
Faiza Al Aisari, Huda Al-Hashmi, Waad-Allah Mula-Abed
Al Aisari F, et al. OMJ. 25, 9-12 (2010); doi:10.5001/omj.2010.3
ABSTRACT
Objectives: This study aims to assess the usefulness of serum holotranscobalamin (holoTC), the fraction of vitamin B12 that is available for tissue uptake, compared with total vitamin B12 in patients investigated for vitamin B12 disorders
Methods: Serum samples were randomly selected from 76 patients (48 females, 28 males; age range 12-69 years) referred to the Clinical Biochemistry Laboratory, Royal Hospital for the assessment of vitamin B12 status. For each patient, serum total vitamin B12 level was determined by chemiluminescent microparticle immunoassay on Architect 2000 analyzer and holoTC (active vitamin B12) level was determined by microparticle enzyme immunoassay on Axsym analyzer (both from Abbott, USA).
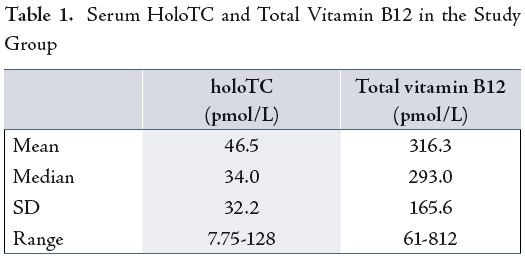
Results: Comparison of the data was conducted to reflect the mean, standard deviation (SD) and correlation coefficient between the two groups. The mean (SD) for serum holoTC and total vitamin B12 were 46.5(32.2) pmol/L and 316.3(165.6) pmol/L respectively. There was a significant correlation between holoTC and total vitamin B12 (r= 0.765, P< 0.001) and the regression equation was expressed as; y = a + bx (i.e: holoTC = 1.5 + 0.14 total vitamin B12). Also, the results were assessed for any misclassification when comparing holoTC and the total vitamin B12 in terms of whether each or both values agree or disagree for classifying the patients as having normal or abnormal (low or high) results, based on the cut-off thresholds of the kit’s quoted reference range for holo TC o f 9 - 1 2 3 pmol/L and for total vitamin B12 of 140-600 pmol/L. Accordingly, in 69 (90.8%) samples, there was a parallel agreement/ classification of results, both being normal or abnormal. In 61 (80.4%) patients, both results were normal, whereas in 4 (5.2%) patients, both results were high, and in 4 (5.2%) patients both results were low. However, in 7 (9.8%) cases, there was disagreement/ misclassification of results; 6 (7.8%) patients, holoTC was normal while total vitamin B12 was low, and in 1 (1.4%) patient, holoTC was normal while total vitamin B12 was high.
Conclusion: It can be recommended that holoTC and total vitamin B12, alone and in combination, have almost equal diagnostic efficiency in screening/diagnosing vitamin B12 deficiency for the majority of patients. In very few patients, holoTC appeared to be a better reflector of vitamin B12 status. Further comparison studies based on a gold standard method for classifying vitamin B12 status are worth considering.
From the Department of Chemical Pathology, Royal Hospital, Muscat, Sultanate of Oman.
