A 15-year-old female was referred to King Faisal Specialist Hospital and Research Centre with a history of lower abdominal discomfort and abdominopelvic mass. She was referred to us with the diagnosis of hematocolpos with uterus didelphys and an imperforate hymen. The patient was diagnosed with an absent right kidney since childhood. However, she had no history of urinary complaints. The patient admitted that she had not started menses. Physical examination of the external genitalia showed no abnormalities. Routine evaluation include laboratory findings were unremarkable.
Transabdominal sonography demonstrated an absent right kidney. The left kidney was normal. Pelvic ultrasound revealed two uterine cavities; right and left [Figure 1]. The right uterus was larger than the left; however, both showed normal, regular endometrial thickness. There was a distended structure to the right side behind the urinary bladder, which measured 4.6 × 6.4 × 10.8 cm and contained echogenic material in keeping with a distended right vagina. Both ovaries were normal.
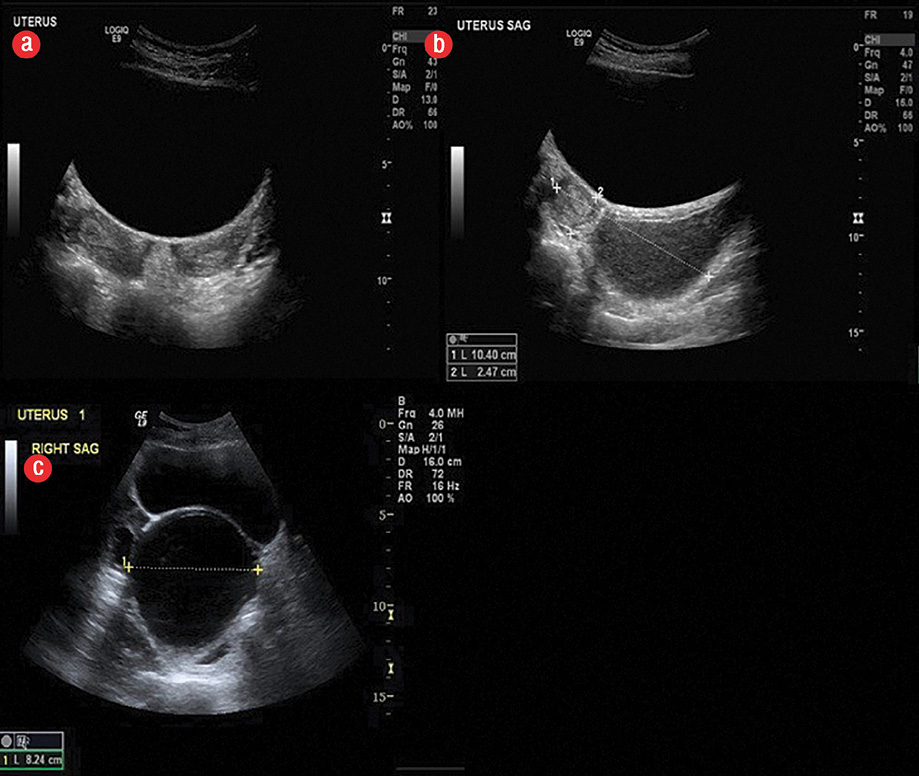
Figure 1: Transabdominal ultrasound of the patient revealed (a, b) two uterine cavities and a (c) distended obstructed structure to the right side just behind the urinary bladder containing echogenic material in keeping with distended right vagina.
Magnetic resonance imaging (MRI) of the pelvis was done and revealed two separated uteri and vagina consistent with uterus didelphys. However, the right vagina was obstructed inferiorly and was hugely distended with blood consistent with hematocolpos. It measured 12 × 7 × 7 cm. The right uterine cavity was also filled with blood; however, it was only mildly distended and had a diameter of 1.2 cm. The left uterine cavity had normal endometrial thickness. The left cervix and vagina were stretched along the left wall of the right hematocolpos. The distal vagina crossed anteriorly where it had a patent opening. The right kidney was absent and the left kidney was normal in appearance. These findings were consistent with the diagnosis of obstructed hemivagina and ipsilateral renal anomaly (OHVIRA) syndrome.
The details of the patient’s condition were discussed with the patient and her parents, including the complications of outflow obstruction to the right vagina which can lead to hematocolpos, hematometra, hematosalpinx, and later may cause a retrograde bleeding, chronic pelvic pain, endometriosis, and infertility. Vaginoscopy and laparoscopy with vaginal septal resection were recommended.
Discussion
The overall prevalence of congenital anomalies of the Müllerian tract is around 2% to 3% among women.1 OHVIRA syndrome, previously known as Herlyn-Werner-Wunderlich syndrome, was first reported in 1922. It classically occurs in the setting of uterine didelphys or, rarely, a septate uterus.1,2 The most common renal anomaly associated with this syndrome is renal agenesis. Other malformations, including multicystic dysplastic kidney and renal duplication, have also been reported.2
The pathogenesis of OHVIRA syndrome is unclear but is thought to be multifactorial. Uterine didelphys happens due to fusion failure of the Müllerian ducts. Early high-level obstruction of the pelviureteric junction leading to agenesis of the ipsilateral kidney, often results in defects in the Müllerian duct at the same level. Because of the close relationship between the development of urinary and reproductive systems, female patients with renal malformations may benefit from evaluation later in life for reproductive structural anomalies and vice versa.3
The usual presentation of such cases is nonspecific symptoms of repeated abdominal pain or dysmenorrhea from progressive distention of the obstructed hemivagina after the age of menarche.
