
Belief in Charity Giving (Sadqa) and its Role in Healing: Results of a Survey Conducted at a Teaching Hospital in Karachi, Pakistan
Waris Qidwai,1 Rumina Tabassum,2 Raheela Hanif,3 Fahad H. Khan3
Qidwai W, et al. OMJ. 25, 108-113 (2010); doi:10.5001/omj.2010.30
ABSTRACT
Objectives: To study patients’ belief and practice about Sadqa (charity) and its role in recovery from illness and restoration of health. This study will determine whether such belief and practice is related to any demographic factors such as sex, education, and religious sects.
Methods: A questionnaire was designed that included the demographic profile of patients and questions in accordance to the study objective. It was administered to 400 patients or their attendants against the calculated sample size of 385. There were very few refusals to participate with response rate of around 98%. The study objective was explained to all participants, written consent was obtained and full confidentiality was assured.
Results: The mean age of the study population was 34.33 years, majority of the patients were males with 65.6% having grade XII or higher education. The practice of giving sadqa/charity for healing was significantly associated with females (p<0.001); Ismaili sect (p=0.017); educational level of grade V (p=0.03); graduate (p=0.041); being housewives (p<0.001), students (p=0.048) and employees in private services (p<0.001). Approximately 85% of the study population gave sadqa/charity for healing diseases and 84.8% believed that sadqa/charity heals diseases. According to 97.5% of the participants, medical treatment should be combined along with sadqa/charity for healing.
Conclusion: This study highlights the importance of the patients’ attachment to charity giving and expectation that it will lead to recovery from illness. Future research in this area should be qualitative rather than quantitative to explore more about beliefs, attitude and behavior of the individuals. It is recommended that health care professionals should consider and also respect patients’ and relatives beliefs about sadqa and charity; clashing with their beliefs during provision of medial care should be avoided.
From the 1Department of Family Medicine, Aga Khan University, Karachi, 2Department of Gynaecology & Obstetrics, Dow University of Health Sciences, 3Medical student, Dow University of Health Sciences, Pakistan.
Received: 13 Dec 2009
Accepted: 11 Feb 2010
Address correspondence and reprint request to: Dr. Waris Qidwai, Department of Family Medicine, Aga Khan University, Stadium Road, P.O. Box: 3500, Karachi 74800, Pakistan.
E-mail: waris.qidwai@aku.edu
Qidwai W, et al. OMJ. 25, 108-113 (2010); doi:10.5001/omj.2010.30
INTRODUCTION
Charity is defined as giving to those in need, or love of one’s fellow men.1 Charity both obligatory almsgiving and voluntary donations, was and is an established practice for Muslims throughout the world.2 Sadqa is charity giving but unlike charity, it is given to get blessings of the creator to have favorable outcome in different areas such as improvement in health or averting a disaster. It is a common observation that Sadqa is given to promote healing and recovery from diseases and illness in Pakistani society. It has been observed that when a person is sick, his or relatives will give charity in the hope that healing and recovery will take place.
A study reveals South African Muslim and Hindu traditional healers advised people to give to charity during illness.3 Healing in a patient takes place through a process that draws upon powers of nature, science and physician and it is these forces that are assumed to be favorably affected by giving of sadqa or charity.4 Bargaining is an important step in accepting a serious illness and includes giving charity and praying.5
The faith in healing resulting from charity is not confined to the developing countries but is also documented in the developed world.6, 7
This is an age that advocates a holistic model of patient care that includes biological, psychological, social and spiritual aspects.8 It is for this reason that modern day clinicians should enquire charity giving by patients and their relatives in the hope of healing and recovering from an illness.
Terminal care patients and patients with chronic illnesses have no option other than palliative care offered by modern medicine to reduce their suffering and improve quality of life.9,10 Giving charity in the hope of recovery from illness in such situation can have positive impact on patient over all well being.
Given this background, there is need to determine patients’ belief and practice of Sadqa (charity) and whether such belief and practice is related to any demographic factors associated factors such as sex, education, and religious sect.
A questionnaire based cross-sectional survey was conducted at the Community Health
Centre of Aga Khan University Hospital, Karachi, Pakistan in June 2008. On an
average, 200 family practice patients with mostly primary and secondary care
level problems were seen daily by 12-16 family physicians at the centre.
A questionnaire was developed by the investigators after extensive literature
search, including input from colleagues and patients.2-7 The
questionnaire included the demographic profile of patients including age, sex,
marital status, education, occupation, ethnic group and religious sect.
Questions were developed at exploring patients’ perceptions regarding the
healing effects of sadqa/charity and prayers, the way the patients preferred
such practice and its role in combination with modern medicine.
