
Splenic Pathology in Traumatic Rupture of the Spleen: A Five Year Study
Hunaina Al-Kindi,1 Leena Devi,2 Mina George2
Al-Kindi H, et al. OMJ. 24, 81-83 (2009); doi:10.5001/omj.2009.19
ABSTRACT
Objectives: To Study the histopathology of spleens with a history of traumatic rupture with a view to establish possible predisposing factors to the rupture
Methods: This study examined the gross and microscopic features of consecutive cases of splenectomies done for traumatic rupture during a five year period in order to evaluate the presence or absence of any pathology prior to rupture.
Results: Of the 17 cases of splenectomy during this period, 14 were normal and 3 cases showed pathology other than rupture.
Conclusion: In the five year period of studying splenic pathology in traumatic rupture, 82% of the spleens showed normal histology except for the rupture. 18% of the cases showed different pathological findings on histopathology which could have contributed to the rupture.
From the 1Department of Histopathology, Khoula Hospital, Sultanate of Oman, 2Department of Pathology, Khoula Hospital, Muscat, Sultanate of Oman.
Received: 02 Jan 2009
Accepted:16 Mar 2009
Address correspondence and reprint request to: Dr. Hunaina Al-Kindi, Department of Histopathology, Khoula Hospital, Muscat, Sultanate of Oman
E-mail: alkindihunaina@hotmail.comINTRODUCTION
Rupture of the spleen can occur sponteneously or due to trauma. The incidence of traumatic rupture of the spleen increases due to rise in automobile accidents.1 Some studies have considered spleens affected by trauma to be normal and have used such spleens as control specimen in their studies.2 On the other hand, many studies have shown that there is an increased amount of white pulp in spleens from patients with traumatic injury.2,3,5 This has led to the speculation that in many cases of traumatic rupture, there could be a predisposing factor. In order to evaluate this in detail, this study reviewed the history and records of all splenectomy specimens received at the department of histhopathology from 1st January 2003 to 31 December 2007.
METHODS
Spleens were sent to the histopathology unit at Khoula Hospital following Road Traffic Accidents (RTA) during the period of 1st January 2003 to 31st December 2007. The age and sex of the patients and type of injury were noted. Size, weight and gross examination findings of the spleens including appearance of capsules, presence of rupture, hemorrhage or hematomas as well as a description of rest of the splenic pulp etc., were also noted (table 1).
Table 1: Patients and findings
No |
Age |
Sex |
Type of injury |
Size in cm |
Wight (g) |
Gross findings |
Microscopic findings |
1 |
28 |
M |
RTA |
8 x7 x 1.5 |
100 |
Breach of capsule and hemorrhage |
Hemorrhage and neutrophilic infiltrate at the ruptured area |
2 |
63 |
M |
RTA |
6 x 3.5 x 2.5 |
40 |
Breach of capsule and hemorrhage |
Hemorrhage, Lymphoid follicle hyperplasia & amyloidosis |
3 |
31 |
F |
RTA |
Not taken |
70 |
Breach of capsule |
Hemorrhage and neutrophilic infiltrate at the ruptured area |
4 |
79 |
M |
RTA |
7 x 7.5 x 4 |
110 |
Breach of capsule and hemorrhage |
Hemorrhage and neutrophilic infiltrate at the ruptured area |
5 |
36 |
M |
RTA |
10x3x 5 |
100 |
Breach of capsule |
Hemorrhage and neutrophilic infiltrate at the ruptured area |
6 |
31 |
M |
RTA |
12x5.5 |
230 |
Breach of capsule and splenicule |
Hemorrhage and neutrophilic infiltrate at the ruptured and splenicule |
7 |
36 |
F |
RTA |
8x6x3 |
50 |
Breach of capsule |
Hemorrhage and neutrophilic infiltrate at the ruptured area |
8 |
46 |
M |
RTA |
12 x 7 x 3 |
120 |
Breach of capsule |
Hemorrhage and neutrophilic infiltrate at the ruptured area |
9 |
7 |
M |
RTA |
11 x 6 x 2.5 |
90 |
Breach of capsule |
Hemorrhage and neutrophilic infiltrate at the ruptured and prominent malpigian corpuscle |
No |
Age |
Sex |
Type of injury |
Size in cm |
Wight (g) |
Gross findings |
Microscopic findings |
10 |
4 |
M |
RTA |
8 x 7 x 2 |
50 |
Breach of capsule |
Hemorrhage and neutrophilic infiltrate at the ruptured area |
