|
Abstract
Objectives: Low Birth Weight (LBW) has an important role in the mortality and morbidity of neonates and the incidence of LBW may vary across different environments. The aim of this study was to determine the incidence and some related factors of LBW in Mazandaran province, Northern Iran.
Methods: In this longitudinal study, all live births that were born in 5 maternity hospitals in Mazandaran province, north of Iran in 2011, were evaluated. Data including birth weight, sex, maternal age, gestational age, living location, number of pregnancy and delivery, as well as multiple births were recorded in medical files. LBW neonates were compared with neonates whose birth weight was more than 2,500 gram (control group).
Results: Out of 3792 infants, 2.9% (CI 95%: 2.3-3.3) were of low birth weight. Sixty percent of the infants in the LBW group and 8.3% in the control group were preterm, (p<0.001). In the LBW group, 22.2% were multiple births, while 0.5% in control group were multiple births (p<0.001), but other variable distributions such as sex, living location and mother's age did not differ between the LBW and the control groups (p>0.05).
Conclusion: Results show that the incidence of LBW in Mazandaran was low and prevention of preterm labor, educational intervention programs for high risk can be effective in the prevention of low birth weight.
Keywords: Low birth weight; Neonate; Incidence.
Introduction
According to the World Health Organization, Low Birth Weight (LBW: defined as weight at birth of less than 2500 gram irrespective of gestational age),1 and Very Low Birth Weight (VLBW: defined as weight equal to 1500 gram or less), have a high risk of mortality and disease during the first year of life.2 Risk of death in LBW infants increased forty-fold in comparison to normal birth weight babies.3 The risk of respiratory and diarrhoeal disease,4 impaired growth and mental development, as well as poor outcomes in young adulthood is high in LBW.5,6 LBW is caused by preterm birth, intrauterine growth retardation or both. Over the past two decades, rates of LBW have increased. According to UNICEF statistics, the overall rate of LBW stands at 17%, it is 6% in developed countries and 21% in developing countries.7
Based on the results of studies from Iran, the LBW rate was 11.8% in Zahedan city in the south-east of Iran,8 and 8.8% in Yazd, the central city of Iran.7 As the prevalence of LBW is one of the most important health indices and as the prevalence of LBW is a function of social status and lifestyle, it is important to determine the incidence and risk factors for LBW in different areas.8 There have been a number of previous studies on LBW in the Islamic Republic of Iran, but these studies were done in local areas while this study was done in a large area in Northern Iran. The aim of this study is to determine the incidence and some associated factors of LBW in Mazandaran province, Northern Iran.
Methods
This was a longitudinal study performed from 01 January 2011 to 31 December 2011. All live births in 5 primary maternity hospitals in Mazandarn, Northern Iran, were evaluated. The neonates were divided into two groups according to the birth weights. Birth weight was measured by digital scale. All LBW neonates were classified as the study group, while those whose birth weight exceeded 2,500 gram served as the control group. LBW were subdivided into very low birth weight (less than 1500 g) and extremely low birth weight (less than 1000 g) groups. Variables such as sex, maternal age, gestational age, living location, number of pregnancy and delivery, as well as multiple births for both groups were recorded in a special questionnaire. Gestational age was calculated using either the first day of the last normal menstrual period or estimated by obstetric sonography. Data was analyzed using the SPSS 15. Chi-square test and fisher’s exact test were used to compare categorical variables between the groups. Logistic regression was used to find any association between LBW and other variables. Rate ratios were calculated for incidence of LBW with 95% confidence interval (CI 95%). A p-value less than 0.05 was considered to be statistically significant.
Results
In this study, 3792 infants were included. The total number of LBW babies was 108 with an incidence of 2.9% (CI 95%: 2.3-3.3). Out of these LBW neonates, 11 (10.2%) were classified as very low birth weight and 8 (0.2%) as extremely low birthweight. Ten neonates (0.3%) included in the control group were macrosomia. Table 1 shows the distribution of sex, living location, gestational age, multiple births and maternal age in the control and the LBW groups.