Received: 05 Nov 2009
Accepted: 28 Dec 2009
Address of correspondence and reprint requests to: Dr. Waad-Allah Mula-Abed, Directorate of Medical Laboratories, Royal Hospital, Muscat, Oman. E- mail: drsharef@omantel.net.om
INTRODUCTION
Vitamin B12 (cobalamin) is an important metalloenzyme which consists of a porphyrin-like macromolecule with a central cobalt atom that is bound to a nucleotide residue, the whole unit is called cobalamin. It is required as coenzymes for the metabolism of the amino acids methionine, threonine and valine, as well as for the transformation of methyl-tetrahydrofolate to tetrahydrofolate which is necessary for DNA synthesis.1
Cobalamin is bound to two proteins, transcobalamin (TC) and haptocorrin (HC). The TC-vitamin B12 complex is called holotranscobalamin (holoTC) containing the biologically active cobalamin, which promotes the uptake of its cobalamin by all cells, via specific receptors. The much larger fraction (about 80%) of cobalamin carried by HC is considered to be metabolically inert because no cellular receptors exist, except on the liver.2,3 Genetic absence of HC, although rare, is not a serious condition. On the other hand, genetic absence or abnormalities of TC are manifested as typical haematological, neurological and metabolic manifestations of cobalamin deficiency requiring treatment even though serum analysis may show normal cobalamin concentrations.4 The shorter half life for holoTC compared to holoHC makes a decrease in holoTC as one of the earliest markers of cobalamin deficiency.5
Measurement of total vitamin B12 suffers from some limitations, in particular, most of the cobalamin measured is that bound to HC.6,7 A number of studies have been published to support that holoTC would be a better indicator of vitamin B12 status than total vitamin B12.8,9 New methods based on specific anti-TC antibodies are available and confirm the usefulness of holoTC measurement for diagnosing vitamin B12 deficiency.10,11 As expected, holoTC levels are low in patients with biochemical signs of vitamin B12 deficiency.12
Also, low levels have been reported in vegetarians, and in subjects with low intake of vitamin B12.13,14 In addition, holoTC levels reflect vitamin B12 status, independent of recent absorption of the vitamin, and it is recommended as a better indicator of vitamin B12 status during pregnancy.15,16
Serum vitamin B12 bound to holoTC represents the fraction of total vitamin B12 that is available for tissue uptake and hence, has been proposed as a useful alternative indicator of vitamin B12 status. The objective of this study is to compare the usefulness of the determination of serum holoTC and total vitamin B12 in patients investigated for vitamin B12 disorders.
Methods
Serum samples used in this preliminary study were randomly selected from 76 patients who were admitted or followed up at Royal Hospital, Muscat, Oman, and who had been referred to the Clinical Biochemistry Laboratory, for the assessment of vitamin B12 status, during September 2007. These patients included 48 females and 28 males with an age range of 12-69 years. A variety of clinical problems/diseases were present or investigated in these patients including; anaemia, gastrointestinal diseases, autoimmune, endocrine disorders, malignancy and chronic renal failure. Two of the female subjects were pregnant. For each patient, serum total vitamin B12 level was determined by chemiluminescent microparticle immunoassay on Architect 2000 analyzer (Abbott, USA) and holoTC (active vitamin B12) level was determined by microparticle enzyme immunoassay on Axsym analyzer (Abbott, USA).
Comparison of the data was performed to test the statistical relationship as reflected by the mean, median, standard deviation and correlation coefficient.17 Also, the data was evaluated concerning any misclassification of the results. This was performed by comparing holoTC versus total vitamin B12 values, particularly in terms of whether either or both values agree or disagree for classifying the patients as being normal (results within the reference range) or abnormal (results lower or higher than the reference range). The cut-off thresholds for the data were assessed using the kit’s quoted reference range for holoTC and for total vitamin B12. The quoted between-batch coefficient of variation
(CV) for holoTC assay was 6.3-7.8%, and for total vitamin B12 assay was 4.4-6.8% at different levels of the vitamin.
RESULTS
A comparison of holoTC and total vitamin B12 are presented in Table 1. The correlation between the two parameters was examined using linear regression analysis. A significant (P< 0.001) correlation was noted with r= 0.765 and regression equation of: y = a + bx (ie: holoTC= 1.5 + 0.14 total vitamin B12). (Fig. 1)

However, in 7 (9.2%) samples, there was a disagreement/ misclassification of results. In 1 (1.4%) case, holoTC was within the reference range but total vitamin B12 was high. The patient was a nine year old boy, with acute lymphoblastic leukaemia. The laboratory findings for the patient were; serum holoTC 74.1 pmol/L (RR 9-123), total vitamin B12 685 pmol/l (RR 140-600), folate 19.0 nmol/L (RR 4.8-30.5); and Hb 8.6 g/dL, RBC 3.9 X 1012, MCV 77 fL, MCH 25 pg, MCHC 32 g/dL, RDW 21.5 %, WBC 7.4 X 199/L, neutrophil 2.7 X 199/L, platelets 365 X 199/L.
