| |
Abstract
Objectives: Limited research has been undertaken on suicide in developing countries. This paper aims to investigate characteristics of suicide attempts in Hamadan district of Iran.
Methods: A prospective study was conducted in all university hospitals in the Hamadan district of Iran and patients admitted for attempted suicides were included. All cases were assessed by psychiatrists and visited by two trained interns of Medicine.
Results: The incidence rate per 100,000 persons of attempted suicides was 228.6 for males and 263.1 for females; moreover, 344.9 for rural areas and 222.7 for urban areas. The suicide attempt was the highest in the 15 to 24 age category for both sexes and regions.
Conclusions: Suicide is a complex, long-term outcome that requires multifaceted theoretical constructs for the appropriate study of its antecedents. Findings of this study along with other studies in Iran revealed that unemployed men, housewives, and rural women, high-school students, and those with a low level of education were at higher risk of suicidal behaviors.
Keywords: Suicide; Attempted suicide; Iran.
Introduction
Suicide is considered as an important public health problem in many countries,1,2 and is a major, but largely preventable,3 cause of mortality in teenagers and young adults.4-6 It is considered as the third leading cause of death between the ages of 15 to 34 years.1,7 Even in North America, it has been identified as one of the most important causes of potential life years lost and contributes substantially to economic burden.1,4 Based on the World Health Organization (WHO) report, it contributes to 0.3 per 100,000 mortality in the male population in Iran.8 However, in some studies from Iran, suicide rates are as high as 63 per 100,000 persons.9 According to the WHO, suicide is among the top 20 leading causes of death worldwide, which results in nearly one million deaths per ten to twenty million suicide attempts each year.10 As such, suicidal behavior is a significant global public health problem.7 Suicide indicates a severe level of mental health problems,11-13 which is in turn due to many political,14 cultural, social, and economic factors,12,14-18 such as financial problems, spousal infidelity, family conflicts, and frustrated teenage romance,6 along with the availability of easy instruments for suicide.19 Some studies have reported the association between low socioeconomic factors and higher suicide attempt rates,5 especially in developing countries, where welfare systems were limited or absent. Thus poverty, unemployment, and financial difficulties have been identified as important causes for suicide.3
Limited research into suicide has been undertaken in developing countries where religious, cultural, and social values are varied and play an important role. In this regard,3 developing countries should pay closer attention to mental health research, due to the imbalance between the burden of mental disorders and the resources for managing them.20 Suicide is a multifactorial problem of age, gender, race, socioeconomic, marital, and many other personal and societal status.1,3,4,7,21 Therefore, the incidence and pattern of suicide may vary in different nations.1,4 As a result, different studies have shown different demographic conditions among population subgroups.
Suicide is a continuum of ideation, plans, and attempts.12 Studies focusing on completed suicides provide only the tip of the iceberg in terms of information.17 Most literatures have been devoted to completed suicides. This paper investigates some characteristics of suicide attempts (SA), "which are powerful predictors of further suicidal behavior,22 in Hamadan, where it is believed to have the highest rates of suicide deaths in Iran (13.5 per 100,000 persons in comparison with 5.7 per 100,000 persons mean for the entire country).23
Methods
This study was aimed at determining the demographic and epidemiological characteristics of SAs in the Hamadan district of Iran. A prospective study was performed during a one year period from 21 March 2007 to 20 March 2008. Unlike information on completed suicide, there is no single primary data source for information on SA,1 therefore, all university hospitals in Hamadan, including Be'sat, Farshchian, Mobasher, and Ekbatan, and their wards for burn, surgery, pediatric, emergency, ICU, internal medicine, psychiatric and poisoning were investigated for any admitted SA, as defined as a self-inflicted injurious behavior with an intention to die. All admitted SAs were assessed by psychiatrists routinely, then registered in the HIS system of these hospitals, and finally visited by two trained interns of Medicine, who completed data-gathering checklists by interviewing patients or relatives, and scrutinizing the patient’s records. Interviews were conducted after stability and ability to response to questions before discharge. The definition of SA included only behaviors that matched the following three conditions: i) SAs that had led to hospitalization, ii) the trauma being an act of intentional self-inflicted injury, and iii) the trauma had to be included in a specified list of traumas traditionally associated with SAs such as cutting of wrist, self-immolation, hanging, and/or self-poisoning.24
A National Population and Housing Census survey is conducted every 5 years in Iran. Based on the last census,25 the Hamadan district had a population of 637,304 people at the time of the study, with a male/female ratio of 1.02:1 and a urban/rural split of 4.3:1. There were five university hospitals in the city of Hamadan which cover the entire district of Hamadan’s population. One hospital specifically for Gynecology and Obstetrics was excluded from this study. SA incidence rates were estimated by relating the numbers of SAs to 100,000 numbers of persons as estimated from the 2006 National Population Census.25 Admitted suicidal individuals living in other districts at the time of the study were excluded. Further, this project was approved by Hamadan University of Medical Sciences Deputy of Research and patients names and confidentiality was respected.