The questionnaire was developed in English language and translated into local Urdu language and translated back to English to confirm consistency in the meaning of questions. It was administered in both English and Urdu languages, depending upon patient’s comfort. It was administered by study investigators and a meeting was arranged prior to its administration to ensure consistency in data collection by different interviewers. The investigators interviewed the patients and filled out the questionnaire. A pilot study was conducted prior to the initiation of the administration of the final questionnaire.
An agreement was reached between the investigators on how to administer the questionnaire, in order to ensure the uniformity in filling of the questionnaire. The questionnaire was administered in the waiting area outside the physician’s office prior to the consultation.
Patients who agreed to participate in the study regardless of family physician they consulted were interviewed. The interviews were conducted throughout the month no specific timings were followed. The calculated sample size was 385.
Ethical requirement including the administration of written informed consent and the provision of confidentiality were ensured.
Participants were interviewed based on their availability and convenience. A systematic random selection of study subjects was not undertaken. Epi info version 3.0 & SPSS version 16.0 were used for data entry and management respectively. Since no prior data was available on this topic, a sample size of 400 was used. “P” values were calculated to determine statistical significance of beliefs and practices across various demographic variables.
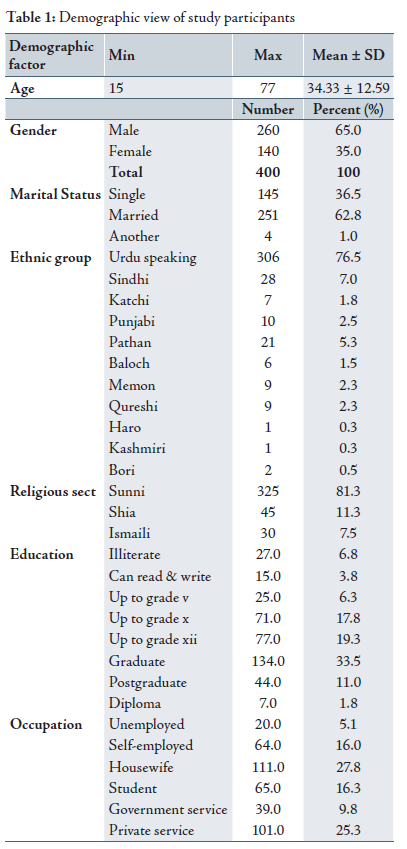