In 6 other (7.8.%) patients, holoTC was within reference range, however, total vitamin B12 was low. Their laboratory findings were as follows:
- Male, 14 years (with neutropenia). Serum holoTC 14.2 pmol/L, total vitamin B12 138 pmol/l, folate 24.9 nmol/L, ferritin 36 ug/L (RR 20-280); and Hb 11.7 g/dL, RBC 4.3 X 1012, MCV 84 fL, MCH 27 pg, MCHC 32 g/dL, RDW 13.2 %, neutrophils 0.8 X 109/L, platelets 434 X 199/L, blood film: moderate neutropenia.
- Male, 36 years (with gait problem). Serum holoTC 21.1 pmol/L,total vitamiMale, 43 years (with thrombocytopenia). Serum holoTC 13 pmol/L, total vitamin B12 137 pmol/l, folate 16.2 nmol/L, ferritin 40 ug/L; and Hb 9.4 g/dL, MCV 82 fL, MCH 28 pg, MCHC 34 g/dL, RDW 14.9 %, RBC 3.4 X 1012, WBC 29.6 X 199/L, neutrophil 25.8 X 199/L, platelets 3 X 199/L, blood film: normochromic normocytic, severe thrombocytopenia, marked neutrophilia with mild hypersegmentation
- Male, 48 years (with periodic leg movement). Serum holoTC 19.6 pmol/L, total vitamin B12 135 pmol/l, folate 26.4 nmol/L, ferritin 45 ug/L; and Hb 12.9 g%, RBC 5.5 X 1012,MCV 68 fL, MCH 22 pg, MCHC 32 g/dL, RDW 12.9 %, WBC 6.6 X 199/L, neutrophil 4.3 X 199/L, platelets 247 X 199/L
DISCUSSION
In this preliminary study, comparable results with significant correlation (r= 0.765, P< 0.001) were noted between holoTC and total vitamin B12. Using the cut-off thresholds or kits’ quoted reference range for holoTC of 9-123 pmol/L and for total vitamin B12 of 140-600 pmol/L, a parallel agreement/classification of results was noted in the majority of patients. This was evident in 90.8% of patients, who had agreement in the classification of results, both being normal or abnormal (low or high). Generally, in 80.4% of cases, both results were within the reference ranges. However, in 5.2% cases, both results were higher than the reference ranges, and also in 5.2% of cases, both results were lower than the However, in 7 (9.2%) patients (6 males and 1 female), there was disagreement or misclassification of results. Although more females (48) than males (28) were included in this comparison study, the misclassification was observed mostly among males.
Blood samples were randomly collected, and male patients who were included in the study may be more severely affected than females, otherwise there is no other explanation for this sex predominance. Also, no medication history was available for the patients. Of these seven patients, only one patient (1.4%) had holoTC of 74.1 pmol/L (within the reference range) but with high total vitamin B12 (685 pmol/l) level. The patient was a nine year old boy, with acute lymphoblastic leukaemia. The possible explanation for the raised total vitamin B12 is that, in patients with myeloproliferative disorders or liver diseases, the haptocorrin level may be high leading to high total vitamin B12, as most of the cobalamin measured is that bound to HC.6,7,18
The other six patients (5 males, 1 female) (8.4%) had normal levels of holoTC but low total vitamin B12. Following the interpretation of the data, the range of holoTC was 13-25 pmol/L while the range for total vitamin B12 was 115-137 pmol/L. holoTC levels were in the lower reference range (cut-off 9 pmol/L) while total vitamin B12 levels were moderately decreased (cut-off 160 pmol/L). There seemed to be no clear evidence of vitamin B12 deficiency (particularly from blood film examination and lack of haematological indices of hyperchromasia, macrocytosis, neurophil hypersegmentation, thrombocytopenia), however, three patients had iron deficiency anaemia. HoloTC may appear to be a better indicator of total vitamin B12 status in these few patients, although no definite conclusion can be drawn. No gold method for comparison was used in this study, as other indices such as methylmalonic acid (MMA) and homocysteine, which are not offered on a wide scale as core investigations for vitamin B12 deficiency, were not measured in this comparitive study.2,19
In this study, results with normal total vitamin B12 but low holoTC were not observed. This may be due to the random selection of the samples in this preliminary study, however, it would have been an area of interest for investigation.