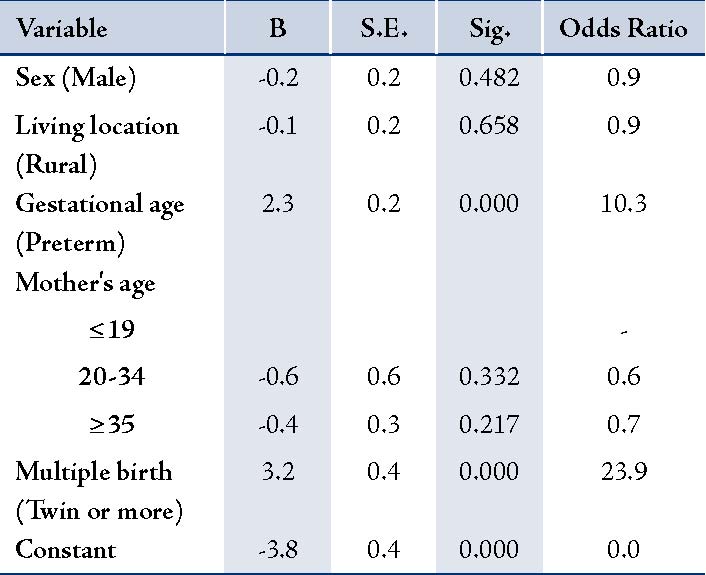
Sixty percent of the infants in the LBW group and 8.3% in the control group were preterm, and this difference was significant (p>0.001). In the LBW group, 22.2% were multiple births, while 0.5% in the control group were multiple births and showed that multiple pregnancies were more prevalent in the LBW group (p>0.001), but other variable distribution did not differ between the two groups (p>0.05). Regression analysis is shown in Table 2.
Table 1: The distribution of variables in LBW and control neonates in Mazandaran.
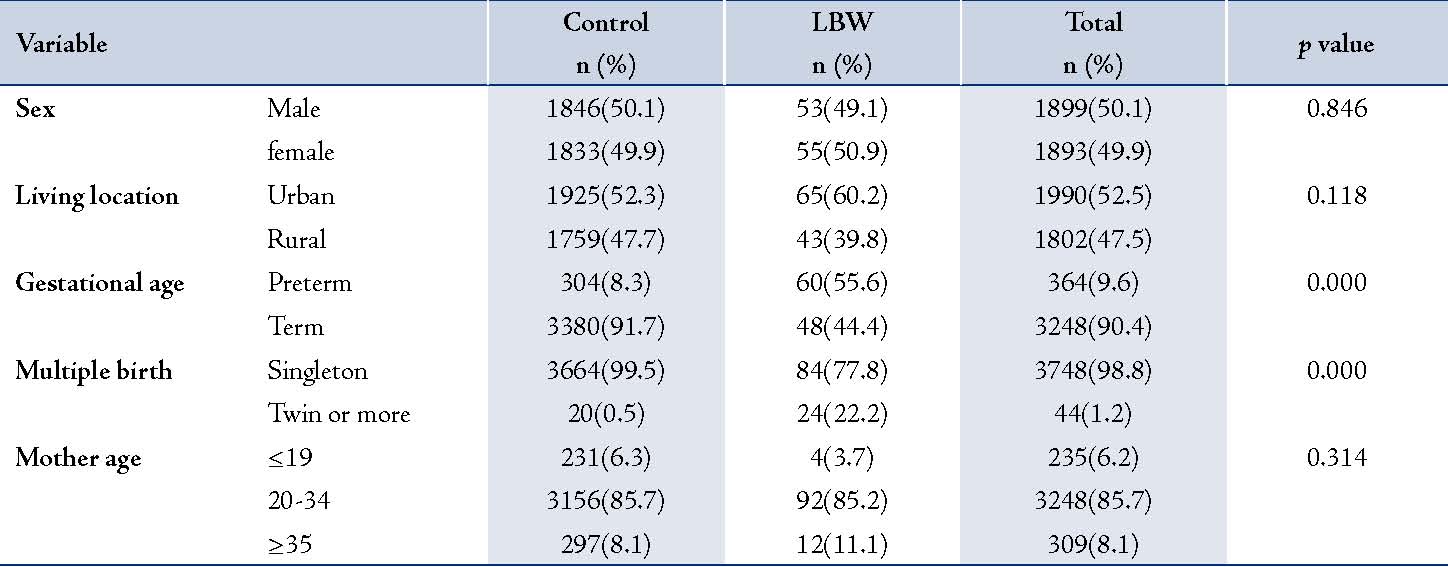
Table 2: Logistic regression findings between LBW and other variables.