Statistical analysis was conducted with SPSS version 11 for Windows (SPSS Inc., Chicago, IL, USA). The analysis was mostly descriptive in nature; differences between various groups were evaluated with the unpaired Student’s t-test and chi-square test. A value of p less than 0.05 was considered significant.
Results
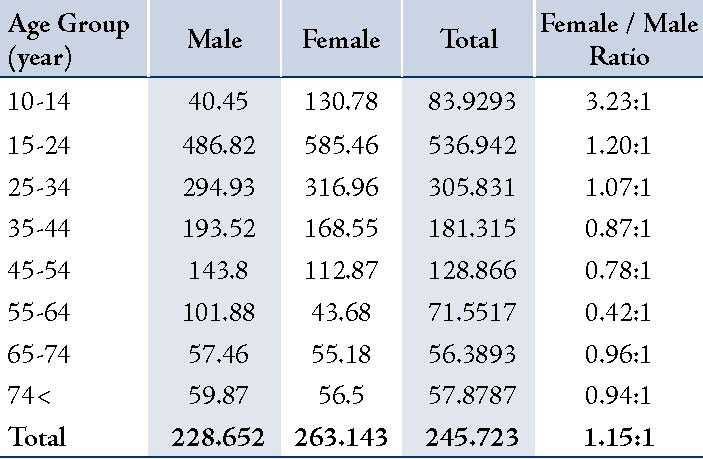
During the study period, 1,566 SAs were investigated, including 830 (53%) females and 736 (47%) males, (Table1). The mean age of persons who attempted SA was 27.6±11.53 for males, and 24.83±10.67 for females (p<0.001), ranging from 10 to 91 years. The incidence rate per 100,000 persons of SA was 228.6 for males and 263.1 for females; moreover, 344.9 for rural areas and 222.7 for urban areas. The SA, was the highest in the 15 to 24-year-old category in both sexes and regions, (Fig. 1). The distribution of all patients according to age and gender, as depicted in Fig. 1 reveals that rural women under the age of 34 attempted more SA than other cohorts; however, men from rural areas between the ages of 35 and 64 years had the highest incidence of SA, and after this age group, urban people attempted suicide more than rural persons. It can be stated that in both rural and urban areas, females under the age of 34 attempted suicide more than men in the same region; however, this trend reverses after this age group.(Table 2)
In this study, 48 children under the age of 14 attempted SA; this comprised of 12 (1.6%) boys and 36 (4.3%) girls. One girl in this age group was married. Most of the patients were single, but being single was more prevalent among men (p<0.001). Subgroup analysis showed no difference between rural and urban areas in marital status among men or women (p>0.3).
Table 1: Demographic Characteristics of Patients Attempted Suicide
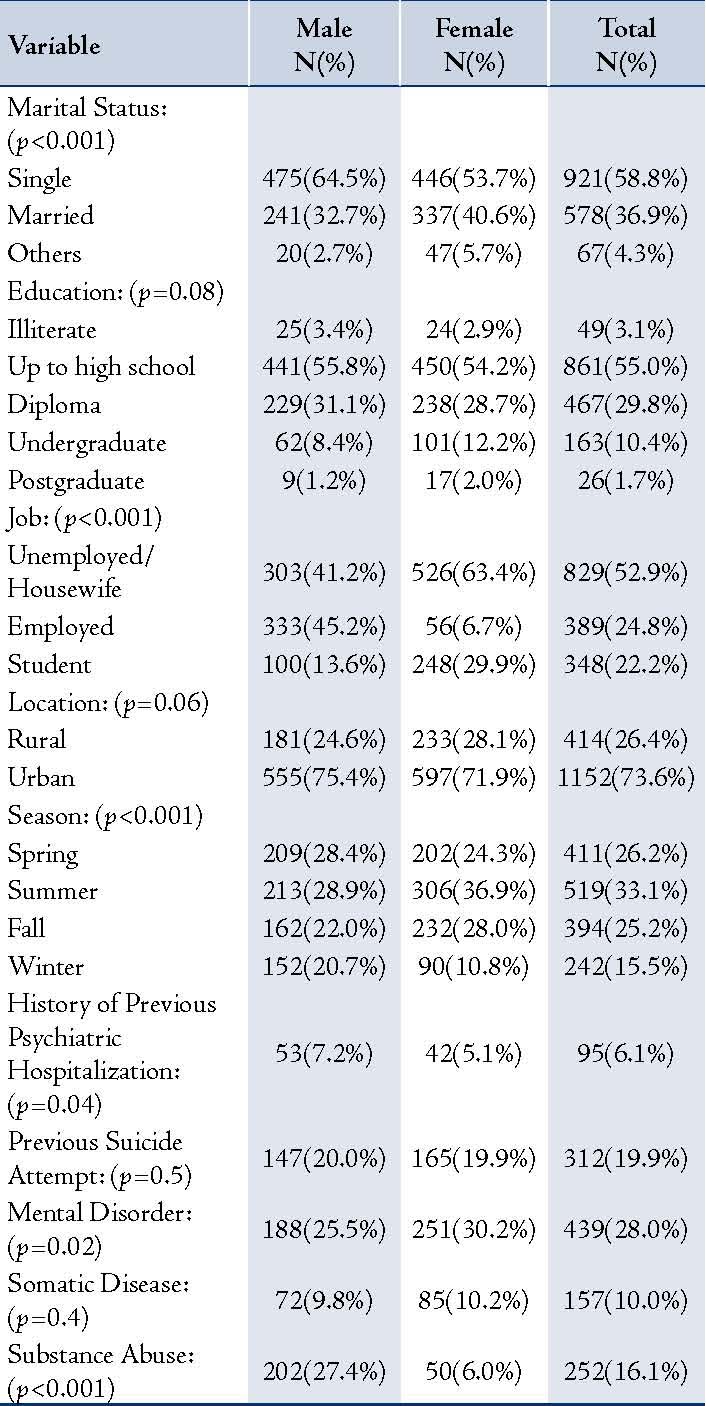
Unemployment was as high as 41.2% in men; however, as is shown in Table 2, it was higher in women, (p<0.001). There was no marked difference between urban and rural men employment rates, with 41.4% of urban and 40.3% of rural males reporting as being unemployed (p=0.5). Unemployment among rural females was higher than urban females, with 58.6% of urban versus 75.5% of rural women reporting as being unemployed (p<0.001).