More importantly and taking into consideration the agreement of the results in the majority of patients (90.8%) in this study, it can be recommended that both holoTC and total vitamin B12 have almost equal diagnostic efficiency in screening/diagnosing vitamin B12 deficiency. In a few patients and under certain circumstances, holoTC alone or in combination with total vitamin B12 may be required. Miller et al. in a comparison screening study using total vitamin B12 (at a cut-off 148 pmol/L), holoTC (at cut-off 25 pmol/L), MMA and homocysteine assays, their refults supported the diagnostic accuracy of both forms of vitamin B12, alone and in combination for screening of metabolic vitamin B12 deficiency.14
They reported that in only 5-6% of cases, holoTC explained more of the observed variance in MMA and homocysteine than did total vitamin B12, but ROC curve analysis indicated that both indices were essentially equivalent in discriminating subjects with and without vitamin B12 deficiency. They recommended that measurement of both holoTC and total vitamin B12 provides better screening for vitamin B12 deficiency than either assay alone. Also, other the evaluation of other studies that involved the measurements of holoTC, total vitamin B12, MMA and homocysteine observed that the majority of subjects with combined low holoTC and elevated MMA had normal concentrations of total vitamin B12.
They suggested that holoTC is a more sensitive marker for vitamin B12 deficiency favoring its use as a first line parameter in detecting cobalamin deficiency.20,21 Analytical studies of the different techniques that include microbiological, enzyme-labelledAgreement between serum total vitamin B12 and holoTC results were noted in the majority of patients, where a highly significant correlation was reported between the two indices. There was a disagreement in a minority of patients who had low total vitamin B12 but low-normal holoTC levels in the absence of a clear evidence of any deficiency. It can be recommended that holoTC and total vitamin B12, alone and in combination, have almost equal diagnostic efficiency in diagnosing vitamin B12 deficiency for the majority of patients. In a small number of patients, holoTC appeared to be a better reflector of vitamin B12 status. Further large-scale comparison studies based on a gold standard method for classifying vitamin B12 status are worth considering and warranted to clarify the effectiveness of holoTC in the clinical setting.
ACKNOWLEDGEMENTS
The authors reported no conflict of interest and no funding has been received on this work.
-
Davis RE. Clinical chemistry of vitamin B12. Adv Clin Chem 1985; 24: 163,216
-
Markle HV. Cobalamine. Crit Rev Clin Lab Sci 1996; 33(4): 247-356.
-
Solomon LR. Disorder of Cobalamin (vitamin B12) metabolism: emerging concepts in pathophysiology, diagnosis and treatment. Blood Rev 2007; 21(3): 113-30.
-
Hakami N, Neiman PE, Canellous GP, Lazerson J. Neonatal megaloblastic anemia due to inherited transcobalamine II deficiency in two siblings. New Engl J Med 1971; 285(21): 1163-70.
-
Nexo E, Hvas AM, Bleie O, Refsum H, Fedosov SN, Vollset SE, et al. Holotranscobalamin is an early marker of changes in cobalamin homeostasis. A randomized placebo-controlled study. Clin Chem 2002; 48(10): 1768-71.
-
Lindenbaum J, Savage DG, Stabler SP, Allen RH. Diagnosis of cobalamin deficiency II. Relative sensitivity of serum cobalamin, methylmalonic acid, and total homocysteine concentrations. Am J Hematol 1990; 34(20): 99-107.