RESULTSA total of 400 participants were interviewed. There were very few refusals to participate with a response rate of approximately 98%. Patients were interviewed based on convenience sampling. The mean age of the studied population was 34.3 years, majority of the subjects were married (62.8%), and the female to male ratio was 1:1.85 with 65.6% having grade XII education or higher. The majority of respondents were housewives (27.8%), followed by those in private service (25.3%), students (16.3%) and self-employed (16%). Also, a majority of respondents were Urdu speaking (76.5%) and 81.3% belonged to Sunni sect. (Table 1)
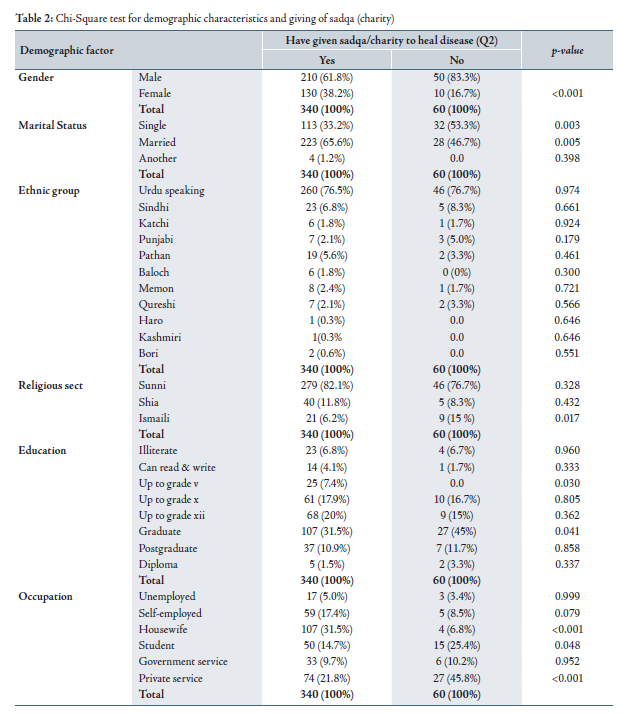
The practice of giving sadqa/charity for healing was significantly associated with females (p<0.001); marital status; Ismaili sect (p=0.017); educational level of grade V (p=0.03); graduates (p=0.041); housewives (p<0.001), students (p=0.048) and employees in private services (p<0.001). (Table 2)
The scatter diagram shows that people above the age of 30 are more in favor of this practice. (Fig. 1)
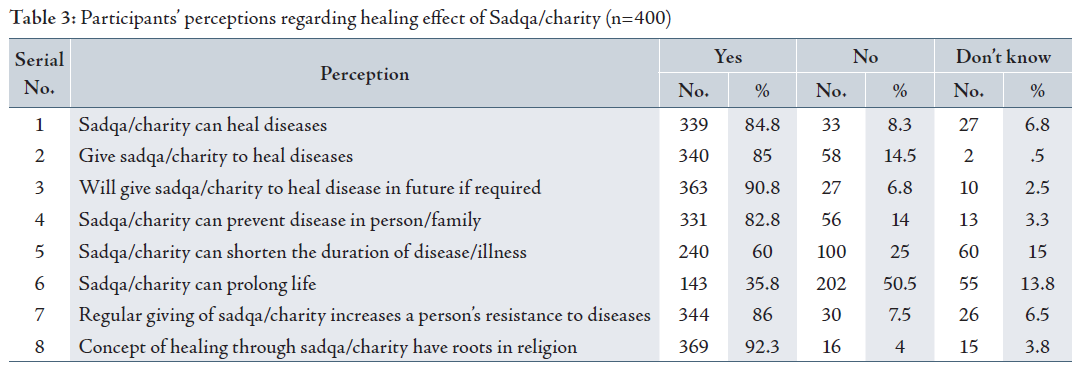
Sadqa/charity can heal diseases is a common belief in 84.8% of the respondents and 85% of respondents give sadqa/charity for healing. According to 92.3% of participants concept of healing by giving sadqa/charity giving is a religious belief. (Table 3)
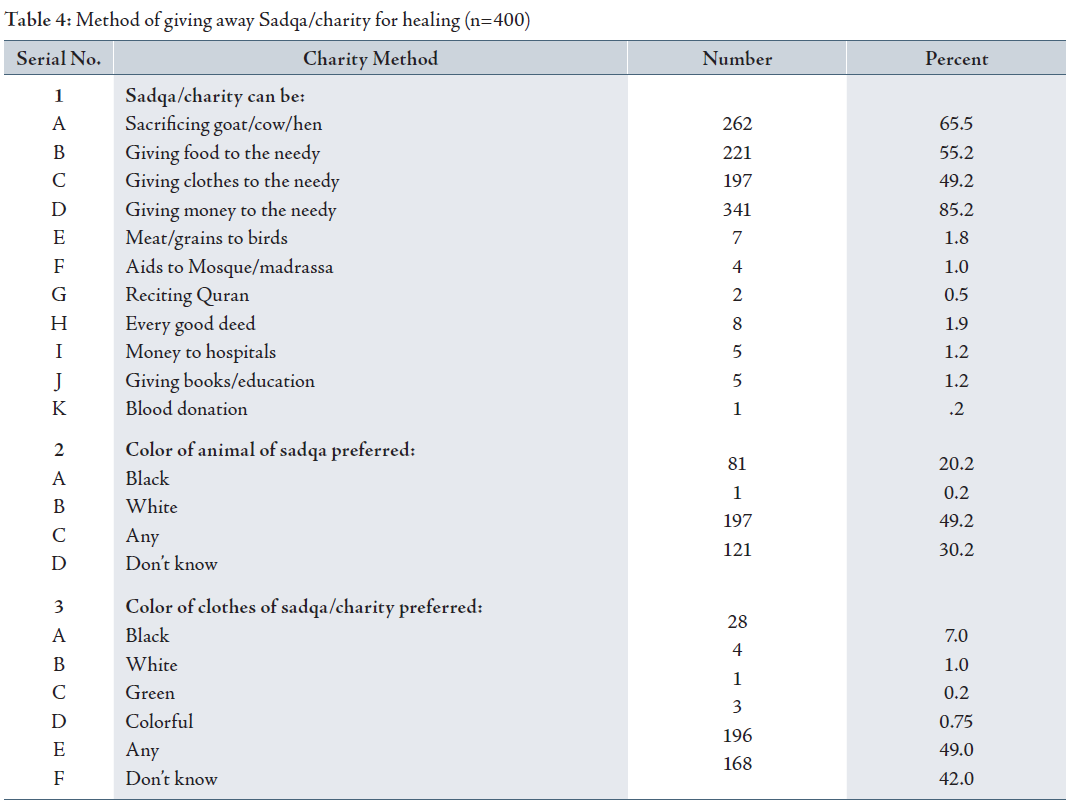
Sadqa/charity is usually given in the form of money (85.2%), food (55.2%), clothes (49.2%) and sacrificing an animal (65.5%) with most of the respondents having no color preferences for clothes (49%) or the sacrificial animal (49.2%). (Table 4)
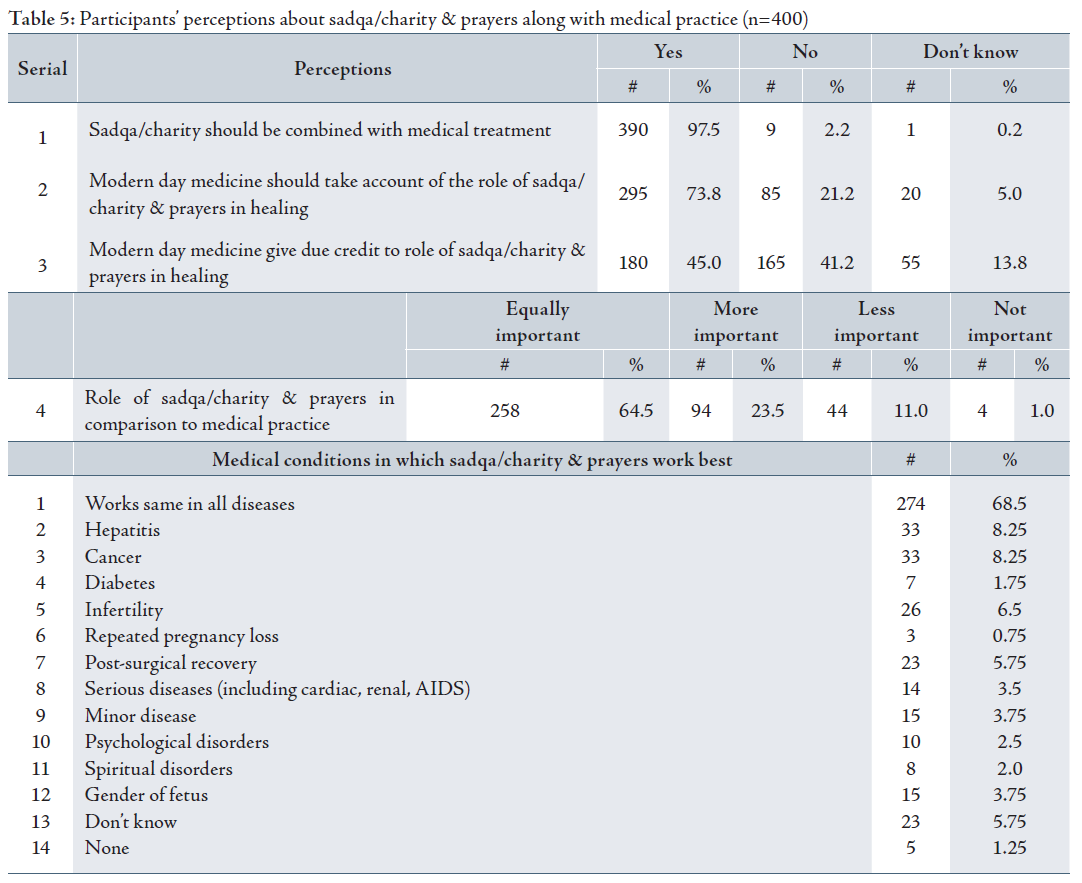