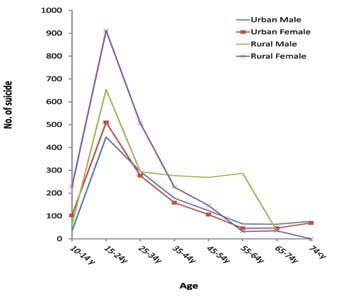
Figure 1: Distribution of SA incidence rates in urban and rural areas (no. of suicide per 100,000 persons) by age and gender
Table 2: SA incidence rates per 100,000 persons by age and gender.
There was no significant educational differences between men and women (p=0.08); however, both men and women in rural areas were less educated than in urban areas (p<0.001). In urban areas 49% were educated below diploma level, 34.7% had a high school diploma, 14% were undergraduates, and 2.3% were postgraduates. However, in rural areas the results were 83.3%, 16,2%, 0.5%, and 0%, respectively. SAs were mainly attempted in the summer. Further, the fewest SAs occurred in the winter for both genders. (Table 1)
Rural men (13.8%) had more somatic diseases than urban men (8.5%; p=0.02) and although this pattern was similar for women, it was not considered statistically significant (p=0.17).
Generally, all women and rural people had a higher history of mental disorder (p<0.02); however, subgroup analysis revealed that differences between urban and rural society (male and female) either in rural or urban areas were not statistically significant. The only statistically meaningful (p=0.01) difference was between rural and urban females. The prevalence of a history of mental disorder resulted as follows: rural females (36.1%); rural males (29.8%); urban females (28.0%); urban males (24.1%). Regression analysis showed that rural females had a greater history of mental disorder (p=0.006).
The highest amount of substance abuse was seen among rural men (29.1%); whereas, the lowest amount was among rural women (5.6%). There were not any significant differences between rural and urban areas in each gender group in this regard (p>0.2). The highest amount of previous SA was revealed in rural females (24.0%), which was significantly higher than urban females (p=0.03), there were not any significant differences between other groups.