11 |
32 |
M |
RTA |
13 x 10 x 3.5 |
240 |
Breach of capsule and hemorrhage |
Hemorrhage and neutrophilic infiltrate at the ruptured area |
12 |
31 |
F |
RTA |
10 x 6 x 2.5 |
90 |
Breach of capsule and hemorrhage |
Hemorrhage and neutrophilic infiltrate at the ruptured area and granuloma with calcific material |
13 |
20 |
M |
RTA |
9 x 6 x 2.5 |
100 |
Breach of capsule, hemorrhage and well defined cream area |
Hemorrhage and neutrophilic infiltrate at the ruptured area |
14 |
35 |
F |
RTA |
10.5 x 7 x 3.5 |
120 |
Breach of capsule and hemorrhage |
Hemorrhage and neutrophilic infiltrate at the ruptured area |
15 |
27 |
M |
RTA |
6 x 5 x 2.3 |
40 |
Breach of |
Hemorrhage and neutrophilic infiltrate at the ruptured area |
16 |
25 |
M |
RTA |
9.5 x 6.5 x 3 |
110 |
Breach of capsule |
Hemorrhage and neutrophilic infiltrate at the ruptured area |
17 |
40 |
M |
RTA |
8.5 x 6 x 2.5 |
60 |
Breach of capsule |
Hemorrhage and neutrophilic infiltrate at the ruptured and small non caseating granulomas |
RTA: Road Traffic Accident; F: Female; M: Male |
|||||||
Hematoxylin and Eosin stained sections and sections with special stains, if any, were reviewed along with the given histopathology reports. Finally, an analysis of the findings was performed and was compared with the findings in published literature of similar studies.
RESULTS
During the period from 1st January 2003 to 31st December 2007, 17 cases of spleens removed for traumatic rupture were submitted for histological examination. All cases were involved in road traffic accidents. The comparatively low number of splenectomies during the 5 year period is due to the fact that most cases of blunt trauma of the abdomen are managed conservatively at the centre. 13 cases were from males and 4 cases from females. 10 of the cases were in 21-40 years age group (table 2).
Table 2: Age Incidence -17 Cases of Ruptured Spleen
Number of cases |
Age |
2 |
0-10 |
2 |
11-20 |
4 |
21-30 |
6 |
31-40 |
1 |
41-50 |
2 |
>50 |
Grossly, all 17 cases received showed breach of the capsule. In addition, 5/17 showed hemorrhage. While two cases showed perisplenitis.
Microscopically, all cases showed congestion of the red pulp and hemorrhage with neutrophilic infiltrate at the ruptured site. Multiple, small and discrete granulomas with calcified material were seen in one case. Small non-caseating granulomas were seen in another case. One case showed amyloid deposition with lymphoid follicle hyperplasia. While another case showed arteriosclerosis with calcification. In the rest of the cases, the rest of the pulp was unremarkable.
DISCUSSION
The spleen is the most commonly injured abdominal organ from non-penetrating injuries.1 Its location and anatomic features are primarily responsible for its susceptibility to injury from external forces.1 The aetiology of traumatic rupture of the spleen include automobile accidents, fall from a height or on level ground, blows and kicks, athletic injuries, gunshot wounds and others.1,3-5 The non traumatic causes of splenic rupture include; infectious mononucleosis, Acquired Immune Deficiency Syndrome (AIDS), malignancies, peliosis, granulomas and infarct.2-5
In this study, all 17 cases resulted from RTA in which the victims were either pedestrians or occupants of vehicles. The adult male in his second decade of life showed the greatest predisposition to this type of injury. The male to female ratio was 3.3:1. The age distribution and the gender follows closely to that reported in the literatures.1,4 In other studies it was found that the more physically demanding occupation and the greater exposure to trauma of young adult male accounts for these age and sex distribution.
Increased weight of the spleen was found to be an independent factor associated with rupture of the spleen.5 In this study, there was no significant increase in weight of the spleens. However, two cases showed increase in weight, clinically both patients were otherwise healthy at the time of RTA. In both cases, the histopathological findings were within normal limits except for the rupture.