Early and accurate diagnosis and further therapeutic intervention should be made to relieve patient’s symptoms and prevent complication of chronic obstructed hematocolpos (e.g., pelvic adhesions and endometriosis) and will support the reproductive capacity.3
In a reported series of 27 cases, the median age at diagnosis was 14 years. Patients were diagnosed between the ages of 10 to 29 years.2 Any delay in diagnosis was due to the lack of knowledge of the disease normal regular menstruations due to incomplete vaginal outlet obstruction in addition to slow progression of the hematocolpos.4
Ultrasound is frequently the initial imaging modality to evaluate suspected Müllerian duct anomalies. This is due to its wide availability and relatively low cost. However, ultrasound is operator dependent and can be missed by inexperienced operators. MRI, however, is an excellent examination of choice for evaluating complex Müllerian duct anomalies. This is due to its multiplanar capability, large field of view, and superior tissue characterization. MRI can accurately depict the shape of the uterine cavity, the uterine contour, and associated cervical and vaginal anomalies. It is also important in the classification of Müllerian duct anomalies and surgical planning.5 MRI can allow tissue characterization of the septa,6 characterize the contents of obstructed cavities (e.g., blood versus simple fluid), and can easily detect any coexisting renal and/or urethral abnormalities.
Primary treatment of OHVIRA syndrome is vaginoplasty to relieve the obstruction. Historically, surgeons advocated a two-stage procedure. Initial surgery aimed to decrease the hematocolpos and the second to reset the excess septum after a period of wound-healing and vaginal remodeling. However, single-stage vaginoplasty, which includes complete resection of the septum in a single procedure, is encouraged in the contemporary literature.2 It is important to recognize that the apparently absent kidney on MRI does not entirely exclude the possible presence of a small and/or atrophic kidney.
Identification of a dysplastic kidney can be very challenging radiologically. Other diagnostic modalities that may be of help include Technetium-99m-dimercaptosuccinic acid (DMSA) renal scan, intravenous urography, and contrast vaginography.7,8 Clinically, chronic purulent vaginal discharge can be the presenting symptom of ectopic vaginal ureter associated with a dysplastic kidney.9 Management is either through transvaginal ligation of the ureter or by laparoscopic transperitoneal nephrectomy. Unfortunately, there are few reported malignant transformation of ectopic vaginal cases in the literature.10,11
Conclusion
Physicians including gynecologists, pediatricians, radiologists, and pediatric surgeons should consider OHVIRA syndrome among the differential diagnosis in young female patients presenting with a pelvic mass. Because there is a very close association between the development of urinary and genital systems, it is always worth checking for renal abnormalities in patients with Müllerian anomalies, and vice versa. Though OHVIRA syndrome is rare, early detection and management is important to avoid future associated complications and maintain normal reproductive capacity.
Disclosure
The authors declared no conflicts of interest.
references
- 1. Shavell VI, Montgomery SE, Johnson SC, Diamond MP, Berman JM. Complete septate uterus, obstructed hemivagina, and ipsilateral renal anomaly: pregnancy course complicated by a rare urogenital anomaly. Arch Gynecol Obstet 2009 Sep;280(3):449-452.
- 2. Smith NA, Laufer MR. Obstructed hemivagina and ipsilateral renal anomaly (OHVIRA) syndrome: management and follow-up. Fertil Steril 2007 Apr;87(4):918-922.
- 3. Orazi C, Lucchetti MC, Schingo PM, Marchetti P, Ferro F. Herlyn-Werner-Wunderlich syndrome: uterus didelphys, blind hemivagina and ipsilateral renal agenesis. Sonographic and MR findings in 11 cases. Pediatr Radiol 2007 Jul;37(7):657-665.
- 4. Zurawin RK, Dietrich JE, Heard MJ, Edwards CL. Didelphic uterus and obstructed hemivagina with renal agenesis: case report and review of the literature. J Pediatr Adolesc Gynecol 2004 Apr;17(2):137-141.
- 5. Tanaka YO, Kurosaki Y, Kobayashi T, Eguchi N, Mori K, Satoh Y, et al. Uterus didelphys associated with obstructed hemivagina and ipsilateral renal agenesis: MR findings in seven cases. Abdom Imaging 1998 Jul-Aug;23(4):437-441.
- 6. Carrington BM, Hricak H, Nuruddin RN, Secaf E, Laros RK Jr, Hill EC. Müllerian duct anomalies: MR imaging evaluation. Radiology 1990 Sep;176(3):715-720.
- 7. Son T, Thang C, Hung T, Tram NT. Single ectopic ureter: diagnostic value of contrast vaginography. Urology 2009 Aug;74(2):314-317.
- 8. Yu HT, Chao A, Wang CJ, Chao AS, Lai CY, Wang CR, et al. Integrated imaging studies and endoscopic management of purulent vaginal discharge in a 6-year-old: vaginal ectopic ureter associated with ipsilateral dysplastic kidney. Eur J Obstet Gynecol Reprod Biol 2009 Feb;142(2):160-161.
- 9. Jain KA. Ectopic vaginal insertion of an obstructed duplicated ureter in an adult female: demonstration by magnetic resonance imaging. Clin Imaging 2007 Jan-Feb;31(1):54-56.
- 10. Jaidane M, Slama A, Bibi M. A tumor of an ectopic ureter mimicking uterine cervix adenocarcinoma: case report and brief review. Int Urogynecol J Pelvic Floor Dysfunct 2009 Nov;20(11):1393-1395.
- 11. Sameshima H, Nagai K, Ikenoue T. Single vaginal ectopic ureter of fetal metanephric duct origin, ipsilateral kidney agenesis, and ipsilateral rudimentary uterine horn of the bicornuate uterus. Gynecol Oncol 2005 Apr;97(1):276-278.