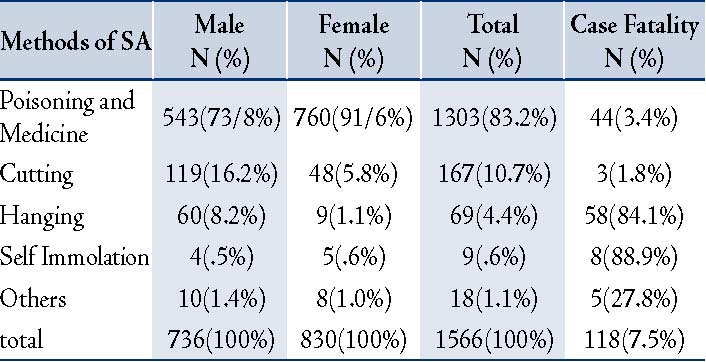
The results also show that the most common method of SA was poisoning, which was used in 1,303 (83.2%) of cases studied. Table 3 presents methods of SA by gender, shows more violent methods used by men than women (p<0.001). One drowning and eleven jumping were reported; however, there was no firearm reported in this study.
Table 3: The most common methods of SA in Hamadan district
Discussion
According to this prospective study, 1,566 patients were hospitalized following suicide attempts during one year in the Hamadan district, these accounts for a total incidence rate of 245.7 per 100,000 persons. Further, this is considerably higher than previous studies of SA in Ilam province, which had reported the mean annual SA rates for the female and male as 64.5 and 41.8 per 100,000 persons, respectively.4 Moreover, the finding of this study is also higher than the 102 per 100,000 person annual rate reported in Kermanshah province.26
In terms of gender and age, SA rates have been higher in women than men in most studies.5,6,12,22,24,27-33 For instance, it was 2.38:1 in an Australian study, and 1.7:1 in another European one.5 In the current study, similarly to other studies which have been conducted in Iran,2-4,14,21,29,34 females were more vulnerable to SA, (Table 1). The total female-male ratio was 1.15:1 per 100,000 persons, (Table 2) while in another study it was 2.4:1,35 suggesting "the high rates of SA in young Iranian women have multiple causes: a vicious cycle of social humiliation and coercion, economic dependence, family insecurity, fear for their children's lives as well as themselves, shame, lack of confidence, insults, sexual abuse, and lack of resources to support them" as well as higher rates of depression in women, which is an important risk factor for suicide.6
In contrast to the study from Belgium,27 in which similarly to other studies,3-6,35,36 females were significantly younger than males; however, child SA, which was 3.1% of all SAs, was less than the 7.7% reported in Qazvin,35 which may indicate cultural differences. Corporal punishment, a reason for suicidal thinking especially in women,11 is frequent in lower social classes of Iranian people, which can describe high SA rates in young people. Furthermore, many teenagers are confronted with issues that lead them to experience feelings of stress, self-doubt, pressure to succeed in their studying, and role confusion.2 Table 2 and Fig. 1 show that young people in the 15 to 24 age group are more vulnerable to SA, which can be seen in other studies.2-4,21,29,31,35-37 However, the total rate of 536.942 and rural female rate of 911.912 per a 100,000 population in this age group are much higher than that of other studies. For instance in Australia it was estimated that the annual rate of SA in Perth was 364 for the same age group.5
In this study, 82.4% of all SAs occurred among people below the age of 34, which is similar to the results of other studies from Iran2,4,14,21,34,36-38 and other developing,6,28,39 and developed countries.5,27,40 Higher rates of SA among females younger than 34 may account for social pressures of growing up,4 in addition to women's marital problems; however, preceding men’s rates after this age, may be due to financial difficulties for men who are responsible for earning a livelihood in their years of economic independence.1,4,6,31 Moreover, men do not ordinarily visit psychiatrists or psychologists, coupled with high rates of opium use for males in this age group (Table 1), can result in a vicious cycle of depression-addiction, and hence finally SA.