Most of the spleens removed for trauma showed capsular laceration and hemorrhage. Microscopic findings included neutrophilic infiltrates at the lacerated site and in some cases, subcapsular infiltrates were also observed.6 Congestion and intraparenchymal hemorrhage were seen in most of the cases. Some studies found that the spleens removed following trauma to be normal.2 But a few other studies have shown that ruptured spleens exhibit follicular hyperplasia suggesting the possibility of immune stimulation as a predisposing factor for splenic rupture following trauma.2,3,5 This has been clearly observed in Epstein-Barr Virus (EBV) infection, a recognized cause of splenic rupture and a potent stimulator of B cell proliferation in the spleen.3 However, in this study, only one case of lymphoid follicular hyperplasia was noted in a 63 year old male which was associated with amyloidosis (figure 1).
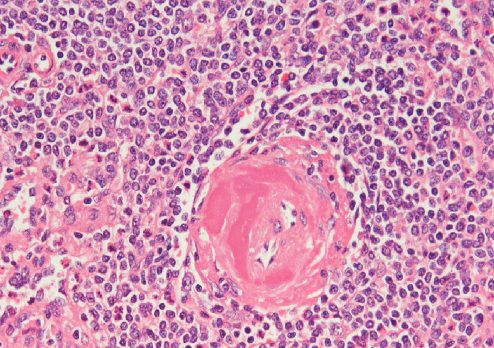
Figure 1. Spleen showing Amyloid deposition in the Blood Vessel (H&E, original magnification x 200).
This could have facilitated splenic rupture as amyloidosis has been associated with spontaneous splenic rupture especially considering the fact that the spleen was not enlarged.7 Unfortunately, there were no follow ups recorded for the patient to look into other organ involvement by amyloidosis.
Multiple small discrete granlomas with calcific material were noted in a 13 year old female (figure 2). Clinically the patient was healthy at the time of RTA and expired one week later due to hypovolemic shock and severe head injury. Small noncaseating granulomas were also noted in another case for a 40 year old male, who is doing well. Non-caseating granulomas were described previously in spleens following blunt trauma.5
Pathological findings in similar previous studies included lipogranulomas, extramedullary hematopoiesis, subintimal hyaline deposits and infarction. However, no such lesions were encountered in this study.3,5
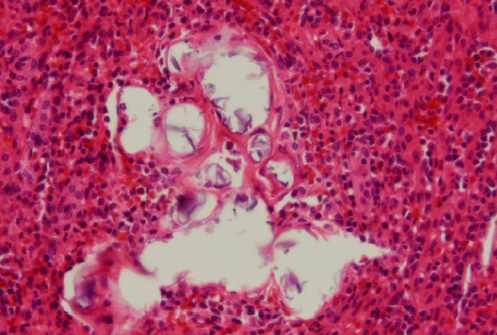
Figure 2. Discrete Granuloma with calcific material (H&E, original magnification x 400).
CONCLUSION
In the five year period of studying splenic pathology in traumatic rupture, 82% of the spleens showed normal histology except for the rupture. 18% of cases showed different pathological findings on histopathology which could have contributed to the rupture.
ACKNOWLEDGMENTS
The authors reported no conflict of interest and no funding has been received on this work.
1. Parsons L, Thompson JE. Traumatic rupture of the spleen from non-penetrating injuries. Annals of Surgery 1958; 147:214-223.
2. Barnard H, Dreef EJ, van Kriekan JHJM. The ruptured spleen. A histological, morphometrical and immunohistochemical study. Histol Histopath 1990; 5:299-304.
3. Farhi DC, Ashfaq R. Splenic pathology after traumatic injury. Am J Clin Pathol 1996; 105:474-478.
4. Gaum AR, Gaum D. Traumatic rupture of the spleen: report of 11 cases. Canad. M. A. J. 1958; 78:189-194.
5. Drachenberg CB, Papadimitriou JC. Splenic pathology in different forms of traumatic injury. Am. J. Clin. Pathol 1996; 695.
6. Rosai J. Rosai and Ackerman’s Surgical pathology. 9 ed, vol two; 2020.
7. Aydinli B, Ozturk G, Balik AA, Aslan S, Erdogant F. Spontaneous rupture of the spleen in secondary amyloidosis: a patient with rheumatoid arthritis. Amyloid. 2006; 13:160-163.