“Medical treatment should accompany sadqa/charity for healing” this was a common belief among 97.5% of the respondents. While 73.8% believed that medicine should take account of prayers as a healing method. For 64.5% of the respondents, prayers and medicine are equally important. Table 5 lists the diseases and conditions in which respondents consider charity giving to be mostly effective.
DISCUSSION
This is among the first studies which highlights the important topic of giving of
sadqa and charity by patients and relatives in the hope of recovering from
illness and disease in Pakistan. The study sample was large enough and with a
very high response rate to draw valid conclusions. The study population
represented all groups and strata of the society. One can argue that the study
population was hospital based and those who are sicker and more health conscious
visit hospital, limiting the results as opposed to generalizing them to the
population at large. This is a limitation of this study and a community based
survey is recommended. The study population was a relatively well-educated and
affluent population at a University medical center and affects the
generalizability of the results. The lack of studies on this topic prevents
direct comparisons to be drawn from any available data. There is indirect
evidence that patient’s faith is considered important by the patient in the
healing process.11,12
This study has documented a very strong preference and practice in favor of giving
Sadqa/charity in the hope of recovery from illness, among the studied
respondents. It is important for clinicians to note that almost 85% of the
respondents believed in this practice and give charity. It is again important to
note that almost 92% relate the belief and practice of Sadqa and charity giving
in the hope of recovery from illness to religion. These are important findings
and can have a favorable impact on patient-physician consultation if handed in a
supportive manner by the clinician.