In this study 2.7% of all SAs occurred after 55 years of age, which resembled other studies in Iran.4 The low rates of elderly suicide, particularly in rural areas (Fig. 1), which did not reveal any SAs after the age of 75, can be largely due to traditional family support and respect for elders in Iranian culture; along with strong family ties and a closely knit social support system in these regions.12
When considering marital status, in some studies,4,21,28,29,35,41 married individuals had the highest rate of SA. In contrast with this study, such as with most other studies,2,3,5,6,14,19,30,34,38,40 SA was mainly observed in single persons. Further, single men had significantly higher SAs than single women (Table 1). This was a reasonable observation in so much as, SA was prevalent among students and young adults under marital ages; moreover, as the marital age has been increasing in the Iranian population, especially among men, who marry about five years older than women. Higher percentage of SA among married women than married men can indicate a miserable condition after marriage for women that may result from patriarchy in Iranian population, especially among lower social class people. This may provide support for the highest SA rate for 15 to 24 year old rural females who are experiencing marital problems, such as parental force for arranged marriages, or assaults by husbands, which are contributing factors towards suicidal thoughts11 in addition to verbal, physical, and sexual abuse by husbands,6 and problems with parents-in-law.21 Generally, could be stated that marriage is more likely to increase the susceptibility of women while protecting men from suicidal behavior.6,31
Urban vs. Rural should that although 1,152 (73.6%) cases were from urban area, the rural to urban ratio per 100,000 persons was 1.54:1, which indicates more SAs in rural regions (Fig. 1). Similar results were reported from Australia,5 and South Korea,17 studies. In yet another analogous study from Iran,35 females in both rural (56.2%) and urban (51.8%) areas had more SAs than men. Moreover, the high incidence rate of 911.9 per 100,000 persons in 15 to 24 year old rural females in the current study can indicate cultural problems, including relationship disputes between daughter-in-law and mother-in-law,6 which are common in lower social class Iranian population.42 Cultural problems could be assumed as serious sources of stress and distress; in addition to limited access to mental health facilities, as well as other reasons previously cited in the Gender and Age section.
The findings of the level of education revealed that most of the study participants (55.0%) had primary or secondary education, and had not completed high school, which is similar to other studies conducted previously in Iran,2,21,34,37 as well as a hospital based study in India.39 In contrast to Ilam,4 where females were less educated, in this study there were no significant educational differences between men and women, although academic women exceeded the men.
In terms of unemployment, some studies have found a strong positive correlation between unemployment rates and SA,5 and ideation,43 especially some specific methods of suicide including self-immolation.36 Unemployment rates among suicide attempters in the current study and the other reports from Iran2,3,21,37 and Canada,30 particularly among women, was high; furthermore, housewives comprised a large number of cases.14,21,34,37,38 During times of high unemployment, the SA rate increases and vice versa.36 A study performed in the Eastern Mediterranean Region (EMR) of the World Health Organization (WHO) revealed that SA rates were higher in all age and sex groups within low and middle-income countries in comparison with high-income countries.18 Another study from Hamadan has reported that family conflict, mental problems and men's unemployment were the most important causes of SAs.38 Although research seem to indicate a positive relationship between unemployment and suicide rates, no causal relationship can be attributed to unemployment and suicide; whereas the causes of unemployment such as mental illness, could account for why they attempted suicide.5
In this study, the previous history of SA, reported by 312 (19.9%) persons, had no gender difference, which was almost the same as 21.5% patients in another study from Iran,35 but lower than another report (28%),2 though higher than a previous study in Hamadan.37
Medical illness is a stressor in older adult suicides,12 which can be found in approximately one-third to one-half of suicides in persons over 60 years old.1 In this study, persons with somatic disease were significantly older than the physically healthy group, with a mean age of 34.15±16.07 and 25.26±10.11, respectively (p<0.001). The percentage of physically ill persons was lower than what was reported in another study from Iran,2 but almost similar to a hospital based study from India.39
Any lifetime psychiatric disorder is believed to be a strong risk factor for SA.12,24,28,44 In this study, 28.0% of all persons attempting suicide reported previous mental illnesses such as major depression (mild 3%; moderate 4%; severe 10%), schizophrenia (5%), personality disorder (3%), and substance disorders (3%), was lower than the 33.6% of cases in other study from Iran.2
Substance abuse is associated with greater frequency of SAs,1 especially in young adults.12 Similar to a report from India,6 substance abuse was significantly higher in men than women in this study (Table 1), which resembles the same pattern in the Iranian general population. Due to the prohibition of alcohol in Iran and strict laws in the country calling for imprisonment for violations, the patients were not asked in this regard during study interviews.
Like other studies,35 winter had the lowest rate of SA. Furthermore, in this study suicide rates were lower among women than men in winter (Table 1), maybe because of less accessibility to pesticides and poisons, which are the most common causes of suicide, especially among women (Table 3). Moreover, winter is the occasion that farmers and laborers do not work and spend more time with their families; as a result women have more time to seek help and participate in healing activities.