Discussion
Low birth weight has a significant economic burden for the health system and families.9 It is one of the most important factors for perinatal mortality and morbidity in both developing and developed countries.10 We found a LBW rate of 2.9% (CI95%: 2.3-3.3) of all deliveries. Our findings are lower than the national and international rate, reported in other studies. The prevalence in other Iranian cities was 4.2% in Tehran,11 4.2% in Tonekabon,12 6.2% in Babol,13 6.3% in Gorgan,14 8.8% in Yazd,7 9.6% in Bushehr,15 and 11.8% in Zahedan.8 In USA and England, LBW rates have been reported to be 7.7% and 7.8% respectively.16,17 LBW rate reported from Korea was 7.2%.18 The prevalence of LBW is nearly 50% in South Asia; whereas, it is reported to be 10.61% in Turkey.10 Thus, the birth weight shows a great degree of variation from country to country and even from one region to another within the same country.10 Therefore, it is essential to have data on local patient population. The health facilities are the most advanced in all cities in Mazandaran province and it is only natural that the LBW rate in this region is low. Other possible factors for this difference include; ethnicity, nutritional status, socioeconomic conditions and maternal health.
Parallel to the study results of Shin et al.18 and Akin et al.10 we could not find any gender majority among LBW deliveries. In the present study, multiple births was a risk factor for LBW, similar to other studies conducted in Iran,7,8,13 Italy,19 and Japan.20 The association between LBW and maternal age is well documented in many studies. Shin et al.18 and Hosain GM et al.21 showed that maternal age and birth weight were strongly related and infants born to older mothers were heavier. The results of this study were not in parallel with those of the two above-mentioned studies, but it is similar to the study by Akin et al.10
As a limitation of present study, other causes of low birth weight like maternal diseases such as hypertension, renal disease and diabetes; congenital malformations in the LBW babies and maternal weight gain during pregnancy were not evaluated because risk factors of low birth weight were secondary objective and not studied completely.
Conclusion
The incidence of LBW in Mazandaran region of Iran was low compared to the national and international rates. Prevention of preterm labor and educational intervention programs for high risk populations can be effective in decreasing the incidence of low birth weight. We also recommend that mothers at risk be provided with adequate prenatal and healthcare facilities.
Acknowldegements
We are very grateful to the babies and their mothers who participated in the study. The authors would like to thank Dr. Alizadeh-Navaei for manuscript preparation. No funding was received for this work.
References
1. Sicuri E, Bardají A, Sigauque B, Maixenchs M, Nhacolo A, Nhalungo D, et al. Costs associated with low birth weight in a rural area of Southern Mozambique. PLoS One 2011;6(12):e28744.
2. Ballot DE, Chirwa TF, Cooper PA. Determinants of survival in very low birth weight neonates in a public sector hospital in Johannesburg. BMC Pediatr 2010;10:30.
