|
How to cite this article
Badar F, Jha A, Azfar SH, Ullah E. A 55-year-old Man with Painless Joint Swelling. Oman Med J 2012 Nov; 27(6):509-510.
How to cite this URL
Badar F, Jha A, Azfar SH, Ullah E. A 55-year-old Man with Painless Joint Swelling. Oman Med J 2012 Nov; 27(6):509-510. Available from http://www.omjournal.org/fultext_PDF.aspx?DetailsID=317&type=fultext
Introduction
A 55-year-old man presented with swelling of left knee for the past one month. He also complained of episodes of joint locking. There was no history of pain, fever or trauma. Physical examination revealed localized increase in temperature of the skin, a large joint effusion, and decreased range of motion. His total leukocyte count was normal; ESR was raised to 48 mm in the first hour. Antero-posterior and lateral radiograph of the knee revealed large joint effusion with no bony abnormality. Subsequent magnetic resonance imaging (MRI) performed revealed joint effusion with lobulated enhancing synovial masses around the knee joint. The masses appeared low signal on T1 weighted (Fig. 1), T2-weighted and Proton density image (Fig. 2a). “Blooming effect” with marked loss of signal was seen on GRE-DESS image (Fig. 3). FNAC and joint aspiration was hemorrhagic. Synovial biopsy was performed and revealed villi and nodule with extensive hemosiderin deposition and abundant multinucleated giant cells.

Figure 1: Sagittal T1-weighted MRI shows lobulated low signal synovial masses in knee joint and popliteal bursa with erosion of tibial condyle.
Questions
- What are the differential diagnoses and diagnosis?
- What is the management for this case and the role of MRI in it?'

Figures 2a and 2b: Sagittal and axial proton density (PD) weighted MRI shows joint effusion with lobulated and frond-like heterogeneous hypointense lesion within the joint and bursa.
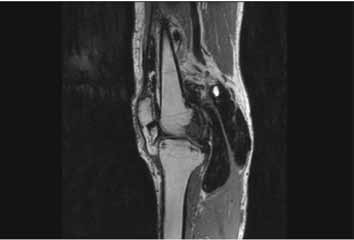
Figure 3: Shows marked loss of signal with “Blooming effect” on GRE-DESS image.
Answer
The differential diagnoses of hypointense synovial masses on T2 weighted MRI are; pigmented villonodular synovitis (PVNS), synovial osteochondromatosis, hemophilic arthropathy, and amyloid deposition. The diagnosis was PVNS made by characteristic MRI and histopathological features.
Complete synovectomy is the most common treatment; however, it is often not possible in large joints because of the complexity of the joint structure. Recurrence rates are high. Other treatment options include radiation therapy, pharmaceutical modulation of the disease, or a combination of these approaches. MRI has a very important role by demonstrating the characteristic finding and allows for the preoperative non-invasive diagnosis.
Discussion
PVNS is a rare proliferative lesion of the synovium of joints, tendon sheaths and bursae.1 The etiological factors are still a matter of debate though certain studies have suggested a neoplastic or inflammatory origin. PVNS is mostly monoarticular with the knee being the most commonly affected joint being involved in 80% of the cases. Other commonly involved joints include hip, ankle, shoulder and elbow.2 This disease can manifest in any group though the most commonly affected individuals are adults, around 20-50 years of age, with no sex preponderance.
PVNS is known to occur in both local and diffuse forms with the diffuse involvement being more common. Clinically, it is a slow growing process with nonspecific presentation. The spectrum of complaints may vary from subtle features like minimal pain or swelling around the joint to serious manifestations like marked stiffness, joint instability, or grossly reduced movements.
On plain radiographs, the findings are nonspecific, with joint effusion being the most commonly detected abnormality. In advanced stages joint erosions may be seen with sclerosis of the articular surfaces. They are quite evident in hip and shoulder while less commonly seen in capacious joints like knee.3
MR is the imaging modality par excellence for the diagnosis of PVNS. Images reveal a synovial-based mass that affects the entire or part of the joint and displays low signal intensity on T1- and T2-weighted pulse sequences. Magnetic susceptibility artifact (blooming) within the affected joint space on GRE images is also characteristic. Although the degree of enhancement in PVNS can vary, marked enhancement of the synovium is common due to the hypervascular nature of the disease.
The major differentials to be considered while investigating for PVNS include amyloid arthropathy, hemophilia-related arthropathy, and synovial chondromatosis. The factors in favor of amyloid arthropathy are multifocal involvement and low signal intensity on T1- and T2-weighted images in absence of blooming artifact. The presence of osseous deformities favors hemophilia related arthritis over PVNS. Synovial chondromatosis may be considered in cases where multiple intra-articular bodies are seen on plain radiography or their cartilaginous nature revealed by MR imaging.
The ideal treatment for PVNS is total synovectomy which is usually not possible in large joints owing to presence of bursae and recesses, where partial resection is favorable. External beam and intra-articular radiation therapy using yttrium has been reserved for recalcitrant disease due to its potential for causing transformation into malignant PVNS. For advanced cases with joint destruction, arthrodesis and arthroplasty are advocated.4
References
1. Farrokh D, Annaert JM, Fabeck L, Theunis A, Delince P. Localized pigmented villonodular synovitis of the knee with bone involvement mimicking a benign bone tumor: CT and MR findings. JBR-BTR 2001;84:253-5.
2. Dorwart RH, Genant HK, Johnston WH, Morris JM. Pigmented villonodular synovitis of synovial joints: clinical, pathologic, and radiologic features.AJR Am J Roentgenol 1984;143:877-885.
3. Lin J, Jacobson JA, Jamadar DA, Ellis JH. Pigmented villonodular synovitis and related lesions: the spectrum of imaging findings. AJR Am J Roentgenol 1999;172:191-197.
4. Ofluoglu O. Pigmented villonodular synovitis. Orthop Clin North Am 2006;37:23-33.
|