In view of the methods of SA; generally women tend to use less aggressive methods of suicide than men,35 and in this study similar to a study in Belgium,27 hanging and cutting were more common in men, in contrast to the report from Ilam, with 14.9% self immolations in women.4 Self-immolation consisted of 0.6% of all SAs and it was the most lethal way of suicide in the current study, (Table 3). It is estimated that poisons are directly or indirectly responsible for more than one million illnesses worldwide each year.45 One of the oldest methods of SA,45 poisoning in countries with larger rural populations, such as China, India and the Republic of Korea, is common.10 The same result was found in the current study and the other studies.4,17,21,27,35,37,46,47 This may be due to the easy access of medications and poisons in the community. In a study from Tehran, poisoning was reported as the most common (79%) means of suicide.45
Conclusion
Developing countries often underreport suicides as a result of inefficient civil registration and reporting systems, and a tendency to conceal the cause of casualties by family and friends, due to the shame, lack of frankness, social stigma, religious sanctions, and legal issues associated with suicide.3,13,14,19,22,31,48 As such, actual suicide rates are considerably higher than recorded.13,19 In many countries where the majority of the population practice Islam, suicide is still believed to be a criminal offence or taboo; therefore, there is relatively little suicide research available,13 with reliable study methods.48 However, social factors in developing countries play a more prominent role than studies in Europe and North America.6
The findings of this study along with other studies in Iran have revealed that SA was more frequent in single men and women, with lower levels of education, from urban districts in employed men with substance abuse problems and housewives.2,3 In both genders, there is a seasonal variance in suicide attempts. More than 5% of persons attempting suicide have a history of previous suicide attempts. About one quarter have a mental disorder, but 10% have a somatic disorder. More frequently, women who are under the age of 35 and men over the age of 35 tend to commit SA by self-poisoning.
Based on a community survey in central Iran, 66% of females have engaged in suicidal thoughts at some point during their lives.14 Understanding risk factors of suicide and suicidal behaviors provides a way to prioritize preventive efforts and try to wisely invest limited resources.1 Some preventive actions including reducing psychiatric and substance abuse morbidity through identification and appropriate treatment of mental and substance use disorders; limiting access to the most commonly used mechanisms of death,49 including medications.1
It should be considered that it is impossible to determine accurate rates of SA in this study, since SA data were based mainly on hospital admission samples, omitting those who visited general practitioners or who did not seek any medical assistance, which is estimated to be between 50% and 80% of all SAs.5 As a result it could be concluded that the exact rates of SAs are much higher than those presented in this study. Using some more standard approach and scales such as SIS (Suicide Intent Scale) could have strengthened including the results of this study including reports from general practitioners.
Acknowledgements
This study was funded by the Hamadan University of Medical Sciences, contract number 3587492. The authors wish to thank all the staff in hospitals that assisted us in this study, and express special gratitude to Dr. Sahba Eftekhary and Mr. George Kletas for editing the text and their invaluable comments. The authors declare that they have no conflict of interest.
References
1. Moscicki EK. Epidemiology of completed and attempted suicide: toward a framework for prevention. Clin Neurosci Res 2001;1(5):310-323 .
2. Nojomi M, Malakouti SK, Bolhari J, Hakimshooshtari M, Fleischmann A, Bertolote JM. Epidemiology of suicide attempters resorting to emergency departments in Karaj, Iran, 2003. Eur J Emerg Med 2008 Aug;15(4):221-223.
3. Lari AR, Joghataei MT, Adli YR, Zadeh YA, Alaghehbandan RM. Epidemiology of suicide by burns in the province of Isfahan, Iran. J Burn Care Res 2007 Mar-Apr;28(2):307-311.
4. Janghorbani M, Sharifirad G. Completed and attempted suicide in Ilam, Iran (1995-2002): Incidence and assocoiated factors. Arch Iran Med 2005;8(2):119-126.
5. Cantor C, Neulinger K. The epidemiology of suicide and attempted suicide among young Australians. Aust N Z J Psychiatry 2000 Jun;34(3):370-387.
6. Parkar SR, Dawani V, Weiss MG. Gender, suicide, and the sociocultural context of deliberate self-harm in an urban general hospital in Mumbai, India. Cult Med Psychiatry 2008 Dec;32(4):492-515.
7. Mofidi N, Ghazinour M, Salander-Renberg E, Richter J. Attitudes towards suicide among Kurdish people in Iran. Soc Psychiatry Psychiatr Epidemiol 2008 Apr;43(4):291-298.
8. WHO. Suicide rates per 100,000 by country, year and sex 2010 [updated 2010; cited]; Available from: http://www.who.int/mental_health/prevention/suicide_rates/en/.