3. Goldenberg RL, Culhane JF. Low birth weight in the United States. Am J Clin Nutr 2007 Feb;85(2):584S-590S.
4. Lira PI, Ashworth A, Morris SS. Low birth weight and morbidity from diarrhea and respiratory infection in northeast Brazil. J Pediatr 1996 Apr;128(4):497-504.
5. Bhutta AT, Cleves MA, Casey PH, Cradock MM, Anand KJ. Cognitive and behavioral outcomes of school-aged children who were born preterm: a meta-analysis. JAMA 2002 Aug;288(6):728-737.
6. Hack M, Flannery DJ, Schluchter M, Cartar L, Borawski E, Klein N. Outcomes in young adulthood for very-low-birth-weight infants. N Engl J Med 2002 Jan;346(3):149-157.
7. Golestan M, Akhavan Karbasi S, Fallah R. Prevalence and risk factors for low birth weight in Yazd, Iran. Singapore Med J 2011 Oct;52(10):730-733.
8. Roudbari M, Yaghmaei M, Soheili M. Prevalence and risk factors of low-birth-weight infants in Zahedan, Islamic Republic of Iran. East Mediterr Health J 2007 Jul-Aug;13(4):838-845.
9. Sicuri E, Bardají A, Sigauque B, Maixenchs M, Nhacolo A, Nhalungo D, et al. Costs associated with low birth weight in a rural area of Southern Mozambique. PLoS One 2011;6(12):e28744.
10. Akin Y, Cömert S, Turan C, Ünal O, Piçak A, Ger L, et al. Increasing Low Birth Weight Rates: Deliveries in a Tertiary Hospital in Istanbul. Iran. J Pediatr 2010;20(3):284-290.
11.Reshadatjoo H, Faghihzadeh S, Parsay S. (The interval between births and the most important risk factors of pregnancy). Daneshvar 1996;4(13/14):17-24. Persian.
12. Hosseini SZ, Bahadori MH, Fallah Bagher Sheidaei H. [Incidence of low birth weight and associated risk factors during March 2002-03 in Tonekabon, Iran]. J Mazandaran Univ. Med Sci 2006;49:110-113. Persian.
13. Hajian K. [The rate of LBW and some of its risk factors in Babol in 1998]. J Mazandaran Univ. Med Sci 2000;26:49-55. Persian.
14. Khori E, Vakili MA, Golalipour MJ. [The rate of LBW in Gorgan city and some related factors]. J Gorgan Univ. Med Sci 1999;1:46-53. Persian.
15. Mohammadi MM, Hashemi M, Mohammadi Baghmollaei M. [Determination of correlation of some socio-economical factors with low birth weight (LBW) in Bushehr port.] J Bushehr Univ. Med Sci 1997;1:25-28. Persian.
16. Martin JA, Hamilton BE, Sutton PD, Ventura SJ, Menacker F, Munson ML. Births: final data for 2002. Natl Vital Stat Rep 2003 Dec;52(10):1-113.
17. Bell R. Trends in birthweight in the north of England. Hum Fertil (Camb) 2008 Mar;11(1):1-8.
18. Shin SM, Chang YP, Lee ES, Lee YA, Son DW, Kim MH, et al. Low birth weight,very low birth weight rates and gestational age-specific birth weight distribution of korean newborn infants. J Korean Med Sci 2005 Apr;20(2):182-187.
19. Nobile CG, Raffaele G, Altomare C, Pavia M. Influence of maternal and social factors as predictors of low birth weight in Italy. BMC Public Health 2007;7:192.
20. Takimoto H, Yokoyama T, Yoshiike N, Fukuoka H. Increase in low-birth-weight infants in Japan and associated risk factors, 1980-2000. J Obstet Gynaecol Res 2005 Aug;31(4):314-322.
21.Hosain GM, Chatterjee N, Begum A, Saha SC. Factors associated with low birthweight in rural Bangladesh. J Trop Pediatr 2006 Apr;52(2):87-91.
|