabetic ketoacidosis in southern Jordan: five-year experience. East Meditter health J. 2000;6(5-6):1035-1038.
|