The finding that patients believe charity giving not only improves healing but also
shortens disease duration, increases patient’s resistance and prevents it from
recurring in the future has important implications for clinical practice. They
also believed that it prolongs life. The depth of belief in charity giving for
healing and improving health shows the extent to which patients have firm
beliefs in this practice. Clinicians ignoring this aspect in patient care are
missing a very important aspect of medical care from patient’s point of view.
It will be considered a deviation from a patient centered model of medical care and
thus not in line with current day medical practice.
The form in which charity or sadqa is given is also important to note. It is not
restricted to giving money, but also includes giving food, clothes or
sacrificing animals. This shows the value that people attach to this practice
and use whatever means is available to them. There was no preference of color of
the animal to be sacrificed for Sadqa to have maximum impact. The fact that
color of cloth or animal was not considered statistically important among the
respondents shows that superstition had little place in their minds and
practice. It is important for modern medical practitioners to promote patient
beliefs in health seeking behavior that is based on scientific lines and is
evidence based.
This study demonstrates that the practice of giving sadqa and charity in the hope
of recovery from disease is significantly associated with certain factors such
as gender, marital status, Ismaili sect, educational level, and certain
occupations such as private services, being a housewife and student status.
Increasing age is also associated with the practice of sadqa and charity. It is
important to identify factors associated with this practice among patients so
that a better management plan can be made and clinicians can harness advantage
of seeking well being among their patients as a result of this practice.
This study highlights the fact that a majority of the patients consider practice of charity giving and medical treatment equally important in recovery from illness and want modern day medical practitioners to incorporate consideration of sadqa and charity by patients and their relatives while providing medical care. Such patient expectations are in line with holistic models of medical care, as well as patient centered approach advocated by the medical profession today. Patient centered approach is considered an important part of present day medical practice.13 It is important for practitioners to consider Patient’s beliefs as important and not to make the patient feel that their beliefs are being disregarded
CONCLUSION
Charity giving (Sadqa) in the hope of recovery from illness was widespread among the studied patients. The modern day medical practitioners must give consideration to sadqa and charity by patients and relatives to influence recovery from illness and disease. Further research in this important area of health care is recommended.
The authors reported no conflict of interest and no funding has been received on this work.
Catherine Walker. A charitable view of altruism: Commentary on ‘What is altruism?’ by Elias Khalil. Journal of Economic Psychology 2004; 25(1):129-134.
Singer A. Soup and sadaqa: Charity in Islamic societies. Historical Research 2006; 79(205):306-324.
-
Ross E. A tale of two systems: beliefs and practices of South African Muslim and Hindu traditional healers regarding cleft lip and palate. Cleft Palate Craniofac J 2007; 44(6):642-648.
-
Szawarski Z. Wisdom and the art of healing. Med Health Care Philos 2004; 7(2):185-193.
-
VandeKieft GK. Breaking bad news. Am Fam Physician 2001; 64(12):1975-1978.
-
Szini K. Healing with wisdom and charity (in memory of Katalin Fugulj?n). Orv Hetil 1985; 126(22):1360-1362.
-
Long A, Baxter R. Functionalism and holism: community nurses’ perceptions of health. J Clin Nurs 2001(3); 10:320-329.
-
Hariprasad G. Holistic presentation of the undergraduate medical curriculum. Med Educ 2008; 42(8):849.
-
Borreani C, Miccinesi G. End of life care preferences. Curr Opin Support Palliat Care 2008; 2(9):54-59.
-
Gallagher R, Donoghue J, Chenoweth L, Stein-Parbury J. Self-management in older patients with chronic illness. Int J Nurs Pract 2008; 14(5):373-382.
-
Ford D, Zapka J, Gebregziabher M, Yang C, Sterba K. Factors associated with illness perception among critically ill patients and surrogates. Chest. 2010.
-
Cadge W, Ecklund EH. Prayers in the clinic: how pediatric physicians respond. South Med J 2009 Dec; 102(12):1218-1221.
-
Al-Bawardy R, Blatt B, Al-Shohaib S, Simmens SJ. Cross-cultural comparison of the patient-centeredness of the hidden curriculum between a Saudi Arabian and 9 US medical schools. Med Educ Online 2009 Dec; 14:19.