
Chest Pain in A/E with ST Elevation
Kowthar Hassan
Hassan K. OMJ. 24, 308-309 (2009); doi:10.5001/omj.2009.64
From the Department of Medicine, Sultan Qaboos University Hospital, Sultanate of Oman.
Received: 16 Aug 2009
Accepted: 24 Sep 2009
Address correspondence and reprint request to: Dr. Kowthar Hassan,
Department of Medicine, Sultan Qaboos University, Sultanate of Oman.
E-mail::kowhassan@btinternet.com
A 26 year old man was presented to the accident and emergency department with
left sided chest pain. The pain started the night before at 11 pm and intesified
in the morning at around 9 am. It was pricking in nature, did not increase with
deep breathig, nor did it radiate to any where but get worse on sitting up and
sitting forward. The patient had had similar pain 2 years ago but was not
admitted to hospital at that time. On examination, he appeared to be a fit young
man, not in any respiratory distress but was holding his hand on the left side
of his chest. His pulse was 90 bpm regularly but increased to 125 bpm upon
sitting up or sitting forward. There was no pericardial rub. Chest X ray was
normal and so were the laboratory findings including erythrocyte sedimentation
rate and C-reactive protein. His electrocardiogram is shown below. 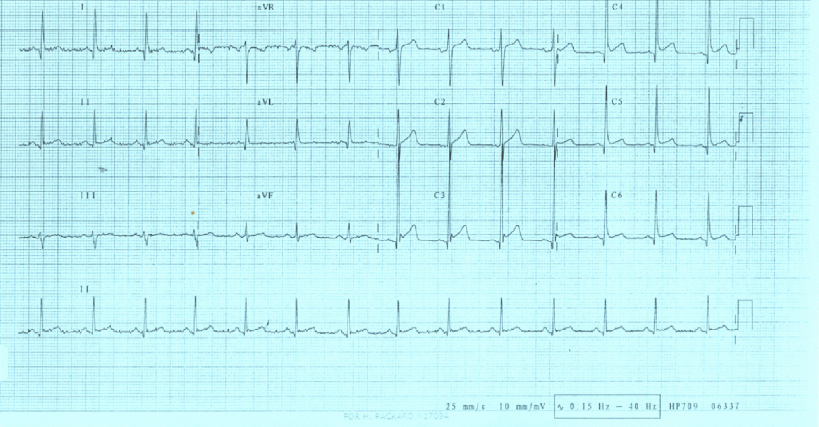
Figure 1: ECG of Patient
What is the diagnosis?
a. acute STEMI
b. acute pericarditis
c. left ventricular aneurysm
d. Brugada’s syndrome
e. none of the above
ANSWER:
None of the above.
In the emergency department, the patient was initially given aspirin 300 mg along with clopidogrel 300 mg. He was then admitted by the medical on call team as a case of acute pericarditis and was treated with a high dose ibuprofen along with omeprazole. His echocardiogram next morning was normal and he was reviewed by a cardiologist who made the diagnosis of musculoskeletal pain. Several points in the patient’s history and examination were in fact against the diagnosis of acute pericarditis although the first look at the ECG gives the impression of this diagnosis. These points are the fact that the pain was not pleuritic in nature and it was getting worse on sitting up and forward which is the opposite of the pain characteristic of acute pericarditis. Also the patient’s inflammatory markers were normal, making acute pericarditis unlikely. The high uptake of ST segment in the chest leads is consistent with the early repolarization, which is a normal variant and does not need any action but reassurance.
The normal early repolarization variant is characterized by ST elevation of the J point, which represents the junction between the end of the QRS complex (termination of depolarization) and the beginning of the ST segment (onset of ventricular repolarization). As a rsult, there is elevation of the ST segment itself, which maintains its normal configuration. ST elevation is most often present in the mind to lateral chest leads (V3-V6) although many leads can be involved.
The following features can be used to distinguish the electrographic changes in acute pericarditis from those in early reporalization:
-
ST elevations occur in both the limb abd precordial leads in most cases of acute pericarditis, whereas about one-half of subjects with early repolarization have no ST deviations in the limb leads1.
-
PR deviation and evolution of the ST and T changes, which are not seen in early repolarization.
-
The most reliable distinguishing feature was the ratio of ST elevation to T wave amplitude in lead V62. If the ratio exceeded 0.24, acute pericarditis was present (positive and negative predictive values were both 100%.
ACKNOWLEDGEMENTS
The author reported no conflict of interest and no funding was received on this work.
REFERENCES
-
Spodick DH. Differential characteristics of the electrocardiogram in early repolarization and acute pericarditis. N Engl J Med 1976;2:295: 523-526.
-
Ginzton LE; Laks MM. The differential diagnosis of acute pericarditis from the normal variant: new electrocardiographic criteria. Circulation 1982 May;65:1004-1009.