9. Khazaei H, Parvizi Fard A. Demographic characteristics and mental state evaluation of attempted suicide victims in Tabriz. Behbood. 2003;18:42-51.
10. Hendin H, Phillips MR, Vijayakumar L, Pirkis J, Wang H, Yip P, et al. Suicide and Suicide Prevention in Asia. Geneva: World Health Organization; 2008.
11. Straus MA, Kantor GK. Corporal punishment of adolescents by parents: a risk factor in the epidemiology of depression, suicide, alcohol abuse, child abuse, and wife beating. Adolescence. 1994 1994 Fall;29(115):543-61.
12. Scocco P, de Girolamo G, Vilagut G, Alonso J. Prevalence of suicide ideation, plans, and attempts and related risk factors in Italy:: Results from the European Study on the Epidemiology of Mental Disorders-World Mental Health study. Comprehensive Psychiatry. 2008 2008/2//;49(1):13-21.
13. Pritchard C, Amanullah S. An analysis of suicide and undetermined deaths in 17 predominantly Islamic countries contrasted with the UK. Psychol Med 2007 Mar;37(3):421-430.
14. Malakouti SK, Nojomi M, Bolhari J, Hakimshooshtari M, Poshtmashhadi M, De Leo D. Prevalence of suicide thoughts, plans and attempts in a community sample from Karaj, Iran. Community Ment Health J 2009 Feb;45(1):37-41.
15. Large MM, Nielssen OB, Lackersteen SM. Did the introduction of ‘dangerousness’ and ‘risk of harm’ criteria in mental health laws increase the incidence of suicide in the United States of America? Soc Psychiatry Psychiatr Epidemiol 2009 Aug;44(8):614-621.
16. Webster Rudmin F, Ferrada-Noli M, Skolbekken J-A. Questions of culture, age and gender in the epidemiology of suicide. Scand J Psychol 2003 Sep;44(4):373-381.
17. Kim M-H, Jung-Choi K, Jun H-J, Kawachi I. Socioeconomic inequalities in suicidal ideation, parasuicides, and completed suicides in South Korea. Soc Sci Med 2010 Apr;70(8):1254-1261.
18. Rezaeian M. Suicide/homicide ratios in countries of the Eastern Mediterranean Region. East Mediterr Health J 2008 Nov-Dec;14(6):1459-1465.
19. Ahmadi A, Ytterstad B. Prevention of self-immolation by community-based intervention. Burns 2007 Dec;33(8):1032-1040.
20. Sharifi V, Rahimi-Movaghar A, Mohammadi MR, Goodarzi RR, Izadian ES, Farhoudian A, et al. Analysis of mental health research in the Islamic Republic of Iran over 3 decades: a scientometric study. East Mediterr Health J 2008 Sep-Oct;14(5):1060-1069.
21. Mohammadi g, Saadati a. Epidemiology and etiology of attempted suicides and their relation with demographic data among patients referred to emergency department in Neyshabur. The Quarterly Journal of Fundamentals of Mental Health. 2004;6(23):117-125.
22. Christl B, Wittchen H-U, Pfister H, Lieb R, Bronisch T. The accuracy of prevalence estimations for suicide attempts. how reliably do adolescents and young adults report their suicide attempts? Arch Suicide Res 2006;10(3):253-263.
23. Moradi S, Khademi A. Evaluation of suicides resulting in death in Iran, comparing with the World rates. Law Medicine Journal. 2002;8(27):16-21.
24. Christoffersen MN, Poulsen HD, Nielsen A. Attempted suicide among young people: risk factors in a prospective register based study of Danish children born in 1966. Acta Psychiatr Scand 2003 Nov;108(5):350-358.
25. Iran SCo. National population and housing census (NPHC) Tehran: (SCI); 2006 [updated 2006; cited]; Available from: http://www.sci.org.ir/portal/faces/public/census85/census85.natayej.
26. Ahmadi A. Suicide by self-immolation: comprehensive overview, experiences and suggestions. J Burn Care Res 2007 Jan-Feb;28(1):30-41.
27. Bossuyt N, Van Casteren V. Epidemiology of suicide and suicide attempts in Belgium: results from the sentinel network of general practitioners. Int J Public Health 2007;52(3):153-157.
28. Borges G, Nock MK, Medina-Mora ME, Benjet C, Lara C, Chiu WT, et al. The epidemiology of suicide-related outcomes in Mexico. Suicide Life Threat Behav 2007 Dec;37(6):627-640.
