|
INTRODUCTION
Testicular ischemia and segmental infarction are rare complications of acute epididymitis. Accurate diagnosis is essential for instituting proper treatment. Doppler ultrasound is an efficient modality for assessing the serial changes in the vascularity of the testis. Lack of symptomatic improvement is a clear justification for perfoming repeat Doppler ultrasound in acute epididymitis.
CASE REPORT
A 31 year old patient presented to the emergency department with acute scrotal pain, swelling, dysuria and fever. On examination, he had a tender swelling of the right testis with preservation of cremasteric reflex. Laboratory studies were normal except for mild elevation of WBC count. Doppler ultrasound of the scrotum revealed an enlarged epididymis with increased vascularity and minimal peritesticular fluid, consistent with acute epididymitis. The testis showed normal echotexture and vascularity (Figs. 1a, b). The patient was discharged with antibiotic and analgesics.
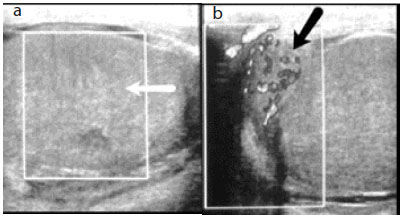
Figure 1: (a) Initial Doppler ultrasound shows minimal peritesticular fluid (arrow head). (b) Enlarged right epididymis with increased vascularity denoting acute epididymitis (white arrow) and testis showing normal vascularity (black arrow).
On the third day after admission, the patient again presented with increased scrotal pain and swelling. A repeat Doppler study showed total ischemia of the testis with slightly increased vascularity, persisting in the epididymis. (Figs. 2 a & b)
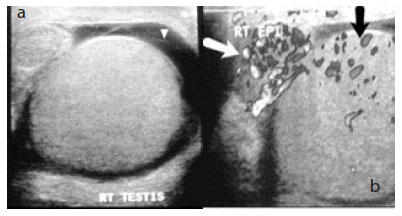
Figure 2: (a) Absent testicular flow suggestive of testicular ischemia (white arrow). (b) Hypervasular epididymis (black arrow).
Figure 3: (a) Partially regained perfusion of the testis (black arrow). (b) Irregular hypoechoic area in the upper pole of testis suggestive of segmental infarction (white arrow).
The patient was admitted and treated conservatively. On tenth day of hospital stay, he developed a tender fluctuant swelling in the right testis with associated fever and chills. Repeat Doppler ultrasound revealed an avascular hypoechoic area measuring 3x 1.8 cm in the upper pole of the testis with regained perfusion in the other parts of the testis, (Fig. 3 a, b). Immediate orchidectomy was performed and histopathological examination confirmed segmental infarction of the testis with necrosis.
DISCUSSION
Epididymitis is an inflammation limited to epididymis, seen approximately in 1 in 1000 men per year.asculitis and hematologic disorders (sickle cell disease and polycythemia).5,6,7
In the present case, the initial Doppler evaluation showed a hypervascular epididymis with normal testicular flow and a diagnosis of acute epididymitis was suggested in correlation with the clinical picture. Even though a hyper vascular epididymis is a definite sign of epididymitis, it can rarely be seen in acute torsion (up to 5%) and in case of spontaneous or manual detorsion.8
Torsion was excluded in this case by demonstration of testicular flow in the initial scan itself. Peculiar clinical course and findings in repeat Doppler also ruled out the possibility of detorsion.
CONCLUSION
This case is reported to illustrate a rare complication of acute epididymitis and to highlight the importance performing follow up Doppler ultrasound, especially when the symptoms persist in spite of treatment.
ACKNOWLEDGEMENTS
The authors reported no conflict of interest and no funding was received on this work |