-
Matchar DB, McCrory, Millington DS, Feussner JR. Performance of serum cobalamin assay for diagnosis of cobalamin deficiency. Am J Med Sci 1994; 308(5): 276-83.
-
Lindgren A, Kilander A, Bagge E, Nexo E. Holotranscobalamin- a sensitive marker of cobalamin malabsorption. Eur J Clin Invest 1999; 29(4): 321-9.
-
Tisman G, Vu T, Amin J, Luszko G, Brenner M, Flener V, et al. measurement of red blood cell-vitamin B12: a study of the correlation between intracellular B12 content and concentrations of plasma holotranscobalamin II. Am JHematol 1993; 43(2): 226-9.
-
Nexo E, Christensen AL, Hvas AM, Peterson TE, Fedosov SN. Quantification of holotranscobalamin, a marker of vitamin B12 deficiency. Clin Chem 2002; 48(3): 561-2.
-
Ulleland M, Eilertsen I, Quadros EV, Rothenberg SP, Fedosov SN, Sundrehagen E, et al. Direct assay for cobalamin bound to transcobalamin (holo-transcobalamin) in serum. Clin Chem 2002; 48(3): 526-32.
-
Obeid R, Jouma M, Herrmann W. Cobalamin status (holo-transcobalamin, methylmalonic acid) andHerrmann W, Obeid R, Schorr H, Geisel J. Functional vitamin B12 deficiency and determination of holotranscobalamin in population risk. Clin Chem Lab Med 2003; 41(11): 1478-88.
-
Miller JW, Garrod MG, Rockwood AL, Kushnir MM, Allen LH, Haan MN, et al. Measurement of total vitamin B12 and holotranscobalamin, singly and in combination, in screening for metabolic vitamin B12 deficiency. Clin Chem 2006; 52(2): 278-85
-
Chen X, Remacha AF, Sarda MP, Carmel R. Influence of cobalamin deficiency compared with that of cobalamin absorption on serum holotranscobalamin II. Am J Clin Nutr 2005; 81(1): 110-4.
-
Koebnick C, Heins UA, Dagnelie PC, Wickramasinghe SN, Ratnayaka ID, Hothorn T, et al. Longitudinal concentrations of vitamin B12 and vitamin B12-binding proteins during uncomplicated pregnancy. Clin Chem 2002; 48(6): 928-33
-
Hill AB, Hill ID. Bradford Hill’s Principles of Medical Statistics. 12th Ed. Hodder Arnold: London; 1991.
-
Ermens AA, Vlaveld LT, Lindemans J. Significance of elevated cobalamin (vitamin B12) levels in blood. Clin Biochem 2003; 36(8): 585-90.
-
McCaddon A, Hudson P, Ellis D, Hill D, Lloyd A. Effect of supplementation with folic acid on relation between plasma homocysteine, folate and vitamin B12. Lancet 2002; 360(9327): 173.
-
Hvas AM, Nexo E. Holotranscobalamin as a predictor of vitamin B12 status. Clin Chem Lab Med 2003; 41(11): 1489-92.
-
Obeid R, Herrmann W. Holotranscobalamin in laboratory diagnosis of cobalamin deficiency compared to total cobalamin and methylmalonic acid. Clin Chem Lab Med 2007; 45(12): 1746-50.
-
Brady J, Wilson L, McGregor L, Valente E, Orning L. Active B12: A rapid, automated assay for holotranscobalamin on the Abbott AxSYM analyzer. Clin Chem 2008; 54(3): 567-73.
-
Refsum H, Johnston C, Guttormsen AB, Nexo E. Holotranscobalamin and total transcobalamin in human plasma: determination, determinants, and reference values in health adults. Clin Chem 2006; 52(1): 129-37.
-
Morkbak AL, Heimdal RM, Emmens K, Molloy A, Hvas AM, Schneede J, et al. Evaluation of the technical performance of novel holotranscobalamin (holoTC) assays in a multicenter European demonstration project. Clin Chem Lab Med 2005; 43(10): 1058-64