29. Mohammadi AA, Danesh N, Sabet B, Amini M, Jalaeian H. Self-inflicted burn injuries in southwest Iran. J Burn Care Res 2008 Sep-Oct;29(5):778-783.
30. Holley HL, Fick G, Love EJ. Suicide following an inpatient hospitalization for a suicide attempt: a Canadian follow-up study. Soc Psychiatry Psychiatr Epidemiol 1998 Nov;33(11):543-551.
31. Alem A, Kebede D, Jacobsson L, Kullgren G. Suicide attempts among adults in Butajira, Ethiopia. Acta Psychiatr Scand Suppl 1999;397:70-76.
32. Rey Gex C, Narring F, Ferron C, Michaud PA. Suicide attempts among adolescents in Switzerland: prevalence, associated factors and comorbidity. Acta Psychiatr Scand 1998 Jul;98(1):28-33.
33. Roberts RE, Roberts CR, Xing Y. One-year incidence of suicide attempts and associated risk and protective factors among adolescents. Arch Suicide Res 2010;14(1):66-78.
34. Nojomi M, Malakouti SK, Bolhari J, Poshtmashhadi M. A predictor model for suicide attempt: evidence from a population-based study. Arch Iran Med 2007 Oct;10(4):452-458.
35. Sheikholeslami H, Kani C, Ziaee A. Attempted suicide among Iranian population. Suicide Life Threat Behav 2008 Aug;38(4):456-466.
36. Ahmadi A, Mohammadi R, Stavrinos D, Almasi A, Schwebel DC. Self-immolation in Iran. J Burn Care Res 2008 May-Jun;29(3):451-460.
37. Rabani a. frequency of suicide attempts among patients referred to hospitals and clinics in Hamadan. Hamadan: Hamadan University of Medical Sciences; 2002.
38. Heidari p a, Maleki h. social and mental variables influencing 1029 suicide attempts in patients referred to educational treatment centers in Hamadan. Scientific journal of Hamadan University of MedicalL Sciences & Health Services. 1999;6(4):56-61.
39. Latha KS, Bhat SM, D’Souza P. Suicide attempters in a general hospital unit in India: their socio-demographic and clinical profile–emphasis on cross-cultural aspects. Acta Psychiatr Scand 1996 Jul;94(1):26-30.
40. Ratnayake R, Links PS, Eynan R. Suicidal behaviour on subway systems: a review of the epidemiology. J Urban Health 2007 Nov;84(6):766-781.
41. Mohammadi AA, Danesh N, Sabet B, Amini M, Jalaeian H. Self-inflicted burn injuries in southwest Iran. J Burn Care Res 2008 Sep-Oct;29(5):778-783.
42. Poshtmashhadi M, Molavi Nojomi M, Malakout S, Bolhar J, Asgharzadeh AS, Asgharnejad FA. Suicide attempt and its relation to stressors and support system: a study in Karaj City Tehran University Medical Journal. 2007;65(4):72-6.
43. Taylor A, Dal Grande E, Gill T, Fisher L, Goldney R. Detecting determinants of suicidal ideation: South Australian surveillance system results. Int J Public Health 2007;52(3):142-152.
44. Suominen K, Henriksson M, Suokas J, Isometsä E, Ostamo A, Lönnqvist J. Mental disorders and comorbidity in attempted suicide. Acta Psychiatr Scand 1996 Oct;94(4):234-240.
45. Shadnia S, Esmaily H, Sasanian G, Pajoumand A, Hassanian-Moghaddam H, Abdollahi M. Pattern of acute poisoning in Tehran-Iran in 2003. Human and Experimental Toxicology. 2007 September 1, 2007;26(9):753-6.
46. Abeyasinghe R, Gunnell D. Psychological autopsy study of suicide in three rural and semi-rural districts of Sri Lanka. Soc Psychiatry Psychiatr Epidemiol 2008 Apr;43(4):280-285.
47. Thombs BD, Bresnick MG, Magyar-Russell G. Who attempts suicide by burning? An analysis of age patterns of mortality by self-inflicted burning in the United States. General Hospital Psychiatry. 2007 2007/6//;29(3):244-50.
48. Khan MM, Hyder AA. Suicides in the developing world: case study from Pakistan. Suicide Life Threat Behav 2006 Feb;36(1):76-81.
49. Wright MA, Wintemute GJ, Claire BE. Gun suicide by young people in California: descriptive epidemiology and gun ownership. J Adolesc Health 2008 Dec;43(6):619-622.
|
|